Transcription
Patient Aligned Care Teams (PACT)Demonstration Lab InitiativeResearch-Clinical Partnerships to Evaluateand Enhance VA PACT ImplementationBecky Yano, PhDRichard Stark, MD (VHA PACT Initiative)Stephan Fihn, MD, MPH (Demo Lab Coordinating Center)Judith Long, MD, MPH (VISN 4 Demo Lab)Eve Kerr, MD, MPH (VISN 11 Demo Lab)David Hickam, MD (VISN 20 Demo Lab)Lisa Rubenstein, MD, MSPH (VISN 22 Demo Lab)David Katz, MD, MSc (VISN 23 Demo Lab)VA HSR&D MeetingWashington DCFebruary 17, 2011
National Implementation ofVA Patient-Centered Medical Homes:Patient-Aligned Care TeamsRichard C. Stark, MDDirector of Primary Care Operations
Primary Care in the Veterans HealthAdministrationLargest integrated health care system in the USComprehensive electronic medical record 850 sites of Primary Care 152 Medical Centers 700 Community Based Outpatient Clinics (CBOC)4.8 million primary care patients-each assigned to an individualprimary care provider 53% in CBOCs12 million encounters/year
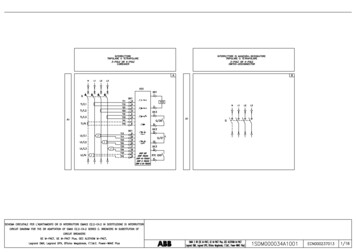
VHA Primary Care by Age & Gender44%1.46.1% FemaleMillion patients1.225%1.00.821% had encounterin Mental Health0.60.40.20.0 2525-3435-4445-5455-64AgeFemaleMale65-7475-8485-up
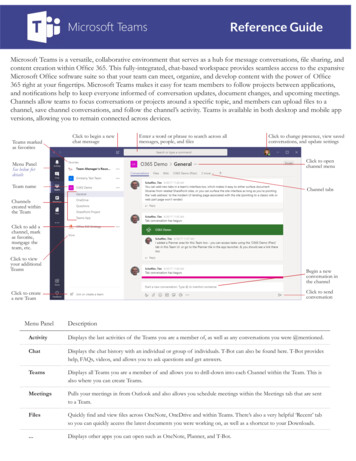
VHA Primary Care Providers7371 Providers, 5008 FTE (Avg. 0.69 FTE)PhysicianAssistant, 8%NursePractitioner20%Physician72%(5% Trainees)5
VHA Primary Care Milestones1993 Under Secretary for Health's Letter, Primary Care as a VHAPriority1994 Guidance for the Implementation Of Primary Care in VeteransHealth Administrative (VHA)1995 Primary Care in VA Primer1996 Kizer’s Vision for Change and Journey for Change1998 Guidelines for Implementation of Primary Care1998 Primary Care Management Module1999 CPRS (EMR)2004 Guidance on Primary Care Panel Size2006 Primary Care Standards2009 Universal Services Taskforce Report
VHA Primary CareStrengthsWeaknessesPrimary Care ModelTeam ConceptProvider oriented, not “patient-centered”Interdisciplinary decision making unusualSome employees not working at "top ofcompetence”Access: Delays for primary carevisits infrequentPoor phone service; secure messaging proceedingslowly; Focus on face-to-face visitsService agreementsimplemented to supportspecialty care interfaceEfforts to manage chronic disease to optimizeoutcomes still limitedSupport programs and services(Home telehealth, HBPC)Limited coordination available to manage crucialtransitions of careComprehensive ElectronicMedical RecordSub-optimal CPRS user functionalityMinimal Decision SupportPreventive Care ProgramLarge burden of chronic diseases; Poor healthbehaviors contributeHealth behaviors often not addressed andinterventions often not providedHealthcare staff need additional training
PATIENT CENTERED MEDICAL HOMEReplaces episodic care based on illness andpatient complaints with coordinated care and along term healing relationshipTakes collectiveresponsibilityfor patient careIs responsible forproviding all thepatient’s health careneedsArranges forappropriate carewith otherspecialtiesTHE PRIMARY CARE TEAM
Principles of the Medical HomePatient-DrivenTeam-BasedEfficient The primary care team is focused on the whole person Patient-preferences guide the care provided to the patient Primary care is delivered by an interdisciplinary team led by aprimary care provider using facilitative leadership skills Veterans receive the care they need at the time they need itfrom an interdisciplinary team functioning at the highest level oftheir competencyComprehensive Primary care is point of first contact for a range of medical,behavioral and psychosocial needs, fully integrated with otherVA health services and community resourcesContinuous Every patient has an established and continuous relationshipwith a personal primary care providerCommunication The communication between the Veteran patient and otherteam members is honest, respectful, reliable, and culturallysensitiveCoordinated The PCMH team coordinates care for the patient across andbetween the health care system including the private sector.
