Transcription
BONE GRAFTSURGERY1
BONE GRAFTSURGERY
S PECIAL THAN KS TO:Subject Matter Experts: Ron Aronovich, DMD, and Brent Golden, DDS, MDEditors in Chief: Ron Aronovich, DMD, Angela J. Dixon, MAand Lynn Fox, MA, MEd, CCC-SLPManaging Editor: Ron Aronovich, DMDAssociate Editors: Angela J. Dixon, MA, Martha S. Matthews, MD,and Sherard A. Tatum, MDMedical Illustrator: Marie Rossettie, CMIWriting Consultant: Amy F. Mendillo, MM, MPPMembers of the ACPA Learning Resources CommitteeCopyright 2019 by the American Cleft Palate-Craniofacial Association. All rightsreserved. This publication is protected by copyright. Permission should be obtainedfrom the American Cleft Palate-Craniofacial Association prior to any reproduction.
TABLE OF CONTENTSWHAT IS AN ALVEOLAR CLE FT?2WHAT AR E TH E G OALS FOR B ON E G RAFT SU RG E RY?2HOW DO WE KNOW IF A CHILD NEEDS THIS SURGERY?3AT WHAT AG E DOES TH IS SU RG E RY TAKE PLACE?3WHAT IS MAXI LLARY EXPANSION?4WHAT HAPPE NS DU R I NG B ON E G RAFT SU RG E RY?4WH E R E DOES TH E N EW B ON E COM E FROM?4WHY AR E B R USH I NG AN D FLOSSI NG I M PORTANT?7WHAT HAPPE NS I N TH E HOSPITAL?7HOW DOES A SPLI NT H E LP WITH H EALI NG?8WHAT CAN A PATI E NT EAT AFTE R SU RG E RY?9WH E N WI LL A CH I LD R ESU M E R EG U LAR ACTIVITI ES?9WAS TH IS SU RG E RY A SUCCESS?9FOR MOR E I N FOR MATION111
WHAT IS AN ALVEOLAR CLEFT?Sometimes, a child born with a cleft lip also has a cleft in the gum line.Instead of having a smooth upper gum line, there is a gap just abovethe teeth. The bone under the gum line is called the alveolar ridge. Thegap is called an alveolar cleft. An alveolar cleft originates near the teethand can extend all the way up to the nose. Just like a cleft lip, an alveolarcleft can happen on one side of the mouth or on both sides.An alveolar cleft needs to be closed. Bone graft surgery, also calledalveolar cleft repair, closes the spaces in the bones beneath the gums.It also closes the spaces in the gums themselves.Figure 1: Bilateral alveolar cleftFigure 2: Before bone graft surgeryFigure 3: After bone graft surgeryWHAT ARE THE GOALS FORBONE GRAFT SURGERY?In order for adult teeth to grow in properly, they need to be anchoredin bone. Bone graft surgery creates a stable maxilla (upper jaw), whichgives the teeth a place to grow. Without a strong upper jaw, severalthings could happen. The adult incisor and canine teeth could fall out. Thehealthy teeth around the cleft area could become crowded and crooked.The gums could get irritated. Later on, braces may not be effective.2
In addition to stabilizing the upper jaw, bone graft surgery also closesthe hole in the gum line. While a surgeon closes most of the openingbetween the mouth and the nose during cleft palate repair surgery (usually performed during a baby’s first year), a child may still have a cleftin the gum line. Closing the alveolar cleft will stop liquids, like drinks orsome foods, from leaking through the cleft in the gum line and comingout of the nose. It will also prevent food from getting caught in thatspace and will block air from escaping during speech. Bone graft surgery also increases bone support to the nose, which can make the noselook more symmetrical.HOW DO WE KNOW IF ACHILD NEEDS THIS SURGERY?An alveolar cleft can be mild for one child and severe for another.Even a mild cleft requires treatment. To learn about a child’s case, asurgeon will examine the mouth, gums, and teeth. Sometimes, thecleft is easy to see. Other times, it can only be found with a finger ora hand tool.The surgeon may take x-rays to learn about the size of the cleft andthe health of the teeth around it. X-rays may include regular plain filmsor a low-power CT scan called a cone beam CT scan.AT WHAT AGE DOES THISSURGERY TAKE PLACE?The timing of bone graft surgery depends in part on the growth of certain teeth. The top incisor and canine teeth are located in the front ofthe mouth, close to the site of the alveolar cleft (on one or both sides).The best time to do alveolar cleft repair is when those adult teeth areforming, but have not yet erupted (come in). This stage can happenbetween ages 6 and 12. The most common time is between ages 6and 9. Once the incisor and canine teeth erupt, they will need a strong,healthy bone as an anchor.The timing of the surgery also depends on a child’s other treatments,general health, mental health, height and weight. The surgeon andorthodontist on a child’s cleft team keep track of growth. Together, theydecide when the time is right to schedule this surgery.3
