Transcription
FINAL PROGRAM55th Annual Meeting of theHealth Physics Society(American Conference of Radiological Safety)22nd Biennial Campus RadiationSafety Officers Meeting27 June - 1 July 2010Salt Palace Convention CenterSalt Lake City, Utah
8:30 AM-Noon150 ABCWAM-E: NCRP SpecialSession - Overview of CurrentReport and ConferenceActivities of the NationalCouncil on RadiationProtection and MeasurementsCo-Chairs: Thomas Tenforde, Richard Toohey8:30 AMWAM-E.1Overview of Current Report andConference Activities of NationalCouncil on Radiation Protection andMeasurements (NCRP)Tenforde, T.S.National Council on Radiation Protection and MeasurementsReports of Program Area Committee 1 on Basic Criteria, Epidemiology, Radiobiology and Risk9:00 AMWAM-E.2Scientific Committee 1-16 Reporton “Uncertainties in the Estimationof Radiation Risks and Probability ofDisease Causation”Hoffman, F.O.SENES Oak Ridge, Inc.9:15 AMWAM-E.3Scientific Committee 1-17 Report on“Second Cancers and Cardiopulmonary Effects after Radiotherapy”Gilbert, E.S., Travis, L.B.National Cancer Institute, Universityof Rochester Medical CenterReports of Program Area Committee 2 on Operational RadiationSafety9:30 AMWAM-E.4Scientific Committee 2-3 Report on“Fluoroscopically Guided Interventional Procedures”Balter, S.Columbia University
9:45 AMWAM-E.5Report No. 162 on “Self Assessment of Radiation Safety Programs”Myers, D.S.Lawrence Livermore Laboratory,LivermoreReports of Program Area Committee 4 (PAC 4) on RadiationProtection in Medicine10:00 AMBreak in Exhibit Hall10:30 AMWAM-E.6Overview of Current NCRP Activities in Radiation Protection in MedicineBushberg, J.T.University of California, Davis HealthSystem10:45 AMWAM-E.7Scientific Committee 4-2 Report on“Population Monitoring and Radionuclide Decorporation Following aRadiological or Nuclear Incident”Vetter, R.Mayo ClinicReports of Program Area Committee 5 on Environmental Radiation and Radioactive WasteIssues11:00 AMWAM-E.8Scientific Committee 5-1 Report on“Approach to Optimizing DecisionMaking for Late-Phase Recoveryfrom Nuclear or Radiological Terrorism Incidents”Chen, S.Argonne National Laboratory11:15 AMWAM-E.9Scientific Committee 64-22 Reporton “NCRP Scientific Committee 6422: Design of Effective RadiologicalEffluent Monitoring and Environmental Surveillance Programs”Kahn, B.Georgia Institute of TechnologyReports of Program Area Committee 6 on Radiation Measurements and Dosimetry11:30 AMWAM-E.10Summary of NCRP Report No. 158:“Uncertainties in the Measurementand Dosimetry of External Radiation”Simon, S.L., Beck, H.L.National Cancer Institute11:45 AMWAM-E.11Scientific Committee 6-3 Report on“Uncertainties in Internal RadiationDose Assessment”Bouville, A., Bell III, R.National Cancer Institute
Overview of Current Report andConference Activities of NCRPThomas S. TenfordePresidentNCRP Special Session55th Annual Health Physics Society MeetingSalt Lake City, UtahJune 30, 2010
NCRP History1929: U.S. AdvisoryCommittee on X-rayand RadiumProtection1946: U.S. NationalCommittee onRadiation ProtectionLauriston Sale TaylorJune 1, 1902 – November 26, 20041964: NationalCouncil on RadiationProtection andMeasurements(NCRP) chartered byU.S. Congress
Key Elements of NCRP’s CharterUnder U.S. Public Law 88-376Cornerstones of role in radiation healthprotection:1. Provide information and recommendations inthe public interest about:a. protection against radiation; andb. radiation measurements, quantities and units.2. Develop basic concepts of radiation protection;3. 3) Facilitate effective use of combined resourcesof organizations concerned with radiationprotection;4. Cooperate with national and internationalgovernmental and private organizations; and5. Disseminate the results of the Council’s work.
