Transcription
Department of Radiology2 01 2 Q ua l i ty R e p o rtACCESSSAFETYEXCELLENCESERVICE
Table of ContentsA Message from the Dean and CEO . 2A Message from the Chair . 3Chapter 1: Departmental Performance Measures . 5Chapter 2: Radiation Dose Optimization Program . 9Chapter 3: Quality Improvement Committee Projects . 15Quality Improvement and Measuring Outcomes: Radiologic-Pathologic Correlationin Acute Appendicitis . 17Standardization of Radiology Reports from NYU Langone MusculoskeletalImaging Specialty . 18Evaluation of Ultrasound for the Diagnosis of Appendicitis in Children . 20Radiology Patient Safety Interdisciplinary Seminars . 22Recommendations for Additional Imaging on Emergency Department (ED) CT Examinations . 23Monitoring Image Quality . 24CT Examination Contrast Extravasation Reporting . 25The Commitment to Process Improvement Continues . 26Chapter 4: Process Improvement . 27Impacting Key Performance Indicators in Our MRI Section through Process Improvement . 28Breast Imaging: Process Improvement and the Power of Change . 30Chapter 5: Patient Safety Training Program at NYSIM . 33Assessment and Treatment of Adverse Reactions to Intravenous Contrast Media . 34Chapter 6: Innovation: New Equipment and New After-Hours Access . 35MRI at NYU Langone . 36CT Imaging at NYU Langone . 37Role of Hybrid Imaging Modalities in Advancing Quality of Care:PET/MR, PET/CT and SPECT/CT at NYU Langone . 38Breast Imaging at NYU Langone . 40Center for Musculoskeletal Care . 42Expansion of Radiology Services . 43Chapter 7: Research Grants and Publications . 45Selected Research Grants . 46Selected Publications . 48Chapter 8: Referring Physician Survey . 53Chapter 9: Leadership . 55DEPARTMENT OF RADIOLOGY 2012 Quality Report 1
A Message from the Dean and CEOGuided by a clear vision and a series ofmeasurable performance goals, NYULangone Medical Center is uniquelypositioned to drive its tradition ofexcellence into all aspects of our growth.As public interest in healthcare quality andaccountability grows, we continue to define bestpractices by building upon our strong tradition ofexcellence in patient care, education and research.With quality and safety at its core, our model ofpatient-centered care includes a highly focusedprogram of process improvement along withthe ongoing investment in the technology andresources necessary to sustain success.Radiologic imaging plays an essential rolein supporting all of the medical and surgicalspecialties at NYU Langone and throughout thecommunity. It provides critical information andhelps inform the key medical decisions madeevery day.NYU Langone’s Department of Radiology ispassionately committed to this broad scope ofresponsibility. In the pages of this report, you willsee evidence of their commitment to quality alongwith concrete examples of the progress we aremaking. I think you’ll be impressed by the stepsthat have been taken to understand and addressthe level of excellence required in the areas ofquality, safety and service, not only from theperspective of our patients, but from those of ourphysicians, students, and other key stakeholdersas well.As a radiologist myself and former chair of theDepartment of Radiology, I am particularly proudof the work of the department under ChairMichael P. Recht, MD, The Louis Marx Professorof Radiology, and am pleased to present you withthe Department of Radiology 2012 Quality Report.Robert I. Grossman, MDThe Saul J. Farber Dean and Chief Executive OfficerNYU Langone Medical Center2 DEPARTMENT OF RADIOLOGY 2012 Quality Report