What the Evidence Indicates:Cost neutral or cost savings(modest)Decreased ED/Urgent Care visitsDecreased hospital admissionsImproved: Quality of LifeQuality of CareFunctional tyLess disparityLess Staff Burnout
Involving External Subject Matter Experts
VISN 23 Chronic Disease Model10,847 patientsOctober 2007 – August 2009COPD RR ED visits 51% RR Admissions31% Mortality per 100patient yr 10.1/ vs.13.8CHF ED visits 35% 1.02 fewer EDvisits for CHF/15months after Admissions 0.15 fewer forCHF/15 monthsafterDM HgbA1C 8.0% andLDL 100 and BP 130/80 2x usual care(22.3% vs. 10.4%)
PatientCenteredPreventionandPopulationBasedTeam mprovementData Driven,EvidenceBased
First Step: October 2009American College of Physicians Medical Home BuilderN 850 VHA Primary Care PracticesOverall Average Score: 69%
Total Score
Support Staff RatiosJanuary 2010
Other Team MembersClinical Pharmacy Specialist: 3 panelsClinical Pharmacyanticoagulation: 5 panelsSocial Work: 2 panelsNutrition: 5 panelsCase ManagersTraineesIntegrated Behavioral HealthPsychologist 3 panelsSocial Worker 5 panelsCare Manager 5 panelsPsychiatrist 10 panelsMonitored viaPrimary CareStaffing and RoomUtilization DataOther TeamMembersFor each parent facilityHealth Promotion DiseasePrevention Program Manager:1 FTEHealth Behavior Coordinator: 1 FTEMy HealtheVet Coordinator: 1 FTETeamlet: assigned to 1panel ( 1200 patients) Provider: 1 FTE RN Care Mgr: 1 FTE Clinical Associate(LPN, MA, orHealth Tech): 1 FTE Clerk: 1 FTEPatientPanel sizeadjusted(modeled) forrooms andstaffing
FundingGuidancePriority 1Teamlet StaffPriority 2Team StaffStaffing 227.7MHV 20.7ProgramSupport 25.6(Millions) 3 Teamlet members Provider RN, LPN/HT, Clerk New hires or reassignmentPriority 3ReadinessPrevention 75.0Priority 4Space Additional Team staffing: PharmD, social work, dietetics,behavioral health, Women’s Health, etc. HPDP Prog. Mgr., Health BehaviorCoord., MHV Coord.* Training and/or Travel Support VISN PCMH Lead and/or Coordinator PCMH support projects Health Promotion Disease Prevention Redesign/expand PC exam rooms Group rooms Furniture for primary care space Improve appearance of PC space* Separately funded atdesignated parent facilities
Primary Care (PCMM)National Staffing RatioSupport Staff/PC FTE2.702.602.502.402.302.202.102.00
PC Support Staff Mix14,00012,000 90 FTE10,000 339 FTE8,0006,000 430 FTE4,000 471 FTE2,0000January 2010September 2010December 2010PharmClerkLPN/MARN
tiveTraining: Mar2010LS 2:Sep 2010LS 1:June 2010SoutheastLS 4:Mar 2011LS 3:Dec 2010 Intensive training 6 Learning Sessions 18 months 250 Primary Care TeamsLS 6: Sep2011LS 5: Jun2011
Transformation Initiative Learning CentersEducation and Training1 week intensive training in:Team Function & DesignCare Management & CoordinationPatient Centered CareBegintraining:Sep 2010Train 1250PC teamsper year3750 Teamstrained after 3years
Consultation Teams5 Regional TeamsPCP, RN, Administrative lead5-6 Site visits per region per yearProvides constructive feedback andon-site teaching at request of VISNBegin site visits December 2010
Demonstration Laboratories Evaluate the effectiveness andimpacts of VHA’s PCMH model Apply robust research designsand methodsVISN 20 Different practice settingsVISN 11VISN 23 Different geographic locationsVISN 4 Develop and test innovativesolutions for the corecomponents of the PCMHmodel Evaluate solutions for effects onVISN 22 Costs Clinical outcomes Patient and provider experience
Centers of Excellence in PrimaryCare Education Puget SoundBoiseConnecticutClevelandDevelop and testinnovative approachesto prepare for PrimaryCare practice in the21st century Physician residentsStudentsAdvanced practice nurseUndergraduate nursingstudents Associated health traineesSan Francisco Utilize VA primary caresettings