Focal Areas of NCRP Reports and ConferencesHomeland resRadiationProtectionin MedicineRadiationDosimetry &MeasurementsRadiation Bioeffects:Mechanisms &Dose ResponseOperational &EnvironmentalRadiation SafetyNuclear Energy &Health/EnvironmentalProtection
NCRP Strategic Program Plan
NCRP Publications on Nuclearand Radiological TerrorismDetection of Terrorist Weapons & Materials: Commentary No. 16: Screening of Humansfor Security Purposes Using Ionizing RadiationScanning Systems (2003) Commentary No. 17: Pulsed Fast NeutronAnalysis System Used in Security Surveillance(2003) Commentary No. 20: Radiation Protection andMeasurement Issues Related to CargoScanning with Accelerator-Produced HighEnergy X Rays (2007)
NCRP Publications on Nuclear andRadiological Terrorism (cont.)Detection of Terrorist Weapons & Materials:In 2009-2014 NCRP is preparing a series of sixCommentaries (2) and Reports (4) on RadiationHealth Protection Aspects of the U.S. Department ofDefense Program to Develop Active DetectionTechnologies (ADTs) for Nuclear and RadiologicalMaterials That Represent a Threat to NationalSecurity [ADT methods under consideration includehigh-intensity bremsstrahlung radiation,monoenergetic gamma rays, and particulateradiations including neutrons, protons, and muons]
NCRP Publications on Nuclear andRadiological Terrorism (cont.)Countermeasures to Terrorism Acts: Report No. 138: Management of TerroristEvents Involving Radioactive Material (2001) Commentary No. 19: Key Elements ofPreparing Emergency Responders forNuclear or Radiological Terrorism (2005) Proceedings of 40th Annual NCRP Meeting(April 14-15, 2004): Advances inConsequence Management for RadiologicalTerrorism Events [published in HealthPhysics, Vol. 89(5), 2005]
NCRP Publications on Nuclearand Radiological Terrorism (cont.)Countermeasures to Terrorism Acts: Report No. 161 (2 volumes – Handbook andScientific and Technical Bases): Management ofPersons Contaminated with Radionuclides(2008) Report No. 165: Responding to Radiological andNuclear Terrorism: A Guide for DecisionMakers (2010) Report of Scientific Committee 4-2: PopulationMonitoring and Radionuclide DecorporationFollowing a Radiological or Nuclear Incident(publication expected in 2010)
NCRP Publications on Nuclear andRadiological Terrorism (cont.)Late-Phase Recovery from an Act ofTerrorism: Report of Scientific Committee 5-1:Approach to Optimizing DecisionMaking for Late-Phase Recovery fromNuclear or Radiological TerrorismIncidents (publication expected in 2013)
Radiation Protection in Medicine Report No. 155: Management ofRadionuclide Therapy Patients (2006) Report No. 159: Risk to the Thyroidfrom Ionizing Radiation (2008) Proceedings of the 43rd Annual NCRPMeeting (April 16-17, 2007): Advancesin Radiation Protection in Medicine[published in Health Physics, Vol.95(5), 2008]
Radiation Protection in Medicine (cont.)Reports in preparation: Scientific Committee 1-17: Second Cancersand Cardiovascular Effects AfterRadiotherapy (publication expected in 2010) Scientific Committee 2-3: Radiation DoseManagement for Fluoroscopically GuidedInterventional Medical Procedures(publication expected in 2010) Scientific Committee 4-3: DiagnosticReference Levels in Medical Imaging:Recommendations for Application in theUnited States (publication expected in 2011)
Radiation Protection in Medicine (cont.)Reports in preparation (cont.): Scientific Committee 4-4: Adverse Effects ofRadiation on the Gonads, Embryo, and Fetus(publication expected in 2011) Summary of Workshop on ComputedTomography in Emergency Medicine:Ensuring Appropriate Use (September 23-24,2009); basis for 2010 consensus paper on“Guidelines for Application of ComputedTomography in Emergency Medicine”
