Transcription
Using Qualitative Methods in yourImplementation Science Study
Acknowledgements Barbara G. Bokhour, PhD; Mari-Lynn Drainoni, PhD; RendelleE. Bolton, MSW, MA; Timothy P. Hogan, PhD This work was supported by a Career Development AwardCDA 14-156 from the U.S. Department of Veterans Affairs, This material is based upon work in part by the Department ofVeterans Affairs, Veterans Health Administration, Office ofResearch and Development and Health Services Research andDevelopment. The contents do not represent the views of the U.S.Department of Veterans Affairs or the United StatesGovernment No conflicts of interest2
Goals Provide an overview of qualitative methods in ImplementationScience Familiarize audience with strengths of different qualitativeapproaches Use real-world examples to demonstrate how to incorporatequalitative methods in an IS study Provide practical strategies to incorporate qualitativemethods into an IS study3
OverviewI.II.III.IV.Implementation ScienceWhy Qualitative MethodsQualitative MethodsExampleV. Using Qualitative Methods in your ImplementationScience Study4
I. IMPLEMENTATION SCIENCE5
What is Implementation Science Uses a systematic approach to understand & address barriersto effective implementation of EBPs Study of methods to promote the integration of researchfindings and evidence into healthcare policy and practice Seeks to understand the behavior of healthcare professionalsand other stakeholders as a key variable in the sustainableuptake, adoption, and implementation of EBPs Investigates & addresses major bottlenecks (e.g. social,behavioral, economic, management) that impede effectiveimplementation, Tests approaches to improve health programs Determines a causal relationship between the interventionand its impactDrainoni; NIH6
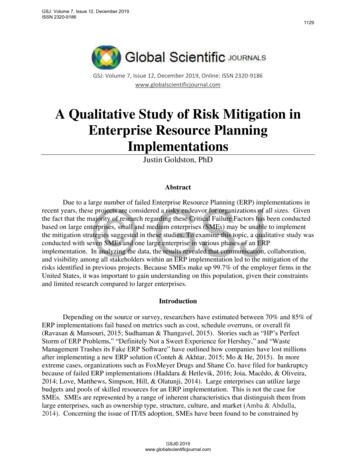
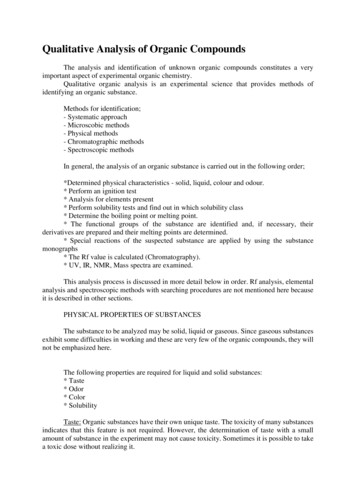
Why Implementation Science?CA orBust!Easy RouteBut 68% stayedin FloridaMade it:32%Satisfied:75%NorthernLong WinterBut met otherswho helpedMade it:60%Satisfied:55%MiddleHard Route,Famine, poorlypreparedMade it:15%Satisfied:5%SouthernBolton, RB7
Why Implementation Science? Implementation can help us learn: Program e ResultsProvide future guidance“De-implementation” A conceptual framework can: Help us understand what happens when a program isimplemented Identify key people or features to examine8Bolton, RB
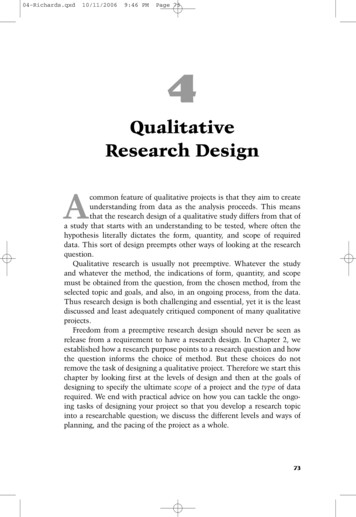
Consolidated Framework forImplementation Research (CFIR)9Damschroder 2009
Implementation Science Characteristics Real-world More complicated & “messy” than traditional studies – realworld, adaptation is part of it Contextual Incorporates context Attentive to local cultural & community influences Complex Dynamic, adaptive, occurs at multiple levels, non-linear, analysesare multi-component (process outcomes & clinical outcomes)10Drainoni
Data Collection and Analysis - What isUnique with Implementation Science? Diverse array of data collection & analysis techniques Multiple forms of non-traditional data are common Notes from meetings, conference calls, e-mails, documents andother artifacts Multiple types of participants are included Patients, providers, team members, other stakeholders Data analysis is often on-going with quick turn-around as thedata are needed to guide study decisions throughout theprojectZickmond, Hamilton & Bokhour11
II. QUALITATIVE METHODS12
Why Qualitative Methods? Rich descriptions of phenomenaDescribe complex settings/interactionsEnhance understanding of contextTheory developmentIdentify patternsProvides meaningful explanations Traditionally used in social sciences (sociology, anthropology) Increasingly used in Health Services & Implementation Science13(Sofaer1999)
When to Use Qualitative Methods Good for “Why?” or “How?” questions Need detailed descriptions or explanations of experiences,behaviors or beliefs Identifying and exploring Want to identify a range of behaviors Describing Capture dimensions or describe complex processes Explaining How or why individuals do/don’t do certain things Evaluation/Assessment14 Tell the program’s storyGuest, Namey, Mitchell 2013
