Transcription
MATERNAL,NEWBORN ANDCHILD HEALTH IN THEAMERICASA report on the commitmentsto women’s and children’s health
This work was co-authored by The Canadian Red Cross Society with theInternational Federation of Red Cross and Red Crescent Societies. TheCanadian Red Cross reserves its right, title and interest in and to this workand any rights not expressly granted are reserved by the Canadian Red Cross.Without limiting the rights under copyright reserved above, any part of thispublication may be cited, copied, translated into other languages or adaptedto meet local needs without prior permission from the Canadian Red Crossprovided that the source is clearly stated. In consideration of this, such useshall be at the sole discretion and liability of the user and the said user shallbe solely responsible, and shall indemnify the Canadian Red Cross, for anydamage or loss resulting from such use.ISBN 978-1-55104-595-5(c) International Federation of Red Cross and Red Crescent Societies &Canadian Red Cross Society, Geneva, 2013Requests for commercial reproduction should be directed to the IFRCat secretariat@ifrc.org and the Canadian Red Cross Society located at170 Metcalfe St., Ottawa, ON, K2P 2P2, Canada, Tel: (613) 740-1900 orby email at feedback@redcross.ca.Cover photo: Sonia Komenda/CRCAcknowledgementsThe IFRC Americas Zone Health Team would like to thank the Canadian RedCross for funding the MNCH Research Delegate position in the Americas ZoneOffice to conduct this project and for the extensive efforts of the AmericasTeam in the overall production of the report.We would also like to recognize Dr. Salim Sohani, Senior Health Advisor at theCanadian Red Cross for the technical expertise he contributed to this report.His insights and knowledge enabled the exploration of different angles on theissues of MNCH and health equity.We would also like to thank Christopher Drasbek, Regional Advisor, IntegratedChild Health, Pan American Health Organization/World Health Organization(PAHO/WHO), Washington, DC, for his technical review of the report. Hissuggestions and input were valuable.ContributorsSonia Komenda – Main Researcher, CRCJulie Hoare – Americas Zone Health Coordinator/Project Manager, IFRCDr. Salim Sohani – MNCH and Technical Advisor, CRC
This report is made possible through the support ofthe International Federation of Red Cross and RedCrescent Societies (IFRC), in co-operation with theCanadian Red Cross and the Pan American HealthOrganization (PAHO).International Federation of Red Cross and Red CrescentSocietiesStrategy 2020 voices the collective determination of the International Federationof Red Cross and Red Crescent Societies (IFRC) to move forward in tackling themajor challenges that confront humanity in the next decade. Informed by the needsand vulnerabilities of the diverse communities with whom we work, as well as thebasic rights and freedoms to which all are entitled, this strategy seeks to benefit allwho look to Red Cross Red Crescent to help to build a more humane, dignified, andpeaceful world.www.ifrc.orgSaving lives, changing minds.Over the next ten years, the collective focus of the IFRC will be on achieving thefollowing strategic aims:1.2.3.Save lives, protect livelihoods, and strengthen recovery from disasters andcrisesEnable healthy and safe livingPromote social inclusion and a culture of non-violence and peaceCanadian Red CrossThe Canadian Red Cross works with partner Red Cross and Red Crescent Societiesaround the world to meet the Millennium Development Goals of reducingpreventable deaths of children under the age of five, and to improve maternalhealth. The Canadian Red Cross has been active in maternal, newborn and childhealth (MNCH) since 1997, and supports programs in some 20 countries. Since 2005,Canadian Red Cross supported MNCH programs have reached more than 12 millionpeople directly, and have indirectly benefited another 40 million. Forty thousandtrained Red Cross volunteers have contributed to the achievement of health programobjectives. www.redcross.caPan American Health Organization/World HealthOrganization (PAHO/WHO)The Pan American Health Organization (PAHO), founded in 1902, is the world’s oldestinternational public health agency. It provides technical cooperation and mobilizespartnerships to improve health and quality of life in the countries of the Americas.PAHO is the specialized health agency of the Inter-American System and servesas the Regional Office for the Americas of the World Health Organization (WHO).Together with WHO, PAHO is a member of the United Nations system. www.paho.org
