Transcription
Ultrasound inObstetrics andGynecologyA Practitioner’s GuideKATHRYN A. GILL
Ultrasound inObstetrics andGynecologyA Practitioner’s GuideKathryn A. Gill, MS, RT, RDMS, FSDMSProgram Director, Institute of Ultrasound DiagnosticsSpanish Fort, Alabama
ivdddddcdvb fnmjk,ujmazzCopyright 2014 by Davies Publishing, Inc.All rights reserved. No part of this work may be reproduced, stored in a retrieval system, or transmittedin any form or by any means, electronic or mechanical, including photocopying, scanning, and recording,without prior written permission from the publisher.Davies Publishing, Inc.Specialists in Ultrasound Education,Test Preparation, and ContinuingMedical Education32 South Raymond AvenuePasadena, California 91105-1961Phone 626-792-3046Facsimile 626-792-5308e-mail ichael Davies, PublisherSatori Design Group, Inc., DesignCharlene Locke, Production ManagerChristina J. Moose, Editorial DirectorJanet Heard, Manuscript ManagementChristian Jones, Production EditingDaniel Liota, Digital MediaGina Caprari, Editorial AssociateStephen Beebe and Jim Baun, IllustrationNotice to Users of This Publication:In the field of ultrasonography, knowledge, technique, and best practices are continually evolving. With new research anddeveloping technologies, changes in methodologies, professional practices, and medical treatment may become necessary.Sonography practitioners and other medical professionals and researchers must rely on their experience and knowledgewhen evaluating and using information, methods, technologies, experiments, and medications described herein, alwaysremaining mindful of their own, their patients’, their coworkers’, and others’ safety and well-being.Regarding any treatments, procedures, technologies, and/or pharmaceutical products identified, users of this publicationare advised to check the most current information provided by product manufacturers and professional societies to verifytheir latest recommendations regarding methodologies, dosages, timing of administration, practice guidelines, standardsof care, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge oftheir patients, to report, make recommendations, and work within these standards, in consultation with other clinicianssuch as referring and supervisory physicians, to determine to take all appropriate safety procedures and to determine thebest treatment of each individual patient.To the fullest extent of the law, neither Davies Publishing, Inc., nor the authors, contributors, reviewers, or editors assumeany liability for any injury and/or damage to persons or property as a matter of products liability, negligence, or otherwise,or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.Library of Congress Cataloging-in-Publication DataGill, Kathryn A., author.Ultrasound in obstetrics and gynecology : a practitioner’s guide / Kathryn A. Gill.p. ; cm.Includes bibliographical references and index.ISBN 978-0-941022-80-4 (hardcover : alk. paper) — ISBN 0-941022-80-3 (hardcover : alk. paper)I. Title.[DNLM: 1. Ultrasonography, Prenatal. 2. CongenitalAbnormalities—ultrasonography. 3. Genital Diseases,Female—ultrasonography. 4. Pregnancy Complications—ultrasonography. WQ ed and bound in ChinaISBN 0-941022-80-3
