Transcription
Regence BlueShield: Silver Connect 4000 (73) Providence-Swedish HealthSummary of Benefits and Coverage: What this Plan Covers & What it CostsCoverage Period: 01/01/2017 – 12/31/2017Coverage for: Individual & Eligible Family Plan Type: PPOThis is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan documentat 73 or by calling 1 (855) 857-9959.Important QuestionsWhat is the overalldeductible?Are there otherdeductibles for specificservices?AnswersIn-network: 3,000 insured / 6,000 family percalendar year.Out-of-network: 8,000 insured / 16,000 familyper calendar year.Doesn’t apply to generic and preferred brand-namedrugs, pediatric vision services, and the followingin-network services: certain preventive care, primarycare and urgent care office visits, diagnostic xray/laboratory services, acupuncture visits, spinalmanipulations visits, and outpatient mental healthand substance abuse therapy visits. Copaymentsand amounts in excess of the allowed amount donot count toward the deductible.No.Yes. In-network: 5,500 insured / 11,000 familyIs there an out-of-pocketper calendar year.limit on my expenses?Out-of-network: Unlimited.What is not included in Premiums, balance-billed charges, and health carethe out-of-pocket limit? this plan doesn’t cover.Does this plan use anetwork of providers?Yes. See regence.com/PSHW or call 1 (855)857-9959 for lists of in-network or out-of-networkproviders.Do I need a referral tosee a specialist?No. You don't need a referral to see a specialist.Why this Matters:You must pay all the costs up to the deductible amount before this plan beginsto pay for covered services you use. Check your policy or plan document to seewhen the deductible starts over (usually, but not always, January 1st). See thechart starting on page 2 for how much you pay for covered services after youmeet the deductible.You don’t have to meet deductibles for specific services, but see the chartstarting on page 2 for other costs for services this plan covers.The out-of-pocket limit is the most you could pay during a coverage period(usually one year) for your share of the cost of covered services. This limit helpsyou plan for health care expenses.Even though you pay these expenses, they don’t count toward the out-of-pocketlimit.If you use an in-network doctor or other health care provider, this plan will paysome or all of the costs of covered services. Be aware, your in-network doctoror hospital may use an out-of-network provider for some services. Plans use theterm in-network, preferred, or participating for providers in their network. Seethe chart starting on page 2 for how this plan pays different kinds of providers.You can see the specialist you choose without permission from this plan.Questions: Call 1 (855) 857-9959 or visit us at 73.If you aren’t clear about any of the underlined terms used in this form, see the Glossary.You can view the Glossary at www.cciio.cms.gov or call 1 (855) 857-9959 to request a copy.WW0117SSLVCON407PRVIE
Are there services thisplan doesn’t cover? Yes.Some of the services this plan doesn't cover are listed on page 5. See your policyor plan document for additional information about excluded services.Copayments are fixed dollar amounts (for example, 15) you pay for covered health care, usually when you receive the service.Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if the plan'sallowed amount for an overnight hospital stay is 1,000, your coinsurance payment of 20% would be 200. This may change if you haven't metyour deductible.The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowedamount, you may have to pay the difference. For example, if an out-of-network hospital charges 1,500 for an overnight stay and the allowedamount is 1,000, you may have to pay the 500 difference. (This is called balance billing.)This plan may encourage you to use in-network providers by charging you lower deductibles, copayments and coinsurance amounts.Your Cost IfYour Cost If YouYou Use an InUse an Out-ofnetwork Providernetwork ProviderPrimary care visit to treat 45 copay / visit, other50% coinsurancean injury or illnessservices 30% coinsurance 65 copay / visit, otherSpecialist