When Not to Use Qualitative Methods Test theories with hypothesis Make generalizations to the whole population Reliably comparing groups (i.e., pre-test/post-test) Measure the outcomes of a program15Guest, Namey, Mitchell 2013
Qualitative Methods in Implementation Science Qualitative methods are an essential aspect ofImplementation Science Particularly well-suited to: Discern how effectively an intervention is adopted at a site(fidelity) Reveal the organizational or interpersonal dynamics that canaffect an intervention Participants’ (e.g., staff, patients) insider knowledge & perspectivesabout the evidence & context in which implementation is to occur Uncover the barriers & facilitators that impact the uptake of theintervention16Zickmond, Hamilton & Bokhour
III. THE METHODS17
Qualitative Methods InterviewFocus GroupArchival DocumentsObservation Data is often used in conjunction with each other and withquantitative data (i.e., mixed methods)18
Qualitative Interview Conversation designed to elicit depth on a topic of interestUsually 1-on-1Open-ended questionsInductive probingLook/feel like a conversation Strength: Good for understanding perspectives or experiences Limitation: Labor intensive; may miss perspectives; don’tknow what people actually do19Guest, Namey, Mitchell 2013
Focus Group Carefully planned discussion with a small group of peopleFocused topicExperiences, opinions, perceptions, reactionsGroup setting and group dynamics are integralSimilarity in group (characteristics, experiences, situation)Discussion moderated by experienced researcher Strength: Good for generating ideas; can be fast way to collectdata Limitation: Not good for personal experiences; quieter peoplemay not speak; not good for all populations (i.e., difficult toreach)Guest, Namey, Mitchell 201320
Archival Documents Textual & visual; Selected (not generated) Example documents: Meeting minutesMemosMission statementsPresentation materialsPolicy documentsProcedural documents (steps taken to achieve something)Clinical practice guidelinesPatient recordsEducational materials, pamphlets, brochures Strength: Easy to collect Limitation: actually happening; hard to follow-upGuest, Namey, Mitchell 2013; Bokhour21
Observation Systematic recording of events, actions & interactions Participant Observation Unstructured/qualitative Traditionally used in anthropology Direct Observation More structured/quantitative, systematic How many, how often Strengths: capture behaviors participants may be unaware of Limitation: labor intensiveGuest, Namey, Mitchell 2013; Rossman & Rallis 201722
Observation Data Collection Tools Fieldnotes Templates Recording sheets and check lists23
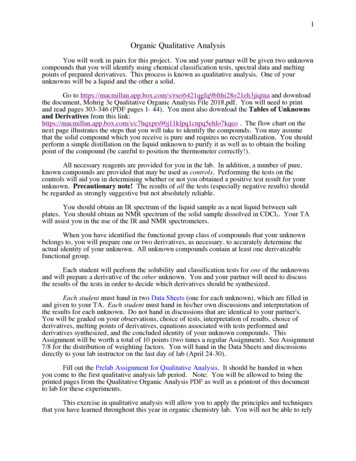
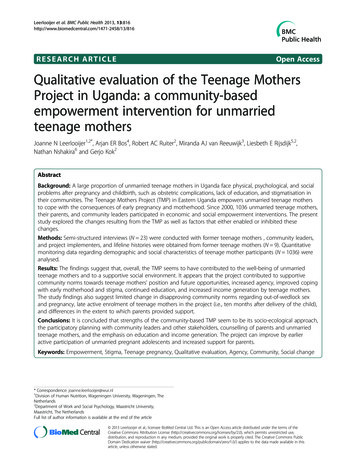
Fieldnotes Least standardized Open-ended,narrative Does not includepreset questions orresponses Example: Fieldnote, written by GMFixSpring 201424
Templates List the interactions,processes orbehaviors Space to jot downnarrative data Allows for emergentdata to be recorded Example: Observation template. From VAPEC 13-001 (Developed by GM Fix & REBolton; BG Bokhour, PI)25
26
Recording Sheets and Check Lists Standardized A priori questions &responses Allows for countingphenomena Keen, M. et al. (2015). "Using the patientcentered observation form: Evaluation ofan online training program." PatientEducation and Counseling.27
IV. AN EXAMPLE28
ImplementingPersonal Health Planning in VA:Results of a Multisite Evaluation
TeamGemmae M. Fix, PhDBarbara G. Bokhour, PhD Principal Investigator, EPCCErrol Baker, PhDAnna Barker, MSRendelle E. Bolton, MSW, MAKimberly L. HarveyTimothy P. Hogan, PhDTana M. Luger, PhD, MPHMark MeterkoDonald R. Miller, ScDTherasia Roland, MSWMollie Ruben, PhD This work was supported by a Partnered Evaluation Center Award #13-001 fromthe U.S. Department of Veterans Affairs, Office of Patient-Centered Care andCultural Transformation and the Quality Enhancement Research InitiativePrograms.30