viiContributorsKathryn A. Gill, MS, RT, RDMS, FSDMSProgram DirectorInstitute of Ultrasound DiagnosticsSpanish Fort, AlabamaJim Baun, BS, RDMS, RVT, FSDMSClinical Consultant and EducatorProfessional Ultrasound ServicesSan Francisco, CaliforniaJoe Rodriguez, RT, RDMSSupervisorUltrasound DepartmentSoutheast Missouri HospitalCape Girardeau, MissouriMisty H. Sliman, BS, RT(R)(S), RDMSAdjunct InstructorAmerican InstituteReviewersGeorge Bega, MDJim Baun, BS, RDMS, RVT, FSDMSAdjunct Assistant Professor of Obstetrics and GynecologyDepartment of Obstetrics and GynecologyThomas Jefferson UniversityPhiladelphia, PennsylvaniaClinical Consultant and EducatorProfessional Ultrasound ServicesSan Francisco, CaliforniaPamela M. Foy, MS, RDMS, FSDMSImaging Manager and Clinical InstructorDepartment of Obstetrics and GynecologyClinical Assistant ProfessorSchool of Health and Rehabilitation SciencesThe Ohio State UniversityColumbus, OhioGeorge Koulianos, MD, FACOGDirectorThe Center for Reproductive MedicineMobile, AlabamaDaniel A. Merton, BS, RDMS, FSDMS, FAIUMClinical Instructor and Technical Coordinatorof ResearchThe Jefferson Ultrasound Research and Education InstituteDepartment of RadiologyThomas Jefferson University HospitalPhiladelphia, PennsylvaniaBryan T. Oshiro, MDVice ChairmanDepartment of Obstetrics and GynecologyMedical DirectorPerinatal InstituteLoma Linda University Medical Center/Children’s HospitalLoma Linda, CaliforniaNirvikar Dahiya, MDDirector—UltrasoundAssistant Professor—RadiologyMallinckrodt Institute of RadiologyWashington University Medical SchoolSt. Louis, MissouriPamela M. Foy, MS, RDMS, FSDMSImaging Manager and Clinical InstructorDepartment of Obstetrics and GynecologyClinical Assistant ProfessorSchool of Health and Rehabilitation SciencesThe Ohio State UniversityColumbus, OhioCatheeja Ismail, RDMS, EdDDirector—Sonography ProgramThe George Washington UniversityWashington, DCDarla J. Matthew, BAS, RT, RDMSProgram Director and Associate ProfessorDiagnostic Medical SonographyDoña Ana Community CollegeLas Cruces, New MexicoSusan Nager, BS, RDMSDiagnostic Medical Ultrasound InstructorCentral Florida InstituteOrlando, Florida
viiiReviewers (continued)Regina Swearengin, BS, RDMSDepartment Chair, SonographyAustin Community CollegeAustin, TexasJill D. Trotter, BS, RT(R), RDMS, RVTDirector, Diagnostic Medical Sonography ProgramVanderbilt University Medical CenterNashville, TennesseeEllen T. Tuchinsky, BA, RDMS, RDCSDirector of Clinical EducationDiagnostic Medical Sonography ProgramLong Island UniversityBrooklyn, New YorkKerry E. Weinberg, MA, MPA, RT(R), RDMS,RDCS, FSDMSDirector and Associate ProfessorDiagnostic Medical Sonography ProgramLong Island UniversityBrooklyn, New Yorkdddddcdvb fnmjk,ujmazzdddddcdvb fnmjk,ujmazz
xiiiContentsContributors viiReviewers viiPreface ixAcknowledgments xiChapter 1 Introduction to Diagnostic Ultrasound 1Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives1The Advantages and Disadvantages of Diagnostic UltrasonographyInformation ProvidedScan Planes, Body Orientations, and LabelingCharacterizing TissueArtifacts12357Characterizing MassesClinical Data911Transducer Formats11Transducer Manipulation 12Introduction to Transvaginal Technique 14Starting Out22References22Self-Assessment Exercises23Chapter 2 Gynecology 25Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives25Pelvic Anatomy and Physiology 25Congenital Pelvic AnomaliesUterine PathologyAdnexal Pathology404356Incidental Pathology and Miscellaneous RequestsScanning Tips, Guidelines, and PitfallsReferences748385Self-Assessment Exercises85Chapter 3 The First Trimester 89Misty H. Sliman, BS, RT(R)(S), RDMS, and Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives89Fertilization and Pre-Embryonic Development 90The Endometrium and Gestational Sac92