A Message from the ChairOver the past several years, innovativeimaging modalities have beendeveloped, including multichannelcomputed tomography (CT), high-fieldmultichannel magnetic resonance (MR),positron emission tomography-CT (PET-CT) andmost recently, PET-MR and minimally invasiveimaging-guided interventional procedures. Thesenew modalities have had significant impact onmedical practices and have allowed physicians tomore accurately and rapidly diagnose and treatpathology.Not surprisingly, they have also led to rapid growthin the volume of imaging procedures performed.This has had a significant effect on health carespending, and has also led to concerns regardingpatient’s radiation exposure. It is imperative thatradiologists and radiology departments take stepsto ensure that medical imaging is performedappropriately, with the least amount of radiationnecessary, and with maximum positive impact onpatients’ clinical outcomes.Over the past year, the Department of Radiologyat NYU Langone Medical Center has embarked onseveral initiatives to ensure that our departmentwill play a leading role in this effort. Moreover,we have implemented several new programs tomake patients’ visits and stays in our departmentas quick, pleasant and safe as possible. This efforthas been led by Danny C. Kim, MD, our directorof quality and patient safety; Jill E. Jacobs,MD, FACR, our associate director of qualityand patient safety; and Kirk Lawson, MBA, ouradministrative director of radiology. A task of thisimportance and magnitude, however, requireswidespread involvement and investment by theentire department in order to be successful, andI am pleased that this has happened in radiology.Staff from all areas of our team—technologists,receptionists, nurses, physician assistants,ombudsmen, residents, fellows, basic scientistsand faculty radiologists—have all contributedsignificantly to our effort. In the following pages,several of our initiatives and their results on ourperformance will be presented. I am proud of theprogress we have made in the past year and canassure everyone that our entire department iscommitted to continuing to be a national leader inthis effort.Michael P. Recht, MDThe Louis Marx Professor of RadiologyChair of the Department of RadiologyDEPARTMENT OF RADIOLOGY 2012 Quality Report 3
Welcome to theDepartment of Radiology2012 Quality Report.4 DEPARTMENT OF RADIOLOGY 2012 Quality Report
1DepartmentalPerformanceMeasuresDEPARTMENT OF RADIOLOGY 2012 Quality Report 5
1 departmental performance measuresDepartmental Performance MeasuresRecognizing the importance of time to patients and physicians, we’re making progress inreducing the amount of time patients need to spend in our department.Average Time Spent by Patients in the Department is defined as the time duration between the patientarrival time and the “end procedure” time stamp entered by the technologist.Average Time Spent by Patients in Our Department by 86360408175326129200Computed Radiography1Q / FY123Q / FY12CTMRINuclear MedicineMODALITY6 DEPARTMENT OF RADIOLOGY 2012 Quality ReportPETUltrasound
Simultaneously, our on-time performance record continues to improve.On-Time Performance: Outpatient CTPERCENTAGEOn-Time Performance is defined as thepercentage of cases starting within 30 minutesof the appointment time.9590858075706560714Q FY1174751Q FY122Q FY12MODALITY793Q FY1290734Q FY1177751Q FY122Q FY12MODALITY3Q FY1291N/A4Q FY11N/AN/A1Q FY122Q FY12MODALITY75691Q FY122Q FY12MODALITY3Q FY129590858075706560878178674Q FY111Q FY122Q FY12MODALITY3Q FY12959085807570656082684Q FY1170661Q FY122Q FY12MODALITY3Q FY12On-Time Performance: Outpatient PETPERCENTAGEPERCENTAGEOn-Time Performance: CMC* MRI95908580757065604Q FY1171On-Time Performance: Screening MammographyPERCENTAGEPERCENTAGEOn-Time Performance: Outpatient Ultrasound959085807570656071On-Time Performance: Clinical Cancer Center MRIPERCENTAGEPERCENTAGEOn-Time Performance: Outpatient MRI95908580757065603Q FY12959085807570656083N/A4Q FY11N/AN/A1Q FY122Q FY12MODALITY3Q FY12*Center for Musculoskeletal CareDEPARTMENT OF RADIOLOGY 2012 Quality Report 7