Dosimetry and Measurements Report No. 156: Development of a BiokineticModel for Radionuclide-Contaminated Woundsand Procedures for Their Assessment, Dosimetryand Treatment (2006) Report No. 158: Uncertainties in theMeasurement and Dosimetry of ExternalRadiation (2007) Report No. 163: Radiation Dose Reconstruction:Principles and Practices (2009) Report No. 164: Uncertainties in InternalRadiation Dosimetry (2009)
Operational Health andEnvironmental Radiation Protection Report No. 152: PerformanceAssessment of Near-Surface Facilitiesfor Disposal of Low-Level RadioactiveWaste (2005) Report No. 154: Cesium-137 in theEnvironment: Radioecology andApproaches to Assessment andManagement (2006) Report No. 157: Radiation Protection inEducational Institutions (2007)
Operational Health and EnvironmentalRadiation Protection (cont.) Report No. 162: Self Assessment ofRadiation Safety Programs (2010) Scientific Committee 64-22: Design ofEffective Effluent Monitoring andEnvironmental Surveillance Programs(publication expected in 2011) Report of Scientific Committee 2-5:Investigation of Radiological Incidents(publication expected in 2012)
Fundamental Radiobiologyand Health Protection Scientific Committee 1-13: Potential Impact ofIndividual Genetic Susceptibility and PreviousRadiation Exposure on Radiation Risk forAstronauts (publication expected in 2010)Scientific Committee 1-16: Uncertaintiesin the Estimation of Radiation Risks andProbability of Disease Causation(publication expected in 2011)Scientific Committee 1-20: Variation inBiological Effectiveness of Photons as aFunction of Energy (publication expectedin 2013)
NCRP’s Strategic Initiative on Biological andHuman Health Effects of Low-Dose Radiation Primary Goal: Prepare definitive publication(s)during 2011 to 2016 on biological effects andpotential human health implications of exposure tolow dose and low dose-rate radiation; planningworkshop held at NCRP on December 1-2, 2008 Important topics under consideration include:– up-to-date reviews of laboratory and humanepidemiology studies– effects of radiation quality and dose rate– integration of results into reliable, predictivemodels of human health effects at low doses– health protection and regulatory implications offindings, and effective communication ofprojected risks of low-dose radiation exposure
Areas of Increasing Importance to NCRP are theSafety, Health and Environmental Protection Aspectsof a Growing Nuclear Industry Worldwide(Proceedings of 2009 Annual Meeting to bepublished in Health Physics in 2010)
NCRP’s Primary Role in RadiationHealth Protection GuidanceThe hallmark of NCRP activities is providing reliablerecommendations for radiation protection policies andpractices based on scientific consensus View NCRP website at http://NCRPonline.org View and purchase NCRP publications athttp://NCRPpublications.org Proceedings of 2010 Annual Meeting: Communicationof Radiation Benefits and Risks in Decision Making willbe published in Health Physics in 2011 NCRP 2011 Annual Meeting: Scientific and PolicyChallenges of Particle Radiations in Medical Therapyand Space Missions March 7-8, 2011 at Hyatt Regency Conference Centerin Bethesda, Maryland
ScientificCommittee 1-16Uncertainties in Estimationof Radiation Risks andProbability of CausationF. Owen HoffmanSENES Oak Ridge, Inc102 Donner Dr.Oak Ridge, TN 37830
Members of NCRPSC 1-16 Julian Preston(Chair) John Boice Roy E. Shore Gayle Wolschak Bertrand Brill Owen Hoffman(Advisor) RanajitChakraborty Charles Land(Advisor) Rory Conolly David C. Kocher Richard Hornung