xivCONTENTSEmbryonic DevelopmentFetal Development98dddddcdvb fnmjk,ujmazz98Pregnancy Tests and Human Chorionic GonadotropinComplications of Early Pregnancy102Scanning Tips, Guidelines, and PitfallsReferences101113115Self-Assessment Exercises115Chapter 4 The Second and Third Trimesters: Basic and Targeted Scans 119Joe Rodriguez, RT, RDMS, Kathryn A. Gill, MS, RT, RDMS, FSDMS, and Misty H. Sliman, BS, RT(R)(S), RDMSObjectives119Part 1: The Basic Scan 120Part 2: The Targeted Scan140Scanning Tips, Guidelines, and PitfallsReferences169175Self-Assessment Exercises176Chapter 5 The Placenta and Umbilical Cord 179Jim Baun, BS, RDMS, RVT, FSDMS, and Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives179Early Placental Development179Amniotic Bands and Sheets 182Placental Anatomy and Physiology184Placental Circulation and Hemodynamics186Placental Location 188Placental Grading 188Fibrin Deposition 190Placental Variants 192Cord Abnormalities 200Scanning Tips, Guidelines, and PitfallsReferences208211Self-Assessment Exercises212Chapter 6 Ultrasound of the Cervix during Pregnancy 215Pamela M. Foy, MS, RDMS, FSDMSObjectives215Anatomy216Cervical Length Measurements 216Cervical Incompetence 218Cerclage218Preterm Labor and Premature Birth 219Cervical Pregnancy 222Technique 222Scanning Tips, Guidelines, and PitfallsReferences225Self-Assessment Exercises227225
CONTENTSChapter 7 Anomalies Associated with Polyhydramnios 229Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives229Polyhydramnios229Neural Tube Defects230Scanning Tips, Guidelines, and PitfallsReferences261262Self-Assessment Exercises263Chapter 8 Anomalies Associated with Oligohydramnios 267Joe Rodriguez, RT, RDMS, and Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives267Oligohydramnios268Associated Anomalies: “DRIP” 270Addendum: The Fetal Biophysical ProfileScanning Tips, Guidelines, and PitfallsReferences284286287Self-Assessment Exercises288Chapter 9 Multiple Gestations and Their Complications 291Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives291Risk FactorsZygosity291292Chorionicity and AmnionicityFetal Presentations296Growth DisturbancesVanishing TwinFetal Demise293296298298Congenital Anomalies298Complications Specific to Monozygotic/Monochorionic TwinsSonographic Management306Scanning Tips, Guidelines, and PitfallsReferences299307309Self-Assessment Exercises309Chapter 10 Maternal Disorders and Pregnancy 313Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives313Supine Hypotensive Syndrome313Hyperemesis Gravidarum 314Pregnancy-Induced HypertensionChronic HypertensionHydrops314316316Diabetes Mellitus and PregnancyThyroid Disease328Adnexal Masses328319xv
xviCONTENTSOther Disorders 330dddddcdvb fnmjk,ujmazzScanning Tips, Guidelines, and PitfallsReferences331332Self-Assessment Exercises332Chapter 11 Fetal Syndromes 335Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives335Risk Factors 337Biochemical Markers for Genetic Screening338Facial Deformities 339Echogenic Bowel 344Hand and Foot Deformities344Aneuploidy 347Turner Syndrome 357Meckel Syndrome 358Prune Belly Syndrome 359Beckwith-Wiedemann Syndrome360Pentalogy of Cantrell 361Caudal Regression Syndrome 362Sirenomelia362Fetal Alcohol Syndrome 363Amniotic Band Syndrome 363Holt-Oram Syndrome 365Scanning Tips, Guidelines, and PitfallsReferences365367Self-Assessment Exercises368Chapter 12 Doppler Applications in Obstetric and Gynecologic Sonography 371Jim Baun, BS, RDMS, RVT, FSDMSObjectives371Physical Foundation of Doppler UltrasoundClinical Utility of Doppler Ultrasound372374Gynecologic Applications 378Obstetric Applications 382Scanning Tips, Guidelines, and PitfallsReferences391392Self-Assessment Exercises392Chapter 13 Infertility 393George Koulianos, MD, FACOG, and Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives393Gynecologic Factors in Infertility394Ultrasound Imaging and Laboratory Tests 394Ovulatory Factors 397Assisted Reproductive Technology402Scanning Tips, Guidelines, and PitfallsReferences408Self-Assessment Exercises409407