1 departmental performance measuresOur commitment to reducing turnaround time continues across all modalities and sites.The definition of Average Turnaround Time is defined as the time duration between the “endprocedure” time stamp entered by the technologist and the time when the report is signed by theattending radiologist. Graphs below are based on 3rd quarter FY 2012 ediatrics20010051283000NYU y Musculo- Neuro- Pediatrics NYUDept.skeletal ricsMODALITY8 DEPARTMENT OF RADIOLOGY 2012 Quality ReportNYULangoneNGR121Abdomen615860Breast ImagingPediatricsNYU Langone NGRMODALITY
2RadiationDoseOptimizationProgramDEPARTMENT OF RADIOLOGY 2012 Quality Report 9
2 radiation dose optimization programRadiation Dose Optimization ProgramThe safe use of radiation in imagingexaminations is one of the mostimportant challenges confronting theDepartment of Radiology. CT examinationsaccount for nearly 70% of the radiationexposure delivered by our department. Whilethe information gained from CT examinationscontributes greatly to patient care, we mustacknowledge the small risk of deleterious effects,including the risk of developing cancer. To date,the risk of developing cancer from small doses ofradiation delivered in typical imaging examinationsremains uncertain. Although controversial,currently accepted risk estimates derive primarilyfrom extrapolations based upon surveillance ofthe atomic bomb survivors in Japan. While theserisks are rather small compared to the population’sbaseline risk of developing cancer, the increasinguse of CT examinations and the multiplicity ofuse in many patients warrant the careful use ofradiation for the individual patient and the entirepatient population.10 DEPARTMENT OF RADIOLOGY 2012 Quality ReportA Commitment to SafetyOur department adheres to the principle ofALARA (as low as reasonably achievable) whenperforming CT examinations. This principleincludes two major components: justificationand optimization. First, the examination must bemedically indicated. Second, the examinationmust be performed with radiation dose as low asreasonably achievable for the diagnostic task. Ourdepartment is taking steps to be fully accountablefor appropriate CT radiation usage by creating aCT Radiation Dose Optimization Program. Wewill formally address other imaging modalitiessoon. Our department has affirmed our efforts tooptimize radiation dosage in imaging pediatric andadult patients by pledging to the Image Gently and Image Wisely public campaigns.Standardizing ProtocolsIn our department, the first step in our CTRadiation Dose Optimization Program wasstandardization of the imaging protocols used toscan patients for specific clinical indications. Forexample, a CT scan for hematuria is performedin the same manner no matter which radiologistis performing and interpreting the examinationor where in the medical center it is performed.A departmental CT protocol committee meetsregularly to ensure that imaging protocols are upto-date with the standard of care, and to ensurethat they incorporate the latest technologicaladvancements from the equipment vendors tooptimize our examinations.
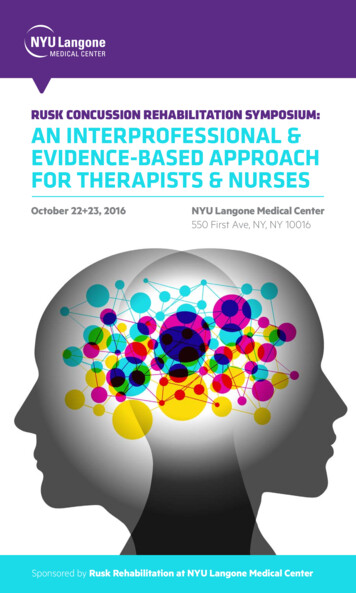
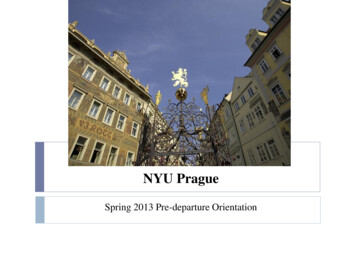
Reducing Variationunnecessarily higher on the first two scanners.When we adjusted the parameters to similarlevels as the third scanner, we achieved anapproximately 40% decrease in radiation doseon the first two scanners without sacrificingdiagnostic quality. Since that change, the radiationdose indices have been similar across the threescanners from 10/1/2011 to 5/1/2012 (Figure 2).The second step in our CT Radiation DoseOptimization Program was to standardize theradiation dose exposure for all the departmentalCT scanners for each protocol. The departmentinstalled a database to collect CT radiation doseindices from our CT scanners for each protocol.These data were analyzed to ensure that theradiation dose exposure was similar across ourCT scanners and imaging protocols. Throughthis evaluation, as an example, we found thatthe average radiation dose index, ComputedTomography Dosage Index (CTDI) (vol), for a CTscan of the sinuses was higher on two of ourscanners compared to the third from 5/1/2011 to9/1/2011 (Figure 1).Figure 3 below demonstrates our efforts in thestandardization of CT radiation dose indicesfor four of our most common CT examinationsperformed in our department on our five CTscanners for the first half of the calendar year 2012.Small differences in the mean dose indices may besecondary to multiple factors. In addition to patientbody habitus, scanner parameters and hardwareand software differences are important factors. Weare continually analyzing the data to ensure that ourscanner settings are optimized to achieve diagnosticquality images and deliver similar radiation dose.After confirming that the CT scanner with thelower dose index was producing diagnosticquality examinations, we compared the scannerparameters and found the settings to beFigure 1. Average CTDI (vol) 5/1/2011 to 9/1/2011BaselineFigure 2. Average CTDI (vol) 10/1/2011 to 5/1/2012Post-OptimizationSCANNER 1SCANNER 2SCANNER 3SCANNER 1SCANNER 2SCANNER 316.3(n 118)16.0(n 118)11.5(n 44)10.3(n 182)9.9(n 176)9.0(n 135)SCANNER CSCANNER DSCANNER EFigure 3. CTDI (vol) 2012 ComparisonSCANNER AMEASURESCANNER BMEANSDMEANSDMEANSDMEANSDMEANSDBrain .672.91Chest DEPARTMENT OF RADIOLOGY 2012 Quality Report 11
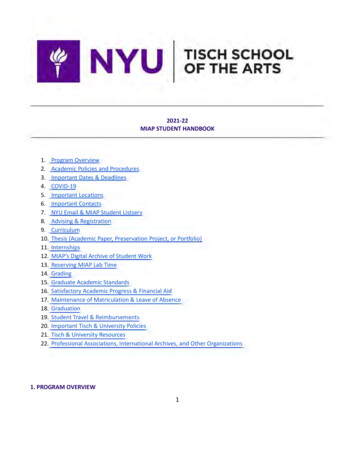
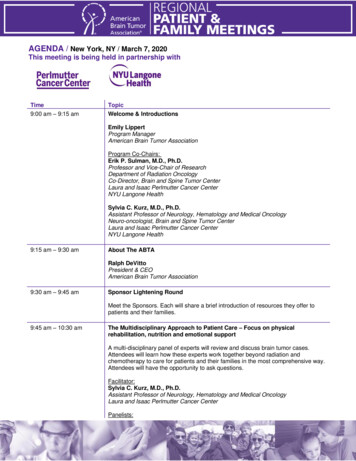
2 radiation dose optimization programBenchmarking Our DataThe third step in our CT Radiation DoseOptimization Program was to submit our CT doseindices into a national database, the AmericanCollege of Radiology’s Dose Index Registry, tocompare our departmental dose indices againstnational benchmarks. Thus far, we have receivedsome preliminary reports but await morecomprehensive information from this program.These results will allow us to compare ourradiation dose indices to benchmarks and help usto identify examinations that potentially may beperformed with lower radiation doses.Reducing ExposureThe fourth step in our CT Radiation DoseOptimization Program is to identify opportunitiesto reduce radiation dose without compromisingdiagnostic capability. Our clinical sectionsthat utilize CT have already been investigatingnumerous opportunities to reduce radiation dose.One of our noteworthy accomplishments hasbeen a collaborative effort with the Institute ofReconstructive Plastic Surgery to reduce radiationexposure in pediatric patients, who are the mostsusceptible to the potential deleterious effectsof radiation. Their evaluation of patients withcraniosynostosis necessitates performing a CTscan to determine their therapeutic strategy. Werealized that low-dose scout exams performedduring other neurological examinations producedgood quality images of the skull. We thereforeconsulted with our colleagues to determine ifthese low-dose images would be satisfactoryfor their evaluations. Figure 4 shows a skullimage comparison of a previous CT scan versusthe new low-dose CT scan. After getting theirapproval, we adopted this lower dose CT scan forthese pediatric patients, enabling a reduction inradiation exposure by 60% without compromisingdiagnostic image quality (Figure 5).Figure 4. High-dose CT skull image on the left and low-dose CT skull image on the right.12 DEPARTMENT OF RADIOLOGY 2012 Quality Report
Figure 5. This graph shows the CT radiation dose index, CTDI (vol), for our last 31 CT scansperformed for craniosynostosis:25CTDI (vol)2015FPO105Change inProtocol0135791113151719212325272931CT SCANSUsing a similar methodology, we have been ableto reduce radiation dose for lumbar spine CTscans. We realized that low-dose CT scans ofthe abdomen and pelvis produced good qualityimages of the lumbar spine. Our musculoskeletalradiologists reviewed these images and found theimage quality sufficient for making a diagnosis.Since then, we have implemented this low-doselumbar spine CT scan protocol.Increasing CollaborationOur department also works closely with ourequipment vendors to employ the latest hardwareand software advancements that enable usto further optimize radiation