WHAT IS MAXILLARY EXPANSION?Treatment for alveolar clefts almost always includes orthodontic care. Itis common for a person born with an alveolar cleft to have an incorrectlyshaped upper jaw due to the cleft. Earlier palate repair surgery, too, canimpact the shape of the upper jaw. Orthodontic treatment moves theupper jaw into a correct “U” shape. It also aligns the top jaw with thebottom jaw. Most orthodontists do this treatment with a palate expander or another device. The process is called maxillary expansion.Some children receive maxillary expansion before bone graft surgery,others afterwards. The timing depends on a child’s age, the growthof his or her teeth, and the preference of the surgeon or orthodontiston the team. The surgeon and orthodontist on a child’s team will worktogether to coordinate this treatment. In most cases, maxillary expansion lasts 6 to 12 months. A second phase of orthodontic treatmentmay be needed afterwards, with braces.WHAT HAPPENS DURINGBONE GRAFT SURGERY?Bone graft surgery is performed by a surgeon on a child’s cleft team.The type of surgeon varies from team to team.For this procedure, a surgeon uses a small amount of healthy bone to patchthe space of the cleft. Sometimes, this bone is “borrowed” from somewhere else in the child’s body. In these cases, the surgeon’s first task is toremove a small amount of bone from the donor site (see below for details).Then, the surgeon operates on the alveolar cleft. To start, he or she separates the skin at the bottom of the nostril from the gums. The surgeonthen repairs the nostril skin and places the new bone material (sometimes referred to simply as the bone graft) into the space of the cleft.Last, the surgeon closes the gums with absorbable sutures (stitches).With time, the new bone and old bone will join and heal completely.WHERE DOES THENEW BONE COME FROM?The bone that fills an alveolar cleft can come from one of several places(each discussed in detail in the sections below). Most often, a surgeonuses a small piece of bone from somewhere else in the child’s body.4
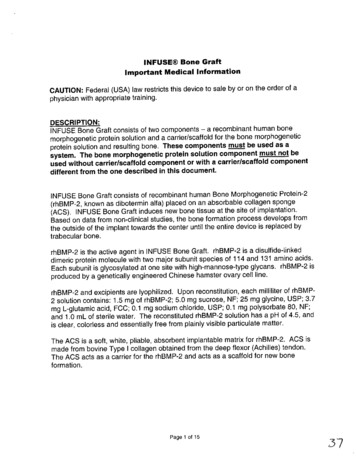
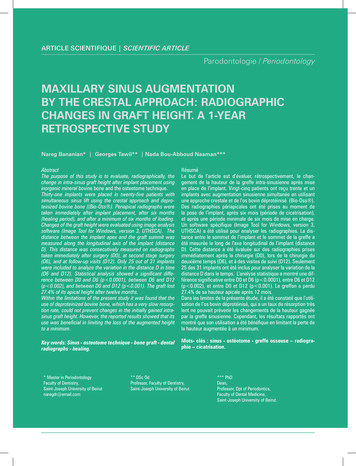
Bone from your own body is called autogenous bone. This bone usuallycomes from the hip, shinbone, lower jaw, top of the head, or ribs.Another method is to use bone from outside the body, called substitute bone. Substitute bone may come from a human cadaver (allograft),from an animal (such as a pig) or it may be man-made (synthetic bone).A third method does not involve borrowed bone at all. A surgeon maychoose to close an alveolar cleft with a protein that signals a child’sbody to grow new bone. When choosing a method, the surgeon considers the size of the cleft, the kind of bone needed, the health of thechild, and personal preference.BON E FROM TH E CH I LD’S BODYHip. The hip is the most common source ofbone used for alveolar cleft repair. The donorsite, located at the top, outer edge of the hip,is called the iliac crest (also called the wing ofthe pelvis). The bone of the iliac crest is plentiful and works well for grafting. To harvest thebone (remove it), the surgeon makes a 2-inchFigure 4: Iliac crest donor sitecut near the waistline.Removing bone from the hip can be painful. The pain is manageablewith painkillers, which in some cases are administered with a pain pump.Most children are able to stand or walk gently a few hours after surgery.The hip area may feel numb and must be watched for infection. At twoweeks, the skin incision is usually healed. At that point, most patientscan walk without difficulty.Shin. Sometimes a surgeon will close an alveolar cleftwith bone taken from a child’s shin (the tibia). The donorsite on the shin is called the metaphysis. It is part of thegrowth plate in the bone. This area contains slightly lessuseable bone than the hip. While the risks of harvestingthis bone are similar to the hip graft, recovery from thisprocedure may be shorter than for the hip.Figure 5: Shindonor siteMedical experts have shown concern that taking bonefrom the growth plate of growing child might cause problems with growth. However, some studies show goodresults and no growth problems.5
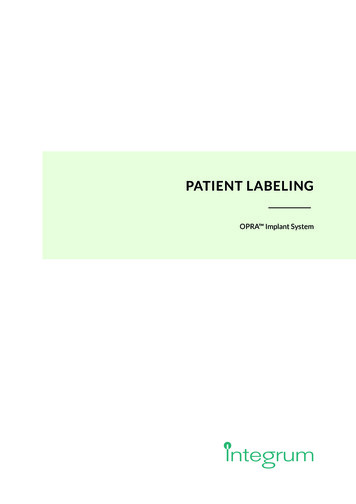