Objectives of NCRPSC 1-16 Analyze uncertainty relatingabsorbed organ doses to the risk ofdisease– Including cancer, non-cancer, and severegenetic defects Build upon recent NCRP reports thataddress uncertainty in– External dose (SC 6-1)– Internal dose (SC 6-3)– Dose reconstruction (SC 6-4)
Uncertainties Addressed byNCRP SC 1-16 Extrapolation of risk from the LifeSpan Study (LSS) of Japan– to the US and other populations withbaseline rates different than in Japan Extrapolation of risk from acuteexposure– to chronic and fractionated exposures Extrapolaton of risks from exposureto external radiation sources– to exposure to internal emitters
Sources of UncertaintyAddressed by NCRPSC 1-16 Extrapolation of risk estimatesfrom high energy gamma rayexposures to situations involving– low energy photons– low energy electrons– neutrons of various energies– alpha particles
Evaluation of Uncertainties Modify or reduce uncertainty in riskestimates by– combining information from epidemiologyand biological studies– combining information from multipleepidemiological cohorts using meta andpooled analyses Evaluate effect of dose uncertaintyon risk estimation– Size, shape, and confidence interval of thedose-response function
Evaluation of Uncertainties Contrast uncertainties for risks toindividual organs with– Risks to related groups of organs– Risks to all tumors combined fromuniform whole body exposure Evaluate methods to quantifycombined uncertainty in risk from– Uncertainty in dose– Uncertainty in risk per unit dose
Evaluation of Uncertainties Evaluate risk and uncertainty– using mortality versus morbidity as riskendpoint Evaluate uncertainty in lifetime risksfor populations versus subgroups– subgroups identified by age, sex, lifestyle,and other factors affecting the baselinerisk Evaluate the effect of variations inbaseline risks for differentpopulation subgroups
Evaluation of Uncertainties Uncertainty in risk depends onassessment objectives– Lifetime risk to populations vs. subgroupsvs. individuals– Probability of Causation/Assigned Share(PC/AS) for an individual with a specificdisease diagnosed in a given year Risk uncertainty in decision-making– Required by law (EEOICPA) for Federalradiation worker compensation program– Role of risk and uncertainty in situationsunrelated to compensation is less clear
Progress to Date withinNCRP SC 1-16 Work still in progress– internal drafting stage Once initial draft completed– it will be subjected to several rounds ofreview, revision, and editing before a finalreport is issued Some subjects will be referred toother committees for furtherevaluation– e.g., NCRP SC 1-20, risk of exposure tolow energy photons
National Cancer InstituteU.S. DEPARTMENTOF HEALTH ANDHUMAN SERVICESNational Institutesof HealthSC 1-17: SecondCancers and CardiacEffects AfterRadiotherapyEthel GilbertNational Cancer InstituteLois B. Travis, Chair SC-17University of Rochester Medical Center55th Annual Health Physics Society MeetingSalt Lake City, UtahJune 30, 20101
SC 1-17 Committee MembersLois B. Travis, ChairU. of Rochester Medical CenterJohn Boice, Vice-chair International Epidemiology InstituteKimberly ApplegateRiley Hospital for ChildrenLouis S. ConstineU. of Rochester Medical CenterAndrea NgBrigham and Women’s HospitalChing-Hon PuiSt. Jude’s Children’s HospitalXie George XuRensselaer Polytechnic InstituteEthel GilbertNational Cancer InstituteAnn KennedyU. of Pennsylvania Medical SchoolJoachim YahalomMemorial Sloan-Kettering Cancer Ct.James Allan, Consultant Newcastle U. Medical School
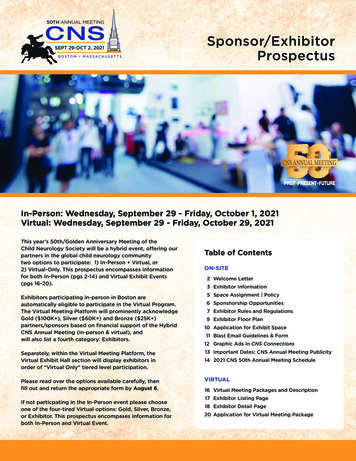
Patients with Cancer*5 y Relative Survival Rate* Cancer at all sites; all age, race and sex groups.