CONTENTSChapter 14 Volume Sonography 411George Bega, MD, and Daniel A. Merton, BS, RDMS, FSDMS, FAIUMObjectives411Introduction411Technology and Data AcquisitionObstetric Applications412416Gynecologic Applications426Volume Color Flow Sonography433Networking with Volume Sonography435Volume Sonography Artifacts, Limitations, and PitfallsScanning Tips, Guidelines, and PitfallsReferences435436437Self-Assessment Exercises441Chapter 15 Invasive Procedures 443Bryan T. Oshiro, MD, and Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives443Amniocentesis443Chorionic Villus SamplingAmnioreductionAmnioinfusion446446447Fetal Blood Sampling447Intrauterine Fetal Transfusion450Minimally Invasive Fetal Surgery451Scanning Tips, Guidelines, and PitfallsReferences452453Self-Assessment Exercises454Chapter 16 The Sonographer’s Role in the Grieving Process 457Kathryn A. Gill, MS, RT, RDMS, FSDMSObjectives457The Terminology of GriefGrief Support458462Applying Theory to Everyday PracticeCase StudiesReferences463466470Self-Assessment Exercises470Appendix A: Frequently Referenced Measurements 473Appendix B: AIUM Practice Guidelines 511Appendix C: Clinical Data Sheets 531Appendix D: Glossary 543Appendix E: Application for CME Credit 587Appendix F: Answers to Self-Assessment Exercises 607Index 619xvii
CHAPTER1Introduction toDiagnostic UltrasoundKathryn A. Gill, MS, RT, RDMS, FSDMSOBJECTIVESAfter completing this chapter you should be able to:1. Explain the advantages and limitations of B-modeultrasound imaging.2. Describe how the body is imaged in two dimensions.3. List the sonographic criteria necessary to characterizea mass as cystic, solid, or complex.4. Identify sonographic artifacts and describe theirappearance.5. Explain the relative advantages and disadvantagesof the sector, linear, and curved (convex) lineartransducers.6. Demonstrate the various maneuvers used tomanipulate the ultrasound transducer.7. Describe the correct way to hold the transducerwhile scanning a patient.B-mode (brightness mode) diagnostic ultrasound imagingprovides a dynamic means of evaluating soft-tissuestructures of the pelvis and pregnant uterus in crosssection. Although the technique of performing diagnostic ultrasound procedures appears effortless, diagnosticultrasound is one of the most difficult imaging modalities to perform and interpret. Because the inexperiencedpractitioner can make normal anatomy look abnormal,practitioners must be able to recognize normal patternsbefore they can appreciate pathology. To help simplifythe learning process, this chapter introduces some ofthe basic concepts and terms used among sonographers,focusing on two-dimensional B-mode imaging. Doppler concepts and applications are addressed elsewhere,including Chapter 12.THE ADVANTAGES AND DISADVANTAGESOF DIAGNOSTIC ULTRASONOGRAPHYAdvantagesDiagnostic ultrasonography has several advantages overother imaging modalities. In most cases, the sonographicexam is easily tolerated by patients. For evaluating thepelvic area transabdominally, the only required preparation is that the patient has a full urinary bladder. Thereis usually no need for elaborate bowel preparation, noris it necessary to introduce contrast agents in order toimage soft-tissue organs, as is required for other radiologic procedures. Since the images are produced by usinghigh-frequency sound waves, the patient is not exposedto radiation. To date, no adverse human biologic effects1