PACT CompassPanel Management Panel sizePanel capacityDCGTeamlet staff FTEStaffing ratioRevisit rateNumber of new patientsAccess Desired Date appointments Same day Within 7 days Within 14 days 3rd next available Group clinic encounters Telephone clinic encounters No-show rate Telephone access data Secure messaging dataPatient Engagement andSatisfaction All-Employee survey PCsatisfaction scores SHEP scores (selected) Patient complaints (PatientAdvocate) My HealtheVet enrollment % IPACoordination Admission rate Pt contacted within 2 days ofdischarge Pt contacted within 7 days ofdischarge CCHT Enrollment Consult tracking Specialty referral ratesContinuity Provider: % visits withassigned PCP ED visit rate Team: % visits with teamClinical Improvement Admission rates ED visit rates Panel case mix Readmission rates Ambulatory Care SensitiveAdmissions Mortality
Learning, Discovery,Continuous ImprovementReadiness AssessmentStaffing Support ACP Medical Home Builder Primary Care StaffingMeasurement: PACTCompass AccessContinuityPatient Engagement/SatisfactionCoordinationPanel ManagementClinical ImprovementCenters of Excellencein Primary CareEducationTraining and Education PCMH Summit PACT Collaborative TILC (TransformationInitiative Learning Centers) Consultation TeamsDemonstration LabsIT ImprovementsCommunication PCMM enhancements CPRS enhancements Identify high risk patients Secure Messaging Staff Patients StakeholdersImplementationGuidance and Support PACT Handbook Workload capture ProtocolsPACT CertificationSpecialty Integration
PCP R OV I D E RCLERKC LINICALA S S O C I AT ERN C A R EM A NAG E RF A M I LY28
ReferencesB.D. Steiner et.al., Community Care of North Carolina: Improving Care through community health networks. Ann. Fam. Med. 2008;6:361-367Health Partners uses “BestCare” practices to improve care and outcomes, reduce costs. Institute for Health Care Improvement. Available mmaryofSuccessJul09.pdfGenesys HealthWorks integrates primary care with health navigator to improve health, reduce costs. Institute for Health Care Improvement.Available at: SummaryofSuccessJul09.pdfLeff, B., et al. Guided Care and the Cost of Complex Healthcare: A Preliminary Report. Am. Journal of Managed Care, 15 (8): 555-559GeisengerHealth System, presentation at White House roundtable on Advanced Models of Primary Care, August 10, 2009.Dorr, DA, Wilcox AB, Brunker CP., et.al., The effect of technology-supported, multidisease care management on the mortality and hospitalizationof seniors. J Am Geriatr Soc. 2008;56(12):2195-202. Findings updated for presentation at White House roundtable on Advanced Models ofPrimary Care, August 10, 2009.Boult, C. et. al., Successful Models of Comprehensive Care for Older Adults with Chronic Conditions: Evidence for Institute of Medicine’s“Retooling for an Aging America” Report. J Am Geriatr Soc 57:2328-2337, 2009.Reid, Robert G., et. al. Patient-Centered Medical Home Demonstration Am. J. Manag. Care. 2009; 15(9), e71-e87Rice, KL, et.al, Disease Management Program for Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial, American Journal ofRespiratory and Critical Care Medicine, Vol. 182. pp. 890-896, (2010).Ishani, A., et.al, Effect of Nurse Case Management Compared to Usual Care on Controlling Cardiovascular Risk Factors in Patients withDiabetes: A Randomized Controlled Trial. (In submission).Dwan, NA., et.al, Economic Evaluation of a Disease Management Program for Chronic Obstructive Pulmonary Disease, (In submission).