4MNCH in the Americas A report on the commitments to women’s and children’s healthContentsExecutive Summary. 6Key Findings and Recommendations. 8Methods. 10RESULTS. 11The Current MNCH Situation. 11Survey to National Societies. 16Questions 1, 2 and 3. 16Questions 4, 5 and 6. 17Questions 7 and 11. 20Question 8. 23Questions 9, 10 and 12. 24Partner National Societies Priorities and Commitments. 25External Partners: Priorities and MNCH Activities. 27DISCUSSION. 29Gaps Based on Current Need. 29Gaps Within the Movement. 31Gap Analysis of Top Five Countries in Need of MNCH Programming. 33Case Study: Haiti. 35Gaps Outside the Movement. 36Coordination Within the Top Five Countriesin which External Partners Implement MNCH. 38Case Study: Bolivia. 40Case Study: Honduras. 42Disparities in MNCH. 44Case Study: Guatemala. 46Case Study: Colombia . 52Case Study: Health Disparities in Panama. 54Next Steps. 55Annexes.ANNEX A – Scale and Results of Statistical Analysis of MNCH Indicators. 56ANNEX B – HDI Value. 58Annex C – MNCH Survey to National Societies. 59Annex D – List of National Societies that Answered the Survey. 64Annex E – Partner National Societies: MNCH-related Projects. 65Annex F – List of Current Government Strategies or Projects. 66Annex G - External Partners List per Country. 67Annex H - Government Priorities and Commitments. 68Annex I - Acronyms and Definitions. 73References. 74
MNCH in the Americas A report on the commitments to women’s and children’s healthTable of Figures and TablesTable 1. Top five countries in the Americas in needbased on under-five, neonatal and maternal mortality. 12Table 2. National Society responses per region in the Americas. 16Table 3. Highest implementation rates for MNCH activities in the Americas. . 17Table 4. Highest implementation rates for MNCH-related activities in the Americas. 20Table 5. Partner National Society MNCH projects in the Americas. 26Table 6. MNCH projects of external partners. 28Table 7. Comparison of all actors for top five countries in need. 39Table 8. Percentage of birth attended by skilled personnel in Haiti. 45Table 9. Government Health Strategies/Plans. 68Table 10. Current government national health strategies by region. 69Table 11. Countries with Maternal and Child health in their National Health Strategies. . 70Table 12. Governments with MNCH Strategy. 70Figure 1. Global Maternal Mortality Ratio Trends. 11Figure 2. Causes of child deaths (under 5). 12Figure 3. Maternal Mortality Ratio and Child Mortality Rate Maps in the Americas. 13Figure 4. Gap Analysis of Top Five Countries in Need of MNCH Programming . 14Figure 5. HDI Value Ranking in the Americas. 15Figure 6.National Societies Implementing MNCH. 17Figure 7. MNCH activities by scope in the Americas (question 4.a). 19Figure 8. MNCH-related activities by scope in the Americas (question 5.a). 19Figure 9. Work of National Societies in Health in Emergencies in the Americas. 21Figure 10. National Societies Capacity to Implement MNCH in the Americas. 21Figure 11. Support required to implement MNCH programming in the Americas. 22Figure 12. Likelihood of implementing MNCH in future years in the Americas. 23Figure 13. National government commitment to MNCH in the Americas. 24Figure 14. Partner National Societies - MNCH activities and projects in the Americas. 25Figure 15. External Partner Priority Countries. 27Figure 16. The Continuum of Care through time. 30Figure 17. Partner National Societies compared to National Societies - MNCH projects. 31Figure 18. Red Cross Red Crescent and External Partner MNCH Projects. 37Figure 19. “Guatemala: Inequalities in Health, Nutrition and Population”. 45Figure 20. “Guatemala: Inequalities in Health, Nutrition and Population”. 45Figure 21. Mortality rate by Departments in Bolivia 1994-2008. 48Figure 22. Guyana and Suriname, Country Programme Document 2012-2016. 49Figure 23. Under- Five Moartility rate in Honduras. 50Figure 24. Percentage of births attended by skilled personnel. 50Figure 25. Honduras Demographic and Health Survey. 51Figure 26. Maternal mortality per province in Panama. Source. 54Figure 27. MNCH components in National Health Strategies. 71Figure 28. Key Areas within MNCH. 725
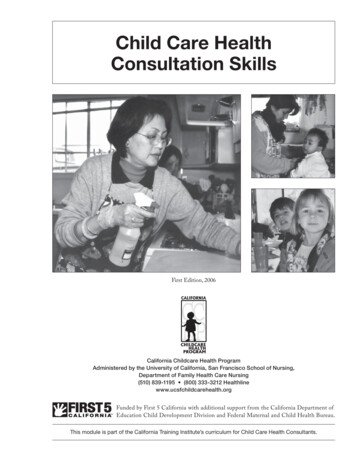