2CHAPTER 1Introduction to Diagnostic Ultrasounddddddcdvbhave been demonstrated at the frequencylevelsfnmjk,ujmazzused indiagnostic ultrasound. Cross-sectional imaging allows usto easily identify anatomic relationships among organsand other structures and to appreciate depth relationships. Most diagnostic ultrasound systems are portable,and so imaging is not restricted to one department orroom. Finally, diagnostic ultrasound procedures are costand time-efficient compared to other imaging modalities(Box 1-1).Box 1-1.Nevertheless, sonographic characteristics can suggestthat a mass is benign or has a high-risk potential for being malignant.INFORMATION PROVIDEDDiagnostic ultrasound provides information about thesize, shape, echo pattern, and position of organs andother structures. The sonographer knows the normalpatterns of all the pelvic organs, including shape, contour,Advantages of B-modediagnostic ultrasonography.Patient tolerates it wellNo bowel preparation is necessaryRelatively noninvasiveNo radiation to patientAnatomic relationships are clearly shownDepth relationships are agesThere are only a few disadvantages to diagnostic ultrasound imaging (Box 1-2). The physics of sound propagation limits the usefulness of ultrasound somewhat inevaluating dense, calcified structures (Figure 1-1) andair-filled organs such as the gastrointestinal tract (Figure 1-2). These structures cause total reflection of theultrasound and inhibit the sound from penetrating theanterior surface of the structure. In addition, B-modediagnostic imaging—as distinct from Doppler ultra sonography—does not provide adequate informationabout function, because the organ, if present, is imagedwhether it functions or not. Although efforts are beingmade through research to improve tissue characterization with ultrasound, the modality is not sensitiveenough to distinguish benign from malignant tissue.Box 1-2.Figure 1-1. Transverse image through a uterus with a calcifiedfibroid demonstrating a shadow (arrows) produced from the fibroid.U uterus, B bladder, F fibroid.Disadvantages of B-modediagnostic ultrasonography.Limited applicationsInability to determine functionInability to distinguish benign from malignantFigure 1-2. Longitudinal image of an ovary with some shadowingposterior to it from intestinal gas (arrow). B bladder, O ovary.
Introduction to Diagnostic Ultrasound texture, and internal architecture and relative position.Any disruption of the normal patterns suggests an anomaly, or abnormality. When a mass is discovered withinor adjacent to an organ, the practitioner should attemptto characterize the mass and determine its origin. To ascertain the size of pelvic organs so they can be comparedto normal, measurements are taken in three dimensions.The three measurements include longitudinal, transverse,and anterior/posterior (AP) dimensions (Figure 1-3).APXXXXLCHAPTER 1SCAN PLANES, BODY ORIENTATIONS,AND LABELINGThere are two basic scan planes used in diagnostic ultrasound imaging. They are longitudinal (or sagittal) andtransverse.Scan PlanesIn longitudinal (sagittal) imaging, the patient’s supinebody is divided into right and left sections. An imaginaryline down the midline is referred to as mid-sagittal (seeBox 1-3). The longitudinal (sagittal) image is viewed asthough the practitioner were looking at the patient fromher right side. On the ultrasound monitor, the patient’shead (cephalic) is on the left side of the screen and herfeet (caudal) on the right. The top of the screen is theanterior aspect and the bottom of the screen is posterior(Figures 1-4 A and B).Box 1-3.Longitudinal/sagittal landmarksand their abbreviations.M or ML—midline (mid-sagittal)R—to the rightTL—to the leftFigure 1-3. Anatomic drawing demonstrating how to measure anorgan or mass in the longitudinal (L), transverse (T), and anterior/posterior (AP) dimensions.ABFigure 1-4. A Drawing showing how the body is viewed in thelongitudinal plane. B Image showing transducer placement onabdomen of a pregnant patient for longitudinal imaging. (Figurecontinues . . . )3