PACT Demo LabCoordinating Center OverviewStephan D. Fihn, MD, MPH
Demo Lab Coordinating Center MissionSupport and evaluate the VA transition toPACT through effective clinical-researchpartnerships developed by the PACT DemoLab Coordinating Center and the PACTDemo LabsOversight & coordination of PACT Demo Labs National Evaluation of PACT Implementation
Specific Objectives/GoalsDefine core measures of clinical andorganizational processes and outcomes Extract and analyze data from VA nationaldatabases to evaluate PACT implementationand report results to VA leadership Develop lab-specific metrics, to supportimplementation and evaluation of lab-initiatedorganizational and clinical programs Timely reporting of lab activities and findings
Collaborators (VA)Funding: Patient Care Services/Office of Primary CareSponsors: Richard Stark, Gordon Schectman PCS – Paul Nichol, Rachel Wiebe, Kathy Frisbee OQP – Joe Francis, Jim Shaffer, Steve Wright, MichelleLucatorto NCOD – Scott Moore, Chris Orszak HSR&D – David Atkins ORD/ORO/VA Central IRB – Lynn Cates, Tom Puglisi OI&T/Corporate Data Warehouse – Steve Anderson Systems Redesign – Mike Davies
Collaborators/Consultants(Non-VA)American College of Physicians – Michael Barr Group Health Coop. – Rob Reid, Katie Coleman Commonwealth Foundation – Melinda Abrams National Committee for Quality Assurance – SarahScholle University of Washington/Dept. of Health Services –Dan Lessler, David Grembowski, Doug Conrad, ChuckMaynard AHRQ - Janice Genevro and David Meyers
Progress to Date Matrix of candidate measures & data sources Pilot testing care mgmnt/predictive modeling Cohort definitions Coordination with learning collaboratives Full integration with PACT IT planning Exploring new measures for key domains– Pt. Experience – new CAHPS/SHEP measures– Team function
Overarching Questions Does implementing PACT improve care? Processes, outcomesVariation by type of site, type of patient?Patient experienceProvider/clinical team satisfactionWhat is the most effective way(s) to implementPACT? What are costs and savings associated with PACT? How does VA respond to new questions that ariseduring rollout?
ConstructHealth statusMeasureCurrent patient Survey of health statusBlood pressurecontrol% of adults age 18-85 years with a diagnosis of hypertension CDWand blood pressure adequately controlled ( 140/90 mm Hg)UTILIZATION/COSTSDomainDISEASE MANAGEMENTSample MeasuresData SourceSF-12 (SHEP)1LDL-C controlBlood sugar controlpercentage of adults age 18-75 years with acute myocardial CDWinfarction, coronary artery bypass graft, percutaneoustransluminal coronary angioplasty, or ischemic vasculardisease diagnosis and good LDL-C control ( 100 mg/dL)% of adults age 18-75 years with diabetes (type 1 and type 2) CDWwith good A1C control ( 9.0%)VA UtilizationEncounters per person-year by visit type (PC, specialty, ED,telephone, etc.); High cost procedures;Admissions/ReadmissionsDSS, NPCDMedicare utilizationFor dually eligible veterans: No. visits/ admissions paid byMedicare; proportion total primary/specialty care visits(VA Medicare) paid by MedicareMedicareclaims, OPC
Sample Measures – cont.PT. EXPERIENCEPROCESS OFCAREACCESS/CONTIN UITYDomainConstructAppointment wait timesMeasureData Source% of patients seen on same day (within 1 day, within 14 days) VSSCas desired appointment dateTelephone consults% of calls successfully answered within 30 secondsIPT, DaytonEmail contactsGroup visitsContinuity% of pt.generated emails responded to w/in 24 hrs.% of PCP time scheduled for any group visits% of encounters with assigned PCP, teamlet (non-providerclinical staff)VSSCPCMMStaffing ratios for effective Staffing Ratio; Staffing mix by provider type; # of unfilledteamsvacancies.PCMMMembers working to topof competencySurvey, LCdataPatient perceptions ofcontinuity andcoordination of care,quality of care, selfmanagement supportSurvey of team members compared to typical team tasks byposition typeAdd PCMH-related CAHPS questions to OQP SHEPsurvey; possibly oversample Demonstration Labs and/orspecific sub-populations. Meta-analysis of intensivequalitative work with patients at Demonstration LabsSHEP,qualitativework
Leadership: Rachel Werner MD PhD, Judith Long MD,David Asch MD
Evaluation Qualitative Process/Implementation Evaluation of the VISN Structured interviews of PCMH implementers (complete)Structured interviews of providers and staff (ongoing)Observation of PACT events (ongoing)Patient survey and focus groups (planned)Quantitative Outcome Evaluations Provider survey assessing organizational climate (complete) Evaluation of primary care provider booking density and ED use(ongoing) Quantitative measures of implementation using VISN 4 VDW (ongoing)
Interventions Clinical Innovation Pilot Projects (ongoing) Pain Care Management for the Medical HomeTelehealth in the PADRECCTargeting Specific Needs of OEF/OIF veteran with PTSD in Primary CareEngaging Caregivers in the Care of Veterans with DementiaProvider Activity Study Phase 1: Tool development (ongoing) Phase 2: Evaluation of relationship between provider activity, processmeasures, and health outcomes (planned) Phase 3: Intervention to improve provider time management(planned)
Questions We Are Addressing How are elements of PACT being defined and implementeddifferently at each site? Why? What is the result? Noted differences: nurse care manager role, pilot teamlets vs. all ofprimary care, chronic care protocols What facilitates/impedes implementation of PACT in differentsettings? Early findings: leadership, access to/understanding of performance data What are meaningful measures of PACT implementation andhow do they influence care and outcomes?How do we improve best practices through PACTs?