dosage withoutcompromising image quality. Several newproducts are currently being incorporated intoour routine clinical practice and are describedlater. Beyond optimizing CT scanning protocolsand incorporating new technology, we arecollaborating with our referring clinicians toperform only clinically indicated examinations,with the assistance of established imagingguidelines published by the American College ofRadiology known as the Appropriateness Criteria .We also collaborate with our referring cliniciansto identify opportunities to utilize non-radiationimaging examinations, such as ultrasound andMRI, to answer the clinical question. This closecollaboration between the clinical departmentsand our department will be vital to achievingthe goals of performing high-quality diagnosticimaging while utilizing the lowest radiation doseto aid clinical diagnosis.Danny C. Kim, MDAssistant ProfessorDirector of Quality and SafetyDEPARTMENT OF RADIOLOGY 2012 Quality Report 13
2 radiation dose optimization programOur departmentadheres to the principleof ALARA (as low asreasonably achievable)when performing CTexaminations.14 DEPARTMENT OF RADIOLOGY 2012 Quality Report
3QualityImprovementCommitteeProjectsDEPARTMENT OF RADIOLOGY 2012 Quality Report 15
3 Quality Improvement Committee ProjectsQuality Improvement Committee ProjectsOne of the key components of healthcaredelivery is diligent monitoring andassessment of patient care, safetyand adverse outcomes. The radiologydepartment at NYU Langone MedicalCenter has demonstrated its high level ofcommitment to this process by creating theQuality and Patient Safety Program. The two mainfacets of this program are committees chargedwith quality improvement and those charged withpatient safety.Subcommittees of the quality improvementcomponent include the Quality ImprovementCommittee, whose charge is the developmentand measurement of initiatives addressingstandardization of patient care, performanceoutcomes, and outcomes management; theOutcomes Management Committee, whose dutyis continual assessment and analysis of radiologyreporting outcomes; and the Best-In-PracticeCommittee, whose concern is modality-basededucation of scanning techniques and safetypolicies for physicians, nursing personnel andtechnologists.Subcommittees of the safety component includethe Patient Safety and Policy (PSP) Committee,charged with continual monitoring and analysis ofprocedural complications and adverse outcomes,as well as the establishment of policies ensuringcontinued patient safety and decreased patientrisk. Subdivisions of this committee include theMRI Safety Committee, responsible for developing16 DEPARTMENT OF RADIOLOGY 2012 Quality Reportand monitoring MRI safety policies, and theContrast Safety Committee, charged with thedevelopment and monitoring of policies to ensurestandardized, safe delivery of intravenous andoral contrast media. Toward this end, an additionalsubcommittee of the PSP Committee is theSimulation Training in Patient Safety and ContrastReaction (SIMS) Committee, responsible fortraining physicians and technologists to accuratelyrecognize and optimally treat contrast reactions.As the exposure of the United States populationto medical radiation continues to rise, another keycomponent of the PSP committee is the RadiationMonitoring Committee. This committee focuseson the continued analysis, standardization andoptimized reduction of radiation dose delivery forall of the patients served by our department.Improvement of patient safety, decreasing patientrisk and adverse outcomes, and lowering radiationdose are of paramount importance to all of theNYU Langone radiologists. We hope the workof these Quality and Patient Safety Programsdemonstrate our commitment to the physiciansand patients we serve.Following are some of our ongoing qualityinitiative and outcomes projects.Jill E. Jacobs, MD, FACRProfessorAssociate Director of Quality and Safety
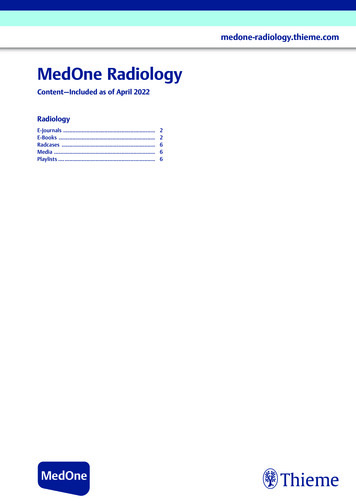