4CHAPTER 1Introduction to Diagnostic UltrasoundCDdddddcdvb fnmjk,ujmazzFigure 1-4, continued. C Drawing showing how the body is viewed from the transverse plane.D Image showing transducer placement on the abdomen of a pregnant patient demonstrating thetransverse orientation. Compression maneuver is also demonstrated.Transverse plane imaging visualizes the patient as thoughshe were bisected by an imaginary horizontal line acrossthe waistline into superior and inferior sections (see Box1-4). The image is viewed as though you were lookingat your patient from her feet. On the ultrasound monitor, the patient’s right side is on the left side of the screenand her left side on the right. The anterior and posterioraspects are unchanged from that of the longitudinal plane(Figures 1-4 C and D). The symphysis pubis describesthe line of the union of the bodies of the pelvic bones inthe median plane, and the iliac crest or transcrestal planedescribes the transverse plane at the level of the top of thepelvic bones.Finally, an oblique scan plane is any plane that is notlongitudinal (sagittal), coronal (A/P), or transverse.Ultrasound has the unique ability to create any type ofoblique plane, as the transducer is in the operator’s hand.This also makes it imperative to have good knowledge ofsonographic anatomy in all planes.The coronal plane divides the patient’s body into frontand back portions. When scanning in this plane in thelong axis, the top of the image would be the lateral aspect,the bottom of the screen would be medial, the right sideof the screen would be inferior (caudal), and the leftwould be superior (cephalic). The sonographer has to indicate whether he or she is scanning from the right lateralapproach or the left lateral approach.Proximal: Closer to the point of reference, the origin, etc.Body OrientationsOther useful terms related to scan planes and body orientations include:Medial: Toward the center line of the body.Lateral: Away from the center line of the body.Distal: Farther away from the point of reference, theorigin, etc.Superior: Above; toward the head; generally interchangeable with “cephalad.”Inferior: Below; toward the feet or “caudal.”Superficial: Closer to the surface/skin.Deep: Farther down from the surface/skin.Box 1-4.Transverse landmarks andtheir abbreviations.S or SP—symphysis pubisIC/TCP—iliac crest/transcrestal planeU—umbilicus1 5 superior movement2 5 inferior movementLabeling and DocumentationImages should be labeled accurately for documentationpurposes. Labeling of scans may vary according to departmental protocols. Some departments choose simply tolabel images by organ, as demonstrated in Figures 1-5 Aand B. Others may label by plane (Figure 1-5C). Guidelines suggested by the American Institute of Ultrasoundin Medicine (AIUM) and other laboratory accrediting
Introduction to Diagnostic Ultrasound ATable 1-1.CHAPTER 1Ultrasound labeling guidelinesand examples.Labeling GuidelineExamplesOrgan/area of interestOvary (ov)Plane/axisLongitudinal (lg-long-ln-sag)Patient positionLeft lateral decubitus (LLD)organizations recommend at the very least that imagesindicate (1) the organ or area of interest, (2) the planeor axis, and (3) the patient’s position if it is other thansupine (Table 1-1). Whichever labeling protocol youchoose, be consistent and as specific as possible.BCHARACTERIZING TISSUEThe descriptive terms used in diagnostic ultrasound helpus to characterize the texture and density of tissues. If astructure has many echoes within it, we call it echogenic.Echoes that are exaggerated and extremely bright arereferred to as being hyperechoic (Figure 1-6A), whichusually suggests either a very solid, dense structure orthe phenomenon of echo enhancement due to the soundbeam passing through a fluid component (Figure 1-6B),as described below. Hypoechoic describes a structure thatis solid but has low-level echoes within it, while anechoicdenotes a structure without echoes (Figure 1-7). Echopenic describes a mass that has a few low-level echoes but isCAFigure 1-5. A Longitudinal scan through a normal uterus (Ut uterus, Bl bladder). B Transverse scan through a normal uterus(Ut uterus, Bl bladder, Ov ovary). C Longitudinal scan througha complex left adnexal mass (calipers; Bl bladder, M mass).Figure 1-6. A Longitudinal transvaginal image demonstratinga hyperechoic endometrium (arrow). (Figure continues . . . )5