Cancer Survivorship: U.S. 12.1 million survivors as of 2007 Number has tripled since 1971 3% of U.S. population
Complications of Cancer andIts Treatment Medical (multiple organ systems) Second primary cancers Cardiac disease Hematologic, pulmonary, renal,endocrine, gonadalNeurologic, fatigue, weight gainPsychosocial (anxiety, depression)Societal (employment, insurance)
SC 1-17: Second Cancers andCardiac Effects After Radiotherapy“The primary purpose of this Reportis to provide a comprehensiveassessment of the risk of secondprimary cancers and cardiacdisease following radiotherapyamong the growing number ofcancer survivors worldwide.”
Sections of the Report1.2.3.4.5.Executive SummaryIntroductionRadiobiology and cancer biologyEpidemiologic MethodsNew Radiotherapy Methodologies andTechnologies6. Radiotherapy: Dosimetry7. Genetic underpinnings8. Second cancer risks in adults and children9. Dose-response relationships10. Cardiac effects11. Conclusions and recommendations
External Beam Radiotherapy Used in treatment of cancer since the1920’s Exposes not only the tumor butsurrounding tissues– Dose drops exponentially with distance fromtumor– Dose to nearby tissues can exceed 20 Gy,depending on tumor dose
Estimated Mean Dose (Gy) from35 Gy to Mantle or Inverted-YFields (Hodgkin Lymphoma)Organ or siteBrainLarynxThyroidBreastLungUpper esophagusLower 21
Changes in Radiotherapy Ability to concentrate energy depositionin the tumor has increased dramatically Modern treatment planning hasbenefitted by the ability to visualizetumors in 3 dimensions Has led to decreases in dose tosurrounding tissues
New Modalities of Radiotherapy Intensity modulated radiation therapy(IMRT)– Improved tumor coverage– Reduced high dose to normal tissues– Increased medium/low-dose exposure Proton and heavy ion therapyTomotherapyGamma knife and cyber knifeElectron beam therapyNeutron therapy
Epidemiologic Studies toEvaluate Second Cancer Risk Long-term follow-up necessary– Can not directly evaluate risks of most recenttreatments Direct study needed because of verylarge doses
Epidemiologic Studies toEvaluate Second Cancer Risk Cohort Studies– Defined group of 1st cancer survivorsfollowed for subsequent cancer– Limited treatment data– Evaluate patterns of risk by site, gender,latency, age at exposure, attained age Case-Control Studies– Study cases and sample of matched controls– Collect detailed treatment data– Dose-response analyses
Findings from Cohort Studies Little evidence of radiotherapy-relatedrisk until at least 5 years after 1st cancerdiagnosis Excess risk can persist for 30 years Relative risks are largest for patients whoare young at 1st cancer diagnosis Absolute risks increase with increasingattained age
Primary Cancers and RadiationRelated Second CancersPrimarycancerSecond cancers associated with radiationtherapyHodgkinlymphomaBreast, lung, esophagus, stomach, pancreas,colorectal, skin, thyroid, sarcoma, head and neck,mesothelioma, leukemiaTesticularcancerLung, thyroid, esophagus, stomach, pancreascolorectal, renal, bladder, sarcoma,mesothelioma, leukemiaBreastcancerContralateral breast, lung, sarcoma, esophagus,leukemiaProstateBladder, colorectal, sarcomaCervicalBladder, renal, rectal, uterine, ovarian, leukemia
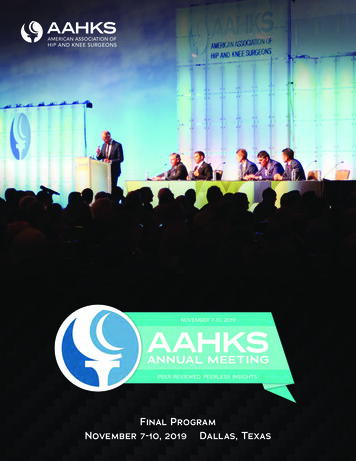
Case-Control Studies Report reviews studies with individualdose estimates for several 2nd cancers:– Leukemia, Breast, Lung, Thyroid, Bone,Brain Dose-response analyses– Quantify risk as a function of dose– Evaluate shape of dose-response Modification of dose-response by otherrisk factors such as chemotherapy,smoking, etc.