What is Patient-Centered Care? Patient-Centered Care (PCC) Institute of Medicine Care that is respectful of and responsive to individual patientpreferences, needs, and values Ensures that patient values guide all clinical decisions Small, but growing evidence base Healthcare systems implementing PCC programs Requires cultural shift in care practices VA’s Office of Patient-Centered Care & Cultural Transformation Focused on transforming VA to a system that providespersonalized, proactive, patient-driven care Implementing several PCC initiatives31
Personal Health Planning VA Patient-Centered Care initiative Collaborative development of a health plan Patient identifies health goal, based on patient life context,values, preferences Series of questions designed to identify what really matters Growing evidence base32
MyStory: Personal HealthInventory1.What REALLY matters to you in your life?2.What brings you a sense of joy andhappiness?3.What is your vision of your best possiblehealth?CURRENT AND DESIRED STATES:33
PHP Implementation Goal of OPCC&CT was to know what the impact of PHP was onVeterans Natural experiment; Not a prescriptive rollout of evidenced-based program Sites given latitude on what and how they implemented PHP EPCC research team wanted to learn: How PHP was implemented at a range of sites,How PHP was done, in depthWhat were patients experiences with PHPWhat were the patient reported and clinical outcomes of PHP.34
Study Objectives Understand what PHP looked like in practice How PHP was implemented at a range of sites How PHP was done, in depth Examine patient experiences of PHP Describe clinical outcomes associated with exposure to PHP35
Study DesignI. Qualitative Evaluation of Implementation Phase 1, broad overview Phase 2, in-depth case studiesII. Quantitative Evaluation Patient surveys Intermediate clinical outcomes36
Mixed-Methods Design More than just qualitative & quantitative data Multiple data sources : Qualitative (interviews, observations, case study approach), Quantitative (survey, database) Inter-related, complementary data Iterative, integration between qualitative & quantitativemethods.37
Collaboration Administrative level OPCC&CT and EPCC OPCC&CT field team and EPCC research team Site level EPCC research team and study sites Team level EPCC qualitative research team and quantitative research team38
I. Qualitative39
Collaboration Administrative level OPCC&CT and EPCC OPCC&CT field team and EPCC research team Site level EPCC research team and study sites Team level EPCC qualitative research team and quantitative research team40
Study Design1.1 How PHP was implemented at a range of sites, 10 diverse sites Selection criteria: OPCC&CT input; size, location & program history Qualitative phone interviews with PHP leads1.2 How PHP was done, in depth 2 sites Selection criteria: extent of PHP program, use of innovative practices& potential to be spread Ethnographic (site visits; interviews, observation, document review) Analysis Qualitative, grounded thematic approach A priori coding, based on PHP program & theories of PCC41
SiteSite CharacteristicsWhere PHP isImplementedWhich VeteransResponsible staff1Rural South Atlantic,High complexity (1c)Wellness Clinic groups;Individual health coachingPre-transplant;Health coachesHistory of substance abuse2Rural Southwest Central,High complexity (1a)Shared MedicalAppointmentsHypertension;Less complexShared MedicalAppointment Providers &Ancillary Staff3Urban New England,High complexity (1a)1 PACT teamNo acute concernsPACT MD & RN4Rural Pacific West,Low complexity (3)All PACT teamsAll PACT patientsPACT clerk, LPN, RN, &provider5Urban Southwest Central,High complexity (1b)Pain clinicChronic painPain clinic providers &ancillary staff6Urban Southwest Central,High complexity (1c)PACT;Mental HealthSerious mental illnessPeer Support Specialists inShared MedicalAppointments & IndividualAppointments7Urban New England,High complexity (1a)1 PACT team;1 Women’s Health Clinic;1 CBOCNo acute concerns1 MD in each location & RN8Rural New England,Low complexity (3)Pain clinicChronic painAll clinic team members9Urban Southeast Central,Medium complexity (2)Health coachingChronic conditionsHealth coaches10Urban Midwest,High complexity (1a)PACT teams at main facilityCBOCsAll patients interested inhealth planningPeer health coach;RN Care Manager42