6MNCH in the Americas A report on the commitments to women’s and children’s healthExecutive SummaryThrough its network of National RedCross Red and Crescent Societies, theInternational Federation of Red Crossand Red Crescent Societies (IFRC) hasbeen supporting and implementinghealth initiatives related to reproductive,maternal, newborn and child health(MNCH) for over 20 years. TheseMNCH initiatives include communityprogrammes that promote healthybehaviours, increase vaccinations,monitor the growth of children andprevent malnutrition, diarrhea andrespiratory diseases. Also, the IFRCworks with partners to increaseuniversal access to care for mothers,children and other vulnerable people.The reasoning behind investing in MNCH stems fromthe IFRC’s Strategy 2020, which sets ambitious goals forhealth. These goals are to build national society capacityto enable safe and healthy living, respond appropriatelyto health emergencies and crises, reduce vulnerabilities,build resilient communities and position the Red Cross RedCrescent as a leading strategic partner in global health. Akey strategic aim focuses on building resilience. In terms ofhealth, this can be addressed on an individual, community,national or global level; however, it is important to look atsome of the most vulnerable populations such as womenand children. The importance of MNCH is addressed in theIFRC’s global Strategic Operational Framework for health(2011–2015).In the next five years, the IFRC will focus on developing amore coherent approach to MNCH as part of integratedcommunity health programming and to contribute to theachievement of Millennium Development Goals (MDGs) 4and 5. So far, there has been some success in child healthand achieving the MDGs in the Americas region; however,many countries still have a long way to go because progresshas not been equitable. This lack of progress in the region,especially in maternal health, needs to be addressed bylooking at these immense disparities to ensure lowermortality rates of mothers and of children under five yearsof age. A strong connection needs to be made with NationalSocieties to ensure they have the support they need to helpthem achieve these goals.
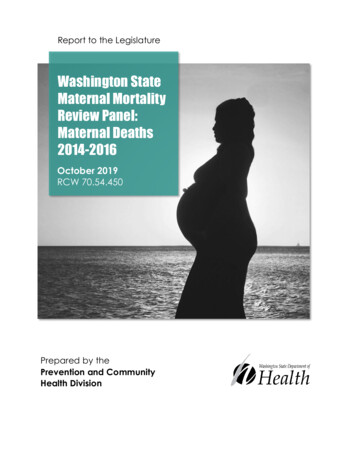
MNCH in the AmericasThis project, an IFRC initiative from the Americas Zonehealth programme, sought to map current Red CrossRed Crescent MNCH programming and MNCH-relatedactivities conducted by National Societies, Partner NationalSocieties, governments and external organizations, aswell as document models, review gaps, identify policyand funding trends in MNCH in the region, and identifyMNCH needs in the Americas. A research delegate inAmericas Zone office in Panama conducted this research.The methodology included the use of surveys (onlineand electronic document format), formal interviewsand meetings to gather the necessary information fromrelevant stakeholders. Additional background research wasconducted to examine strategies and statistics regardingthe subject matter and to identify the individual needs ofpriority countries in terms of MNCH and other potentialrelated areas in health. This research was conducted fromJanuary to April 2012 and has been compiled in this reportalong with recommendations and analysis on the currentsituation and future possibilities for the region. This reportwill serve as a base for a feasible three-year plan of actionto promote and scale-up Red Cross Red Crescent MNCHprogramming in the Americas, which will respond to theIFRC’s Long Term Planning Framework - the Americas Zone2012-2015 and America’s Framework for Action (2012-2016).In order to contribute to the development of a regionalframework for Red Cross Red Crescent MNCH programmingin the Americas and a three-year action plan, informationhas been compiled in this report on MNCH projects oractivities being implemented by National Societies inthe Americas, including those supported by PartnerNational Societies. Existing regional Red Cross healthnetworks in the Caribbean, Central and South Americaserve as a mechanism for coordination, collaboration andcommunication between National Societies, in liaisonwith IFRC zone and regional health staff. The reportalso provides information on the level of coordinationbetween Red Cross Red Crescent partners at the nationallevel and the extent of National Societies’ collaborationand coordination with their ministries of health andkey international or non-governmental organizations todetermine where partnerships can be improved, and tostrengthen the auxiliary role of National Societies. A report on the commitments to women’s and children’s healthThe mapping initiative identified the top five countriesmost in need of MNCH programming: Haiti, Guatemala,Bolivia, Guyana and Honduras. Additionally, Guyana isthe only country out of the top five not prioritized byexternal partners and Partner National Societies for MNCHprogramming.The initiative also identified a lack of MNCH specificfunding in the coming years. Currently, no MNCH PartnerNational Society programming has guaranteed fundingbeyond 2013, other than Haiti. More efforts need to bededicated