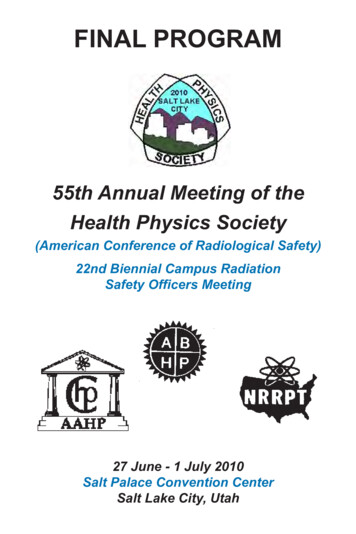
Dose-Response for LeukemiaFollowing Cervical Cancer(Boice et al. 1987)
Dose-Response for Breast CancerFollowing Hodgkin Lymphoma(Travis et al. 9/3020/3112/3117/29Relative Risk(95% CI)1.01.8 (0.7 – 4.5)4.1 (1.4 – 12)2.0 (0.7 – 5.9)6.8 (2.3 – 22)4.0 (1.3 – 13)8.0 (2.6 – 26)
Dose-Response for Thyroid CancerFollowing Childhood Cancer (Sigurdson et al. 2005)
Cardiac Disease Cardiac disease increased amongsurvivors of lymphoma, breast cancer,testicular cancer Effects of radiotherapy on cardiacdisease not as well studied as secondcancers Absolute risks could be large
Cumulative Incidence of Cardiac DisordersFollowing Childhood Cancer (Mulrooney 2009)
Overarching ResearchRecommendations Institute long-term and large-scale followup of existing cancer survivors– Children of special importance– Develop integrated measures to evaluate thelife-long burden according to prior treatment– Integrate epidemiologic studies with molecularand genetic approaches Establish prospective cohorts of cancerpatients– Newer treatments (e.g. IMRT, proton therapy)– Include biological samples
Areas of SpecificRecommendations Dose-response Adolescent and young adult cancersurvivors Molecular and genetic underpinnings Interactions between radiotherapy andother risk factors Comparison of risk of second cancersand cardiac disease after differentradiation modalities Risk prediction models
RADIATION DOSE MANAGEMENTFOR FLUOROSCOPICALLY GUIDEDINTERVENTIONAL MEDICAL PROCEDURES(NCRP Scientific Committee 2-3)Stephen Balter, Ph.D.(on behalf of the scientific committee)Health Physics Society - Salt Lake City – June 20101
Timeline and Status NOV/DEC 2009 – NCRP Program AreaCommittee Review FEB/MAR 2010 – NCRP Counciland Outside Review JUL 2010 – Pending Council Approval(subject to further revisions) Publication Expected in 3rd or 4thQuarter 2010
Intent Addressed to policy makers.Not a complete how-to handbook.Supplements other NCRP reports.Background material on clinicalprocedures is included. Related nonradiation risks arereviewed.