All patients Non-acuteappointments Diagnosis(hypertension,seriousmental illness,chronic pain)Responsible Staff Primary Care Mental Health Pain Clinic SharedMedicalAppointmentsPatient PopulationLocationPhase 1.1 Findings 1-2 people Whole team Health coach MD & RN43
Phase 1.2 SitesFacilitySITE 4.Communitybased outpatientclinicPacific NWSITE 10.Large, urbanmedical centerMidwestSetting*Strong supportfrom MedicalDirector*2 leads from mainfacility*Regional support*Aligned withalready ongoinginitiativesPHPProgram*“Life Goals”*Distributed by clerks*clinicians & ancillarystaff discussthroughout appt.*Clinicians or ancillarystaff refer patient*Health Coach workswith patients*HC develop PHP &provide ongoingsupport44
Phase 1.2 Data CollectionRoleSite 4Administrative Staff5 interviews;1 observationHealth Coach ProgramSite 103 interviews;1 observation;1 focus group3 interviewsPrimary Care TeamAncillary Staff8 interviews3 interviews4 interviews3 interviewsPatients9 observations2 interviews4 observations4 interviews45TOTAL: 35 interviews; 15 observations; 1 focus group
Phase 1.2 FindingsPatient-ProviderInteractionDevelop a Clinic CultureSupportive of PHPFacility-level FoundationSupportive of PHP46
Build a Facility-level FoundationSupportive of PHP Leadership support at all levels Quality over quantity PHP information documented and communicatedSite 10 PHP in the electronic medical record (EMR) Clinical Application Coordinator (CAC) enlisted to develop an electronictemplate in EMR Entire facility had access to a patient’s PHP47
Develop a Supportive Clinic Culture Involve providers in the implementation processEngage all primary care providers in PHPTrain team members responsible for PHPRaise awareness across ancillary staffSite 10 Ancillary staff (dietitian, social work, pharmacy, behavioral health) Largely unaware of PHP Developed their own care plans, in accordance with their scope of practice Care plans were not informed by or even congruent with PHPs A dietician characterized his role by saying: “[My] plan has more to dowith the goals that we [the providers] actually set for the patients. [We]make sure that they’re onboard with. I mean I’m never going to tell apatient, you know, ‘You need to do this,’ without them, you know,acquiescing to actually do it.”48
Patient-Provider Interactions Orient the patientEngage patients in conversations about their prioritiesCollaboration between primary care and ancillary staffIdentify meaningful goals with actionable plansSite 4Beginning of appointment.Clerk introduces PHP & explains it is a different way of providing healthcare“[PHP] really helps put you in the driver’s seat of your health care. For a longtime, the VA has been the driver of that bus, and that’s really not where weshould be"End of the appointment.Clerk checks the patient out.Asks if the patient has questions or issues the patient had not had theopportunity to ask.49
Putting PHP into Practice (cont.) Orient the patientEngage patients in conversations about their prioritiesCollaboration between primary care and ancillary staffIdentify meaningful goals with actionable plansSite 10PatientMade PHP appointment focused on smoking cessationPrevious day, had emergency appointment for high blood glucoseAppointmentNurse framed the appointmentHealth coach & nurse ask patient about his daily life (not smoking)Daily life discussed ; marked by when and where the patient smokedPlanCollaboratively decided to reduce smoking during work breaksHealth coach & nurse suggested strategies– which the patient connected todiabetes management50