to seek funding specific to MNCH in future years,especially for the top five countries identified as being inneed of MNCH programming.Even though National Societies are highly committed toMNCH, less than 40 per cent of National Societies areimplementing activities in the post-natal period. Healthrelated programming instead tends to focus more onhygiene promotion, sexual and reproductive health, andnutrition. This may be due to such topics being moremainstream or common health topics or related to fundingpriorities. Greater focus on post-natal and neonatal healthcould help prevent neonatal deaths.Supporting National Societies in developing or updating theirMNCH strategies or objectives is key since only nine NationalSocieties have active MNCH staff and only two NationalSocieties have made pledges to support MNCH work.When looking at inequalities in health, most of thedisparities in MNCH in the top five countries in needare found within ethnic groups, especially indigenouspopulations. In Bolivia, Guatemala, Guyana, Hondurasand Panama, the worst statistics for maternal and childindicators are found in indigenous districts or zones withhigh indigenous populations.This study provides a picture of the current situationof Red Cross Red Crescent women’s and children’shealth and MNCH programming in the Americas region.The study has been conducted in the hopes of helpingNational Societies and the IFRC identify the importanceof MNCH and prioritize key areas of work to improve thehealth of mother and children and, therefore, help achieveMDGs 4 and 5 by 2015.7
8MNCH in the Americas A report on the commitments to women’s and children’s healthKey Findings and RecommendationsThis report evaluated the current situation of MNCH in the Americas. Aftertaking into account the work of National Societies, Partner National Societies,governments and external partners, key findings and recommendations weredetermined.1The countries that are most in need of MNCH programmingare, in order, Haiti, Guatemala, Bolivia, Guyana andHonduras.2Guyana is the only country out of the top five countriesin need that is not prioritized by external partners andPartner National Societies for MNCH programming. It isexperiencing a severe lack of maternal healthcare activitiesto address the high maternal mortality ratio. It is also facingmajor MNCH disparities in a specific region - the interior.Recommendation: More programming priority andsupport should be given for Guyana - especially formaternal health and in the hinterland region.3Most of the activities implemented by Red Cross RedCrescent are preventative — focusing on dissemination ofknowledge and health promotion. Red Cross Red Crescentis supporting the government’s implementation of curativeMNCH activities.Recommendation: Continue communication andcoordination with governments to ensure that bothcommunity and institutional MNCH are covered. Developcooperation strategies with governments to ensurecomplementary work between preventative care andcurative care.4The region in which most National Societies areimplementing MNCH is South America.Recommendation: Use South America’s MNCHexperience for lessons learned that can be applied toother regions. Facilitate communication between NationalSocieties on MNCH programming and support crossregional health networking.5National Societies are committed to working with theirgovernments and implementing MNCH activities; however,their needs are not being fulfilled by Partner NationalSocieties due to a lack of MNCH-specific funding in thecoming years. Partner National Societies cannot helpNational Societies with project funding and resourcemobilization because they themselves do not haveguaranteed funding from donors to extend their currentMNCH projects.6Currently, no Partner National Society MNCH programminghas guaranteed funding beyond 2013, other than Haiti.Recommendation: Dedicate more efforts to seek MNCHspecific funding in future years, especially for the top fivecountries in need.7The only two countries in which Partner National Societiesare not supporting the implementation of MNCH programsare Brazil and Suriname. Suriname ranks eighth in need ofMNCH, third in the Americas for infant death ratio and is inhigh need of education on health practices such as breastfeeding. The Suriname national society does not havehealth staff specifically dedicated to MNCH.Recommendation: MNCH, especially health promotionactivities and infant health, should be prioritized inSuriname by Partner National Societies and externalpartners. Also, provide training on MNCH to the SurinameRed Cross to increase its capacity to implement activitiesand projects.