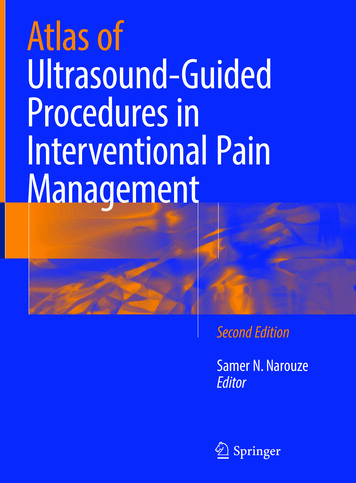
12CHAPTER 1Introduction to Diagnostic Ultrasounddddddcdvb fnmjk,ujmazzTRANSDUCER MANIPULATIONTaming the transducer is one of the sonographer’s greatest challenges. Good scanning technique requires eyehand coordination and a lot of practice.ATerms used in describing transducer manipulationinclude sliding, rocking, tilting or angling, rotating, andcompression: Sliding refers to gross movement of the transducerfrom one location to another and can be done in anydirection (Figure 1-19). Rocking the transducer toward or away from an indicator makes it possible to center the point of interestor actually to extend the field of view in one direction.Another term for this is in-plane motion, as it allowsfor visualization of more anatomy in the original planeslice (Figure 1-20).BCADBEFigure 1-19. A, B Sliding the transducer from midline to themiddle of the right costal. Reprinted with permission from Gill KA:Abdominal Ultrasound: A Practitioner’s Guide. Philadelphia, Saunders, 2001.Figure 1-20. A, B Rocking the transducer. C–E Images demonstrating the in-plane rocking motion. Reprinted with permission fromGill KA: Abdominal Ultrasound: A Practitioner’s Guide. Philadelphia,Saunders, 2001.
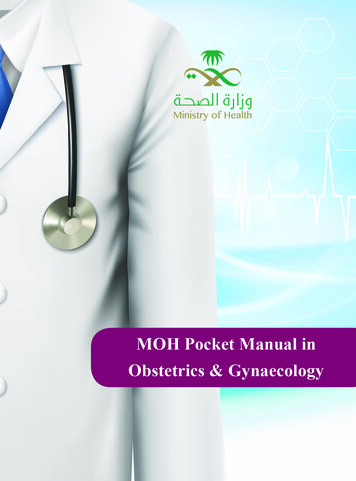
Introduction to Diagnostic Ultrasound Tilting or angling the transducer from side to side(also known as cross-plane motion) makes it possible to visualize other planes in the same axis. One canevaluate an entire organ by sweeping through it fromside to side and from top to bottom because the sweepis perpendicular to the visualized plane (Figure 1-21). Rotating the transducer from the 12 o’clock to the 9o’clock position while holding the transducer in theproper longitudinal plane results in an image of thetransverse plane. Rotation of the transducer off ofthe true longitudinal or transverse plane results in anoblique view (Figure 1-22). CHAPTER 1The compression maneuver—gently pressing downwith the transducer—may be used to displace bowelgas, compress adipose tissue, separate structures,or determine tissue response. When compression isutilized, it should be done gradually and always withconsideration of the patient’s comfort (Figure 1-23).AABBCFigure 1-21. A Tilting the transducer. B Demonstration of thetransducer being tilted cross plane down toward the patient’s feet.Figure 1-22. A, B Rotating the transducer. C Image of a patientin the left lateral decubitus position with the transducer rotatedcounterclockwise from the longitudinal into the right costal margin.Reprinted with permission from Gill KA: Abdominal Ultrasound: APractitioner’s Guide. Philadelphia, Saunders, 2001.13
14CHAPTER 1Introduction to Diagnostic Ultrasoundobtained with the traditional transvesical approach. Because transvaginal sonography relies on higher-frequencytransducers (5–7.5 MHz), tissue resolution is improved.The transducer is placed immediately adjacent to thepelvic structures, and therefore there is no need for greatdepth penetration to image through abdominal wall, fat,and bowel. Large obese patients and those with thick scarring from previous operations are no longer the challengethey once were. The endometrium and fundal region ofthe retroflexed uterus can be better imaged as the soundbeam can be angled so that it is more perpendicular tothe anatomy (Figure 1-24). Products of conception can bedddddcdvb fnmjk,ujmazzFigure 1-23. Compression is applied by gently pushing down onthe transducer and applying pressure evenly across the entire lengthof the transducer. Reprinted with permission from Gill KA: AbdominalUltrasound: A Practitioner’s Guide. Philadelphia, Saunders, 2001.ASee “Transducer Insertion and Manipulation” in the following introduction to transvaginal technique for additional techniques of probe manipulation used in transvaginal studies.INTRODUCTION TO TRANSVAGINALTECHNIQUEFirst a note on terminology. The terms transvaginal andendovaginal are commonly used interchangeably. So tooare the terms transabdominal (through the abdominalwall) and transvesical (through the urinary bladder). For Binstance, one might say, “A transvesical ultrasound examination is performed before an endovaginal examinationin order to evaluate the entire pelvis.” One might also usethe equivalent statement, “A transabdominal ultrasoundexamination is performed before a transvaginal examination in order to evaluate the entire pelvis.” Transabdominal and transvesical examinations both use the anteriorapproach, while the transvesical examination specificallyutilizes the full urinary bladder as an acoustic window.Sometimes we do perform transabdominal examinationswhen the urinary bladder is empty. Nevertheless, it iscommon for ultrasound practitioners to use these termsinterchangeably.AdvantagesTransvaginal sonography is an excellent complement tothe transabdominal pelvic evaluation because it can provide additional information that in many cases cannot beFigure 1-24. A Transabdominal image through the uterus usingthe bladder (BL) as an acoustic window. The endometrial stripe cannot be well-defined. B Transvaginal image showing improved resolution of the endometrium (arrow). Following page: C Transabdominalimage of the right ovary (calipers) revealing little detail of the ovarianarchitecture (BL bladder). D Transvaginal technique allows for visualization of the ovarian parenchyma and individual follicles (arrows).
Introduction to Diagnostic Ultrasound imaged 1–2 weeks earlier, and there is no need for bladderfilling prior to the examination. The vaginal transducercan also be used to locate areas of tenderness and to helprule out adhesions by checking for organ mobility. SeeBox 1-6.Box 1-6.CHAPTER 1Advantages of transvaginal sonography.Provides information that cannot be obtainedtransabdominally.Tissue resolution is improved because of thehigh-frequency transvaginal transducers.DisadvantagesLarge obese patients and those with surgicalscarring are more easily imaged.Although transvaginal sonography can provide valuable,additional information, it is not the recommendation ofthis author to use the technique solely. Due to the lackof penetration provided by higher frequencies, the depthof penetration is only about 6 cm; therefore, anatomypositioned higher in the pelvis will not be imaged. Anenlarged uterus filled with fibroids cannot be adequatelyevaluated, nor can vaginal masses such as Gartner’s ductEndometrium and fundus of a retroflexed uterusare better imaged.Products of conception can be imaged 1–2 weeksearlier.Bladder filling is not required.Areas of tenderness can be localized andevaluated.Adhesions can be ruled out by confirming organmobility.Ccysts. As the bladder begins to fill, pelvic anatomy isdisplaced out of the field of view, and artifactual refractive shadows from the bladder
Chapter 6 Ultrasound of the Cervix during Pregnancy 215 Pamela M. Foy, MS, RDMS, FSDMS Objectives 215 Anatomy 216 Cervical Length Measurements 216 Cervical Incompetence 218 Cerclage 218 Preterm Labor and Premature Birth 219 Cervical Pregnancy 222 Technique 222 Scanning Tips, Guidel