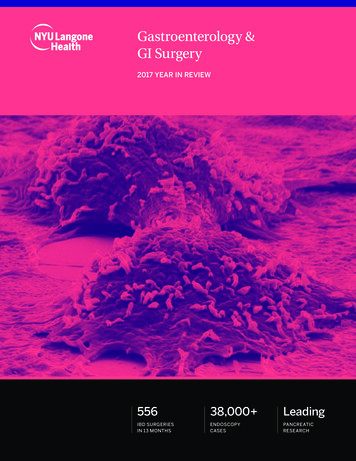
Quality Improvement and Measuring Outcomes:Radiologic-Pathologic Correlation in Acute AppendicitisMethods/Interventions: Data collected on 351 adult patients, of which“appendix” was primary submitted specimento pathology from 1/1/2011 to 12/31/2011. Primary data points: pathology specimendesignated as positive or negative and CTreport impression designated as positive,negative or indeterminate. Secondary data points: patient demographicsand associated findings reported on pathologyand CT reports.Problem:No standardized model exists that completely andaccurately measures performance, accuracy andoutcomes of radiologic diagnoses.Project goal:Evaluate accuracy of radiologic diagnosis ofacute appendicitis using radiologic and pathologiccorrelation with a long-term goal to establish astandardized, reproducible model to measureperformance and outcomes of various radiologicdiagnoses in real time.Progress to date:The positive predictive value of the CT diagnosisof appendicitis is 96%.Team members and roles: Martin Kopec, MD–Radiology Resident,Quality Improvement Committee member Courtney Cunningham–MSIV, NYU Schoolof Medicine Danny C. Kim, MD–Director of Qualityand SafetyLessons learned: Creating a system to perform follow-up on allpatients imaged for suspected appendicitis isdifficult. Using a single variable for evaluating trueperformance is incomplete.Next steps:Refine data collection process.Patient Outcomes351 TotalPatients82Excluded269Included50 PediatricCases32 AdultPatients17Referred fromOutside Hospital8DifferentModalityOutpatient CT atAnother Facility PATH2577Another Reason4 Pregnant – 3MRI/1 Ultrasound4 Othershad Ultrasound247Read Positive4Read asNegative-PATH129Read Positive1Read asNegative2IndeterminateSmall BowelObstruction6IndeterminateDEPARTMENT OF RADIOLOGY 2012 Quality Report 17
3 Quality Improvement Committee ProjectsStandardization of Radiology Reports from NYU LangoneMusculoskeletal Imaging SpecialtyProblem:Every radiologist in the Department of Radiology’sMusculoskeletal (MSK) Imaging Specialtygenerates a uniquely styled, dictated report forMRI examinations. Regardless of which radiologistis producing the report, the report provided to thereferring clinician should be similar.7. Which of the following do you prefer?ResponsePercentResponseCountStandardized radiology reportsfor all modalities including MRI,CT, radiographs, ultrasound, etc.71.4%20Project goal:Standardize the radiology report delivered fromNYU Langone MSK Imaging Specialty.Standardized radiology reportsonly for cross-sectionalmodalities (MRI, CT)10.7%3Team members and roles: Luis S. Beltran, MD–Project Leader Danny C. Kim, MD–Director of Qualityand SafetyNon-standardized radiologyreports for all modalities (i.e.,let the radiologist decide whathe/she wants to describe in thereport)17.9%5Interventions: Survey NYU Langone Medical Center MSKreferring clinicians to collect and analyzeinformation about the desired structure ofMRI radiology reports. Create MRI report templates for individualbody parts based on survey results to deliversimilarly dictated reports for every radiologist. Resurvey NYU Langone Medical Center MSKreferring clinicians to collect and analyzeinformation about their satisfaction with thestandardized MRI radiology reports. Readjust MRI report templates as neededbased on survey results to achieve optimizedstandardized reporting for our referringclinicians.18 DEPARTMENT OF RADIOLOGY 2012 Quality ReportProgress to date:The answers from the NYU Langone MedicalCenter referring clinicians for one of the mostsignificant questions asked in the initial survey aredisplayed in the chart.Lessons learned:The majority of the NYU Langone Medical Centerreferring clinicians sampled in the survey preferstandardized reports.Next steps: Implement standardized reports in clinicalpractice. Resurvey referring clinicians. Readjust report templates based on surveyresults as needed.