Key Products Tools To assess patient flow and provider productivity Validated assessments of patients with dementia for care givers Advances in Clinical Practice Using home telehealth Improving pain care management and disease specific care Enhancing provider productivity Continuous Feedback Research briefs for VISN leadership, Newsletters, Website Scientific Publications and Presentations
Key Partnerships VISN 4 Leadership David Macpherson (CMO), Michael Moreland (VISN 4 Director) Key Implementers at VISN 4 Sites Center for Health Equity Research and Promotion (CHERP) Mental Illness Research, Education and Clinical Centers (MIRECC) Performance Reporting and Outcomes Measurement toImprove the Standard of care at End-of-life (PROMISE) Center PACT Demo Lab Coordinating Center University of Pennsylvania
VISN 11 Demo LabEve Kerr, MD, MPH
VISN 11 Demo LabAnn Arbor, MIVAAAHS PATIENT-ALIGNED CARE TEAM INNOVATIONSPatient Registries:Identifying HighRisk Patients Targeted Chronic- Diabetes- Heart failure- Depression- Co-Morbidities- Chronic Pain Transitional- ED- Hospital- Nursing home Socially ComplexIDENTIFIED PATIENTSNavigator System:Patient-driven care choices Systematic assessment Menu of care programs Program recommendationsdriven by patient goals/needsHealth Care Delivery Teams Primary Care Specialty Care Home-based Primary CareFacilitated Self-MgmtSupportCare PartnersPeer to PeerTransitional Care ProgramEnhanced Management Interdisciplinary pain clinic Primary care mental health Short term intensive casemanagement MOVE/Tele-MOVE Palliative care Tele-health (CCHT)SYSTEM REDESIGNCommunicationCoordinationContinuity
VISN 11 Demo LabMajor innovations being studiedThe Navigator System
VISN 11 Demo LabKey research-clinical partnerships
VISN 11 Demo LabKey products/contributions
VISN 11 Demo LabProgress Highlights1st version of Navigator System built and tested CarePartners (IVR) program developed fordiabetes and CHF Transitional Care Program in development Focus Group Guides, Interview Guides, andSurveys developed for rigorous evaluation ofboth Veterans and staff
VISN 20 Demo LabDavid Hickam, MD, MPHMichael Alperin, MD
VISN20 Demo LabProject Setting Collaborative project among: Portland VA Medical Center (lead site) VA Roseburg Healthcare System Southern Oregon Rehabilitation Center and Clinics(White City VAMC) Evaluating implementation of PACT model in 16VA primary care clinics serving 85,000 veteransin 3 states. 10 urban/suburban clinics 6 rural clinics More than 50 teamlets
VISN20 Demo LabMajor innovations being studied Primary care transformation Effective team functioning Patient centered care Population management Care conduits Cohorts with specific chronic diseases (CHF)Integration of primary and specialty careCare management toolsPatient stratification by severityStaff competencies
VISN20 Demo LabKey research-clinical partnerships Close affiliation between research staffand primary care leadership Portland primary care operations group Key participation by top-level managers Portland Director of Primary Care Division White City Chief of Staff Roseburg ACOS/Primary Care
VISN20 Demo LabKey products/contributions To clinical care improvement Unified care plan for CHF Scripts and templates for use by teamlets Registry tool Built on successful model of diabetes registry Adaptable to multiple diseases To research/implementation science Needs assessment Define variation across clinics about facilitators/barriers Insight into change management
VISN20 Demo LabProgress Highlights High level of integration of Demo Lab staff inplanning activities for primary care.High rates of participation by primary care staffin focus groups and interviews.Care management tools successfully prototyped.Full specification of registry tool.Construction of longitudinal database. Time series analyses for disease-specific measures 5 years of baseline data for all clinics
VISN 22 Demo LabLisa V. Rubenstein, MD, MSPH