Jaw. A surgeon may decide to usebone from the lower jaw (the mandible) to fill an alveolar cleft. Amandibular bone graft comes fromthe bone near the front of the chin,just below the bottom teeth. Toremove this bone, a surgeon makes Figure 6: Donor sitesa cut on the inside of the mouth. This in the jaw bonesmethod works best when the alveolar cleft is small and only a smallamount of bone is needed. The risks include damage to the teeth andnumbness of the lip, chin and gums. However, this is a safe method toharvest bone, with few complications.Skull or ribs. In some cases, a surgeon closes the alveolar cleftwith bone from the child’s skull (a calvarial graft) or from the ribs.Bone from the skull comes from the outer surface of the head, eitherfrom the back of the head or near an ear. The rib site is located justbelow the breast. These two sites are used less often for alveolarcleft repair than the hip, shin, or lower jaw. They can be good optionsfor certain cases.BON E S U BSTITUTE SInstead of using bone from a child’s body, a surgeon may close analveolar cleft with substitute bone. Substitute bone has been usedsuccessfully for other types of bone grafts, such as the placement of afalse tooth. This bone comes from a deceased donor (a human cadaver), a different animal species (bovine or porcine), or from a man-madesource (synthetic). With substitute bone, a child avoids the risks andpain of bone harvesting. For this alveolar cleft repair, however, substitute bone may not heal as well as bone taken from the child’s body.BON E PROTE I N.Bone Morphogenic Protein, or BMP, is an alternative to autogenousbone or substitute bone. At times, it may be combined with substitute bone. BMP sends a signal to a child’s body to grow new bone.There are several types of BMP; the most common is called rh-BMP2.All BMPs are made in a lab, though BMP itself is present in one’sown bone.6
WHY ARE BRUSHING ANDFLOSSING IMPORTANT?A child with an alveolar cleft needs to have good dental hygiene. In theweeks and months before bone graft surgery, a child needs to brush andfloss thoroughly, three times a day, to keep the teeth and mouth clean.The cleft team recommends extra brushing and flossing for several reasons. A child with an alveolar cleft is at risk for certain problems withdental health. If a child has crowded teeth, for instance, bacteria canbuild up. Extra airflow from a cleft can dry out the mouth and invite bacteria, as well. An orthodontic device, like a palate expander, can also causeproblems with plaque and bacteria. Without good dental hygiene, a person is at risk for tooth decay, gum disease, infections, and loss of teeth.The health of the gums can affect the success of bone graft surgery.During surgery, a surgeon will close the gum tissue over the bone graft.Healthy gums are easy to sew. They bring good blood flow to the newbone and help with healing. When the gums are inflamed and unhealthy,they can become infected and break down. They can even cause achild to lose some or all of the bone graft.Even with extra brushing and flossing, a child may have trouble keepingthe mouth clean. A child should see a dentist regularly. The dentist willhelp make sure that the mouth is clean and healthy.WHAT HAPPENS IN THE HOSPITAL?Alveolar cleft repair is done in the operating room with full-body painrelief (general anesthesia). The surgery takes a few hours. Most children stay in the hospital for one or two nights afterwards.Anesthesia and surgery cause side effects. These include sore throat,nausea or vomiting, discomfort, swelling of the face and gums, bruising, difficulty speaking and swallowing, difficulty emptying the bladderor bowels, and constipation. These side effects are usually mild. Theyimprove in the first few days after surgery.A child usually needs pain relievers for about two weeks after bone graftsurgery. Common medications include anti-inflammatory medications(such as ibuprofen, with brand names Motrin or Advil), acetaminophen(brand name Tylenol), and stronger pain relievers such as opioids ornarcotics (such as hydrocodone or oxycodone).7