SC 2-3 Members Stephen Balter, Chair, Columbia UniversityDonald L. Miller, Vice Chair, USUHSBeth A. Schueler, Vice Chair, Mayo ClinicJeffrey A. Brinker, Johns Hopkins HospitalCharles E. Chambers, Penn State CollegeKennith F. Layton, Baylor University Medical CenterM. Victoria Marx, University of Southern CaliforniaCynthia H. McCollough, Mayo ClinicKeith J. Strauss, Harvard Medical SchoolLouis K. Wagner, U. of Texas Medical School
SC 2-3 Consultants John F. Angle, University of VirginiaLionel Desponds, GE HealthcareAndrew Einstein, Columbia UniversityJohn W. Hopewell, University of OxfordNorman J. Kleiman, Columbia UniversityMatthew Williams, Columbia University Marvin Rosenstein, NCRP Staff Consultant
Organization of the Report Executive Summary 31 Recommendations Main Sections–––––Clinical, Dosimetry, BiologyFluoroscopic Equipment and FacilitiesProtection of the PatientProtection of StaffAdministrative and RegulatoryConsiderations Appendices (12) References ( 425)
Uses ICRU Report 74 Style Notation Ka,r air kerma at thereference pointPKA air kerma-areaproductKa,i incident air kermaDskin,e entrance skin doseDtissue,max peak tissue dose
A Patient Undergoing an FGI ProcedureIs Not an ICRP “Average” PersonICRP populationPatient population M:F 1:1Reference sizeAll agesAverage healthAverage lifeexpectancyM:F variableVariable sizeOlderSick individualsDecreased lifeexpectancy
Patient Benefits of FGI Procedures Relief of symptomsImprovement in quality of lifeIncreased life spanDecreased morbidity and shorterrecovery time as compared to moreinvasive treatments
Risk Radiation risk should be one ofthe many risks included in therisk-benefit analysis of FGIprocedures.
Effective Dose Effective Dose (E) shall not be usedfor quantitative estimates ofstochastic radiation risk forindividual patients or patient groups.Effective dose (E) may be used as aqualitative indicator of stochasticradiation risk for classifying differenttypes of procedures into broad riskcategories.
Special Populations Equipment that is routinely used forpediatric procedures should beappropriately designed, equipped,and configured for this purpose. Procedure planning for FGIprocedures on pregnant patientsshall include feasible modificationsto minimize dose to the embryofetus.
Potentially-High Radiation DoseProcedures A FGI procedure should beclassified as a potentially-highradiation dose procedure if morethan 5 % of cases of that procedureresult in Ka,r exceeding 3 Gyor PKA exceeding 300 Gy cm2 . Potentially-high radiation doseprocedures should be performedusing equipment designed for thisintended use.
Patient Dose Records Patient dose data shall be recorded inthe patient’s medical record at theconclusion of each procedure. This shallinclude all of the following that areavailable from the system: Dskin,max, Ka,r,PKA, fluoroscopy time, number offluorographic images. Fluoroscopy time should not be used asthe only dose indicator during potentiallyhigh radiation dose FGI procedures.All available dose indicators shall beused in such procedures.
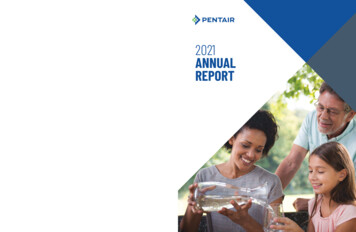
Fluoroscopy time is apoor dose metric ! 2,100noncardiac interventionsKa,r 0.41 0.037 FminR2 0.50 1,700coronary-artery proceduresKa,r 0.53 0.12 FminR2 0.68RAD-IR IIAEA-SRS 59
Substantial Dose Procedures I If a substantial radiation dose level isexceeded, the interventionalist shallplace a note in the medical record,immediately after completing theprocedure, that justifies the radiationdose level used.Default values: Ka,r 5 Gy PKA 500 Gy cm2 Fluoroscopy time 60 min
Substantial Dose Procedures II If a substantial radiation dose level is exceeded,the patient and any caregivers should beinformed, prior to discharge, about possibledeterministic effects and recommended followup. Follow-up for possible deterministic effects shallremain the responsibility of the interventionalistfor at least one year after an FGI procedure.Follow-up may be performed by anotherhealthcare provider.All relevant signs and symptoms shall beregarded as radiogenic unless an alternativediagnosis is established.
Patient Quality and SafetyManagement Facilities shall have a process to reviewall relevant radiation doses for patientsundergoing FGI procedures.Guidance levels, based on measureddosimetric quantities (in particular PKA orKa,r to manage stochastic effects andoverall performance, and Ka,r to managedeterministic effects) should be used forquality assurance purposes. Stochastic risk Deterministic injuries
Protective Barriers All spaces outside the procedure room(including control rooms) should be designedto limit E to not more than 1 mSv y 1. Spaces within the FGI-procedure room intendedexclusively for routine clinical monitoring ofpatients (or similar activities) should be shieldedto limit E to not more than 1 mSv y 1. Door interlocks that interrupt x-ray productionshall not be permitted at any entrances toFGI-procedure rooms.