MNCH in the Americas8Red Cross Red Crescent is a community-based healthimplementing agent for MNCH. Through its wide networkof volunteers and experience in CBHFA, it has the toolsto support the government in implementing MNCHprogrammes at a community level.Recommendation: Continue to support building thecapacity of Red Cross Red Crescent volunteers on MNCHto ensure access to MNCH resources and knowledge toeveryone, especially at a community level. A report on the commitments to women’s and children’s health13Ten organizations have MNCH projects in Bolivia, nine inHaiti, and eight in Honduras. Bolivia and Haiti are a priorityfor 16 agencies and organizations, and Honduras for 14.Recommendation: National Societies should coordinatewith external partners in the seven countries in whichMNCH work is present and collaborate on MNCH projectsor support external partners with MNCH-related activities,especially if the National Societies does not have on-goingMNCH projects.914The gap in newborn health programming is present in theAmericas, and more pronounced in the Caribbean. Lessthan 40 per cent of National Societies are implementingactivities in the post-natal period, which could help preventneonatal deaths.In the disparity analysis, the data on equity, whether takinginto account wealth or residence, indicated that the mainissue is lack of access to health services. This lack ofaccess is due to several reasons including social exclusionof the ethnic population, lack of funding for services, orgeographical isolation.Recommendation: Increase basic post-natal care and/orvisits conducted by National Societies to ensure that hardThe disparities in MNCH are greater between differences into access and vulnerable communities have access to these wealth than place of residence.services.Recommendation: Use the Red Cross Red Crescentvolunteer network to increase communication withmunicipal/regional health delivery points about MNCHProgramming trends are more focused towards HIVneeds in poor, ethnic and remote communities. Also, useprevention and care and sexual and reproductive health;Red Cross Red Crescent volunteers that are part of hard tohowever, this type of programming does not reach all partsaccess communities to provide MNCH care in places whereof the continuum of care.governments and external partners may not have access.Recommendation: More needs to be done from all actors Perform a needs assessment to identify the communitieswith the hardest access to health services and provideon the curative side of MNCH to address the gaps that arecapacity building on MNCH.present.1011Many National Societies are interested in implementingor continuing their implementation of MNCH. Howeveronly nine National Societies have active MNCH staff andonly two National Societies have made pledges to supportMNCH work.Recommendation: Support National Societies indeveloping or updating their MNCH strategies or objectives.Provide technical support to National Societies that areimplementing or are interested in implementing MNCH butdo not have MNCH staff.12External partners support the implementation of MNCHprograms in seven more countries than Partner NationalSocieties and National Societies, in addition to the 13countries in which they both implement MNCH.15Most of the disparities in MNCH in the top five countries inneed are found within ethnic groups, especially indigenouspopulations. In Bolivia, Guatemala, Guyana, Hondurasand Panama, the worst statistics for maternal and childindicators are found in districts or zones with high levels ofindigenous populations.Recommendation: Develop Red Cross Red Crescent tools toaddress MNCH issues in indigenous communities. SupportNational Societies to develop an indigenous MNCH strategyfor areas with high levels of indigenous populations.9
10MNCH in the Americas A report on the commitments to women’s and children’s healthMethodsThe following types of interventions were used:Survey: A survey composed of various questionsaddressing MNCH programming (and other relatedprogrammes) was sent to all 35 National Societies in theAmericas. The survey was also sent to several PartnerNational Societies and overseas branches in the Caribbean.The survey encompassed questions about governments’commitments to MNCH and the relationship betweengovernments and National Societies to determine howa National Society perceives the government’s work. Toaddress any potential bias on the part of the NationalSocieties, a separate literature review was conductedto confirm governments’ commitments to MNCH. Thesurvey was developed in Spanish, French and Englishand distributed online (using Google docs) and by e-mail(Microsoft Word document format).Formal interviews: Interviews were conducted withkey stakeholders in MNCH in the Americas region such asNational Societies, Partner National Societies and externalpartners. The purpose of the interviews was to get morein-depth information on programming or policies they maybe implementing. Most of the interview questions were sentby e-mail and some were conducted in person.Formal and informal meetings: Meetings were heldwith internal and external experts on the subject matter tohelp direct research on the topic of MNCH or their specificarea of expertise (e.g. water and sanitation, nutrition,violence prevention, HIV prevention etc.)Literature/report review: A literature/report reviewwas conducted to analyse the current policies andstrategies being put forth by various actors in MNCH (e.g.IFRC’s Strategy 2020, PAHO MNCH strategy, etc.). A review ofexisting government health strategies or policies was alsoconducted to complement National Societies’ responseson government commitment from the survey. Most of thisresearch was internet based and the rest was conducted bycontacting National Societies, Partner National Societiesand other actors on the subject matter.Statistics research: Research was conducted to findthe statistics for the main MNCH indicators in order toidentify the needs of every country. Data from the WorldHealth Organization (WHO), United Nations Children’s Fund(UNICEF), the Joint United Nations Programme on HIV/AIDS(UNAIDS), the Pan American Health Organization (PAHO)and the United Nations Development Programme (UNDP)was used to acquire
the pan American health organization (pAho), founded in 1902, is the world's oldest international public health agency. it provides technical cooperation and mobilizes partnerships to improve health and quality of life in the countries of the Americas. pAho is the specialized health agency of the inter-American system and serves