During the first two days after surgery, swelling gets worse before itslowly gets better. Swelling usually goes away completely in 3 to 4weeks. Walking on the hip is usually painful after surgery and might puta child at risk for falling. Some children need a walker or other assistance until they can walk on their own.In the hospital and during the first few weeks after surgery, there are afew ways to help with healing: Sleep on 2-3 pillows, to keep the head elevated Avoid blowing the nose Avoid pinching the nose when sneezing Avoid strenuous activity Maintain good dental hygieneHOW DOES A SPLINTHELP WITH HEALING?After surgery, the jaw needs to stay still so thatthe new bone will bond with the old bone andform a strong, healthy jaw. A splint is a devicethat keeps the upper jaw from moving. Somechildren with alveolar clefts on both sides mayneed to wear one after surgery.A splint looks like a retainer. It is made of acrylicand attaches to the upper teeth with wires. Asurgeon may recommend that a child wear thedevice for a few weeks to months after surgery.Wearing the splint can make eating and talkingdifficult. During this time, a child will follow a Figure 7: Splintstabilizing the upper jawspecial diet (see below for more information).A splint can cause plaque to build up on the teeth. A child’s orthodontistwill recommend ways to keep the teeth clean during this time. Sometimes, the orthodontist recommends using a small circular toothbrush,an electric toothbrush, a floss threader, or a special rinse. Patients withtooth decay may need a special fluoride treatment. Those with gum disease (called gingivitis) may need to have extra cleanings from a dentistbefore surgery and after the splint is removed.8
WHAT CAN A PATIENT EATAFTER SURGERY?It is important to prevent damage to the surgical site following alveolarcleft repair. For two to three weeks after the procedure, a child needsto follow a liquid diet. A surgeon will then approve a soft foods diet. Sixto eight weeks after surgery, a child will be cleared for a regular diet.A liquid diet includes only fluids. A juicer or blender can turn most fruits,vegetables and other foods into liquid shakes. When the child is clearedfor a soft foods diet, a blender or food processor will still be useful. Softfood options include mashed potatoes, yogurts, creamed soups, andanything else that can be blended. All liquid and soft foods should contain a good balance of carbohydrates, fats, and protein. A dietician isa professional who can give families ideas about calories and nutrition.WHEN WILL A CHILD RESUMEREGULAR ACTIVITIES?Most children need to be out of school for one to two weeks after surgery. After that, a child can go back to school, but usually with limitedactivity and no gym class. Six weeks after surgery, a child can resumenormal activities.While the body heals, a child should not do any strenuous activity suchas contact sports and heavy lifting. Surgeons do suggest walking andstretching. If the surgical procedure included bone removal from the hipor shinbone, a child may feel some pain in those areas. In some cases,a physiotherapist may suggest that a child use a walker.WAS THIS SURGERY A SUCCESS?After surgery, the gum tissue at the area of the bone graft should stayclosed. When the adult teeth come in, they should have good supportfrom inner bones and gums. Six to twelve months after surgery, a childmay have an x-ray called a radiograph. The radiograph shows if thebones have healed well.The success of a child’s bone graft surgery depends on a few factors.These include a child’s age, general health, whether the teeth enteredthe cleft site before surgery, the size and shape of the cleft, the healthof the gums, surgical technique, and other factors.9
In some cases, a bone graft may not be successful. When this happens,a surgeon usually recommends additional bone grafting. This decisionusually takes place at least 6 months after the first surgery.Treatments for alveolar clefts will vary from one cleft team to another.The surgeon on your child’s cleft or craniofacial team can give information on your specific case.10
FOR MORE INFORMATIONThis booklet and many others have been produced by:The American Cleft Palate-Craniofacial Association1504 East Franklin Street, Suite 102Chapel Hill, NC 27514919.933.9044 info@acpa-cpf.org www.acpa-cpf.org11
1504 E. Franklin St., Suite 102Chapel Hill, NC 933.9044
5 Bone from your own body is called autogenous bone.This bone usually comes from the hip, shinbone, lower jaw, top of the head, or ribs. Another method is to use bone from outside the body, called substi- tute bone.Substitute bone may come from a human cadaver (allograft), from an animal (such as a pig) or it may be man-made (synthetic bone).A third method does not involve borrowed bone at all.