VAIL Overarching Goal Stimulate, prioritize, structureand supportPACT-related innovation development indemonstration sites Organized local innovation development using QIscience tools & VAIL technical support Evidence introduced at multiple points Spread successful innovations regionally and nationally
Innovation: PACT Can a QI research/clinical partnershipenhance PACT success? Uses evidence-based quality improvement(EBQI) VISN 22 Interdisciplinary Steering Committee Interdisciplinary quality councils at eachdemonstration practice Cross-medical center technical workgroups
PartnershipsVISN 22 interdisciplinary leadership Loma Linda, San Diego, and VA Greater LosAngeles Health Systems One demo practice per system this year, two nextyear, and ad lib the following yearCoordinating Center Health services researchers/clinicians in VISNs 2,6, 17 and 18 participating in pilot testing VAILevaluation instruments
Expected Clinical Products/Contributions Toolkits, verified/validated in two to three sites,incorporates/builds on national tools Basic PACT implementation tool kit Successful Innovations tool kits (e.g., potentiallyMyHealtheVet enrollment, detecting medication adherence,teamlet report cards) Integration of existing V22 registry into routinePACT careInterdisciplinary leadership & QI cultural changemethods
Key Expected KnowledgeProducts/Contributions Does ongoing research/clinical partnershipenhance PACT implementation? Qualitative investigation of teamletsHealthcare provider and staff surveyEconomic evaluation (with HERC)Electronic quality measures, including mental healthImplementation/process evaluation
VISN 23 Demo LabDavid Katz, MD, MSc
VISN 23 Demo Lab Evaluation includes 5 states in VISN 23 30 PACT Teams in VAMCs and CBOCs 22 PACT Teams in VISN 23 Learning Collaborative 8 PACT Teams in Central Region Learning Collaborative Demo Lab activities organized around 5 cores Secondary Analysis and BiostatisticsFormative and Team EvaluationBehavioral HealthSurvey Development & AdministrationEvidence Synthesis
VISN 23 Demo LabMajor innovations being studiedHow does implementation of PACT affects the work rolesof team members? Can a “Community of Practice” collaborative supportPACT nurses during role transitions? How to improve information exchange between PACTand private providers for co-managed veterans? What is the relationship between key attributes of PACTmodel and quality of care? What are the preferences of PACT patients regarding selfmanagement of chronic disease?
VISN 23 Demo LabKey research-clinical partnershipsMidwest Rural Health Resource Center Collaboration on issues related to PACT implementationin rural settings VISN 23 Primary Care Service Line Direct implementation efforts related to PACT VISN 23 and Central Region PACT Learning Collaboratives Provide access to PACT teams and materials Feedback from the Demo lab will be provided to thePACT teams
VISN 23 Demo LabKey products/contributions Patient care Tailoring self-management of chronic disease based onpatient preferences Improving co-management of veterans Optimizing PACT model in rural settings Implementation science Understanding of the impact of PACT implementationon providers’ roles Exploring relationships between different team functionmeasures and outcomes Identifying best practices for implementing the PACTmodel in a variety of primary care settings
VISN 23 Demo LabProgress Highlights Completed an in-depth formative evaluation of the Grand Island, NEPACT (started in 2008)Collected baseline measurement of PACT provider perceptions oftheir work environmentConducting telephone interviews with PACT providers and pilotingof telephone-based diary programConducting systematic reviews of PCMH-related literature to informimplementationDeveloping a registry of VISN 23 PACT teams and tracking patientoutcomes during follow-upConducting an analysis of VISN 23 patient survey data during PACTimplementation.
VA HSR&D Meeting Washington DC February 17, 2011. National Implementation of . Genesys HealthWorks integrates primary care with health navigator to improve health, reduce costs. Institute for Health Care Improvement. . Lab Coordinating Center and the PACT