Recommendations for Implementing PHP Develop a local vision, including facility-level strategicplanning and self-reflection Define roles and communication practices across the team Create infrastructure to support the PHP process, built onexisting processes and attentive to patient flow Conduct iterative rounds of piloting to incorporate staff,provider and patient needs Foster an organizational climate that supports PHP, such asidentifying and supporting PCC champions51
Collaboration Administrative level OPCC&CT and EPCC OPCC&CT field team and EPCC research team Site level EPCC research team and study sites Team level EPCC qualitative research team and quantitative research team52
II. Quantitative53
Aims and Approaches Assess veteran perceptions of the Personal Health Planning(PHP) Process and its impact on patient-level outcomesVeteran Experience Survey Evaluate effects of PHP on clinical outcomes over timeTime-series analysis of selected clinical measures54
Veteran Experience SurveySurvey Measures of the PHP Process Derived from Qualitative WorkPersonal Health GoalsActions by VA primary care team and health coach to help reach personal health goalsHelpfulness of specific programs and services at site in reaching personal health goalsExperiences in personal health planningSatisfaction with personal health planningAdditional Measures – Previously Developed, Validated, and UsedPatient Experience CategoryMeasures UsedProcess of CareCommunication Assessment Tool (CAT), CollaboRATESelf-Reported Health and Functional StatusPROMIS (Patient Reported Outcomes MeasurementInformation System)Self-EfficacyChronic Disease Self-Efficacy ScalePatient’s Confidence in Managing HealthPatient Activation Measure (PAM)VA ServicesServices offered at outpatient sitesSociodemographicsGeneral health, sex, age, social conditions, etc.55
Survey Methods Sites 2 PHP qualitative evaluation sites 2 comparison sites similar in region, size, and complexity. As example, presenting results from one PHP site and its comparisonsite (urban Midwest) Survey mailed to patients along with a 5 CVS gift card as incentive;reminder card sent to non-respondents Survey samples Identified by healthcare teams PHP site- 304 outpatients - 168 completed surveys (55%) Comparison - 304 outpatients - 149 completed surveys (49%)56
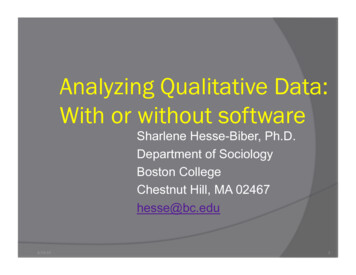
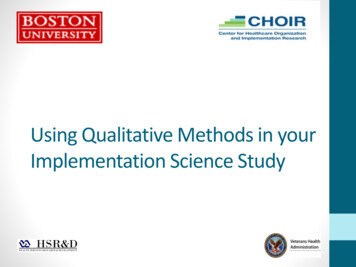
Veteran Experience Survey at PHP SiteHow VA primary care team or health coach helpedveterans reach their personal health goalsReferred me to another VA professionalRecommended a VA class/activityProvided me with encouragement and supportHelped motivate meGave me educational materialsHelped connect me with a specialist or serviceHelped me set realistic/concrete goalsHelped me identify and overcome obstaclesGave me the confidence to build additional skillsHelped me stay accountable to action plan0%10%20%30%40%50%60%70%Veterans received broad and varied support in reaching health goals
Veteran Experience Survey at PHP SiteExperiences of Veterans in Personal Health Planning88% Personal health goal is important to health and well-being75% Would recommend setting a personal health goal74% Had enough say in selecting a personal health goal73% Made progress toward reaching personal health goal72% Someone followed up to discuss progress on personal health goal70% Often discuss personal health goal at visits with VA primary careteam or coach69% Relationship with VA health care team or health coach was helpfulin making progress towards personal health goal68% Choosing a personal health goal improved my health and well-beingVeterans’ experiences were genera
1 PACT team No acute concerns PACT MD & RN 4 Rural Pacific West, Low complexity (3) All PACT teams All PACT patients PACT clerk, LPN, RN, & provider 5 Urban Southwest Central, High complexity (1b) Pain clinic Chronic pain Pain clinic providers & ancillary staff 6 Urban Southwest Central, Hi