Referring Physician Survey (January 2012)1. In which division/subspecialty do you work?Response Percent Response tation6.9%2Other (please specify)6.9%22. Which of the following best describes what you prefer to read in the “Findings” section of the radiology report?List everything, including pertinent and non-pertinent positive and negative findings69.0%20List only pertinent positive and negative findings24.1%7List only pertinent and non-pertinent positive findings6.9%2List only pertinent positive findings0%03. Which of the following best describes what you prefer to read in the “Impression” section of the radiology report?List everything, including pertinent and non-pertinent positive and negative findings10.7%3List only pertinent positive and negative findings53.6%15List only pertinent and non-pertinent positive findings10.7%3List only pertinent positive findings25.0%7Attention to all details, including those that do and do not affect treatment decisions62.1%18Attention only to details that affect treatment decisions37.9%114. Which of the following is the most important to you when reading the radiology report?5. Which of the following examples of a hypothetical text describing a normal meniscus on MRI would you prefer in the“Findings” section of the radiology report?Menisci: within normal limits27.6%8Menisci: no evidence of tear or degenerative change31.0%9Menisci: no evidence of tear, degenerative change, extrusion, or parameniscal cyst41.4%126. In which of the following methods do you prefer the “Findings” section of the radiology report to be structured?By compartment (e.g., Medial compartment of the knee: within normal limits)60.7%17By tissue type (e.g., Cartilage: within normal limits)21.4%6Free text (i.e., no specific structure)17.9%5Standardized radiology reports for all modalities, including MRI, CT, radiographs, ultrasound, etc.71.4%20Standardized radiology reports only for cross-sectional modalities (MRI, CT)10.7%3Non-standardized radiology reports for all modalities (i.e., let the radiologist decide what he/she wants to describe in the report)17.9%57. Which of the following do you prefer?8. Would you like to be a representative of your division or group practice in a multidisciplinary committee designed tocreate standardized radiology reports?Yes (please e-mail luis.beltran@NYUMC.org if you are interested)14.3%4No, thank you85.7%24DEPARTMENT OF RADIOLOGY 2012 Quality Report 19
3 Quality Improvement Committee ProjectsEvaluation of Ultrasound for the Diagnosis of Appendicitis in ChildrenBackground:CT is the gold standard for imaging of appendicitisin adults. However, in children, due to theconcerns and risks of ionizing radiation, firstline imaging at our institution begins with anultrasound, reserving CT for inconclusive cases.This imaging strategy adheres to the As LowAs Reasonably Achievable (ALARA) principleand the American College of Radiology (ACR)recommendation for imaging of appendicitis inchildren.Project Goal:To assess the diagnostic accuracy of ultrasoundfor appendicitis in children and to identify thelimitations of this modality at our
in supporting all of the medical and surgical specialties at NYU Langone and throughout the community. It provides critical information and helps inform the key medical decisions made every day. NYU Langone's Department of Radiology is passionately committed to this broad scope of responsibility. In the pages of this report, you will