Protection of Staff Determinations of occupational dosesshall take into account the personalprotective equipment used by eachindividual in the FGI environment. A collar monitor may be used to estimateequivalent dose to the lens of the eye if aworker exclusively uses under-table x-raygeometry; otherwise an eye dose monitorshould be placed on the collar or closerto the lens of the eye. A single personal monitor worn underthe protective apron shall not be used inthe FGI environment.
Dose Limits - Staff Policies and procedures shouldbe in place so that in the eventof a time-critical urgent oremergent situation, as definedin this Report, advancedprovision exists for exceedingan annual occupational doselimit.
Investigations Investigations should occur ifpersonal monitor readings foran individual are substantiallyabove or below the expectedrange for that individual’s duties.
Training, Privileges, andSupervision A FGI procedure shall be performed orsupervised only by a physician or othermedical professional with fluoroscopicand clinical privileges appropriate to thespecific procedure. Every person who operates or supervisesthe use of FGI-equipment shall havecurrent training in the safe use of thatspecific equipment.23
Equipment Quality Interventionalists and qualified physicistsshould participate in the process forpurchase and configuration of newfluoroscopes and fluoroscopy facilities. A qualified physicist shall performacceptance and commissioning testsbefore first clinical use of new, newlyinstalled, or newly repaired fluoroscopyequipment, and shall perform subsequentperiodic tests.24
5
NCRP Report No. 162Self Assessment ofRadiation SafetyProgramsDavid Myers, CHPLawrence Livermore National Lab
Program Area Committee 2:Operational Radiation Safety- Rpt.134 - Operational Radiation Safety Training (2000)- Rpt.144 - Radiation Protection of Particle Accelerators(2003)- Rpt.147 - Structural Shielding Design of Medical ImagingFacilities (2004)- Rpt.151 - Structural Shielding Design for PhotonRadiotherapy Facilities (2005)- Rpt.157 - Radiation Protection in Educational Institutions(2007)- Rpt.162 - Self Assessment of Radiation Safety Programs(2010)
Definition of Self Assessment Process that institution uses to review its own activitiesand performance in relation to:- Regulations- Standards- Internal policies- Implementing procedures- Best Practices- Goals Institution controls what is assessed and who does it Tailored to size and complexity of program
Why Should HP’s be Interested? Most operational HP’s have lots of experience in beingaudited or inspected Typically have less experience in assessing their ownprograms Useful for evaluating existing programs Good place to start on if you don’t have a program
General Objectives andSpecific Purposes of SA Identify and correct deficiencies and improveperformance Specific purposes- ensure a safe workplace- assess compliance- encourage continuous improvement- identify noteworthy practices- identify areas for further evaluation- provide opportunity for learning
Three Primary Types of Assessment Compliance-Based- does program meet regulations? Risk-Based- what could go wrong? Performance based- evaluates overall effectiveness and efficiency of program- most comprehensive of the three types of assessment
Institutional Responsibilitiesfor Self Assessment Upper management - provide support and resources Line Management - encourage worker participation Radiation Safety Program Personnel - develop andimplement SA program Workers - need to actively participate Minimize conflict-of-interest
Self Assessment Planning Selecting program elements to be assessed (e.g., externaldosimetry, training, ALARA program, contamination control) Establish the schedule to cover all program elements Is an external audit on the schedule? Reviewing past self assessment results Identifying the necessary resources
Methods and Techniques forPerforming Self Assessments Evaluate monitoring results
and Procedures for Their Assessment, Dosimetry and Treatment (2006) Report No. 158: Uncertainties in the Measurement and Dosimetry of External Radiation (2007) Report No. 163: Radiation Dose Reconstruction: Principles and Practices (2009) Report No. 164: Uncertainties in Internal Radiation Dosimetry (2009) Dosimetry and Measurements