visit50% coinsuranceservices 30% coinsuranceIf you visit a healthcare provider’s office 45 copay / visit forOther practitioner officeor clinicacupuncture and spinal50% coinsurancevisitmanipulationsPreventive care/No charge50% coinsurancescreening/immunizationDiagnostic test (x-ray,30% coinsurance50% coinsuranceblood work)If you have a testImaging (CT/PET scans,30% coinsurance50% coinsuranceMRIs) 15 copay* / preferred generic retail prescriptionIf you need drugs to 30 copay / preferred generic mail order prescriptiontreat your illness or25% coinsurance* / nonGeneric drugsconditionpreferred generic retail prescription20% coinsurance / non-preferredMore informationgeneric mail order prescriptionabout prescription 50 copay* / retail prescriptiondrug coveragePreferred brand drugs 100 copay / mail order prescriptionCommon MedicalEventServices You MayNeedLimitations & ExceptionsCopayment applies to each in-network office visit only,deductible waived. All other services are covered at thecoinsurance specified, after deductible.Coverage is limited to 12 acupuncture visits / year.Coverage is limited to 10 spinal manipulations / year.Deductible –––––––––Deductible waived for in-network diagnostic x-ray andlaboratory ��–––––––––No coverage for prescription drugs not on the EssentialFormulary or prescription drugs from an out-of-networkpharmacy.Coverage is limited to a 90-day supply retail (1 copay per30-day supply) or mail order.Coverage is limited to a 30-day supply for injectabledrugs, specialty drugs and self-administrable cancerchemotherapy drugs.2 of 8WW0117SSLVCON407PRVIE
Common MedicalEventServices You MayNeedNon-preferred branddrugsis available atregence.com/formulary/2017/6tierEssentialWA.If you haveoutpatient surgeryIf you needimmediate medicalattentionSpecialty drugsYour Cost IfYour Cost If YouYou Use an InUse an Out-ofnetwork Providernetwork Provider50% coinsurance* / retail prescription45% coinsurance / mail order prescription40% coinsurance / preferredspecialty drug prescription50% coinsurance / non-preferredspecialty drug prescription20% coinsurance forFacility fee (e.g.,ambulatory surgicalambulatory surgerycenters;50% coinsurancecenter)30% coinsurance forother facilities20% coinsurance forambulatory surgicalPhysician/surgeon feescenters;50% coinsurance30% coinsurance forother facilitiesEmergency room services30% coinsuranceEmergency medical30% coinsurancetransportation 65 copay / visit, otherUrgent care50% coinsuranceservices covered the sameLimitations & ExceptionsDeductible waived for generic drugs and preferredformulary brand drugs and immunizations at aparticipating pharmacy.No charge for FDA-approved women’s contraceptivesprescribed by a health care provider.Coverage includes tobacco use cessation drugs whenobtained with a prescription order.The first fill is allowed at a retail pharmacy for specialtydrugs. Additional fills must be provided at a specialtypharmacy.Coverage for self-administrable cancer chemotherapydrugs is 30% coinsurance.Specialty self-administrable cancer chemotherapy drugsmust be purchased at a specialty pharmacy.* 5 off copayment or 5% off coinsurance discountwhen filled at a preferred ��none–––––––––––Copayment applies to each in-network urgent care visitonly, deductible waived.3 of 8WW0117SSLVCON407PRVIE
Common MedicalEventServices You MayNeedFacility fee (e.g., hospitalIf you have a hospitalroom)stayPhysician/surgeon feeMental/Behavioral healthoutpatient servicesMental/Behavioral healthIf you have mentalinpatient serviceshealth, behavioralhealth, or substance Substance use disorderabuse needsoutpatient servicesSubstance use disorderinpatient servicesPrenatal and postnatalcareIf you are pregnantDelivery and all inpatientservicesHome health careIf you need helprecovering or haveother special healthneedsYour Cost IfYou Use an Innetwork Provideras the If you have a testCommon Medical Event.30% coinsuranceYour Cost If YouUse an Out-ofnetwork Provider50% coinsurance30% coinsurance50% coinsurance 45 copay / visit, other50% coinsuranceservices 30% coinsurance30% coinsurance50% coinsurance 45 copay / visit, other50% coinsuranceservices 30% coinsuranceLimitations & ExceptionsCoverage is limited to 3,000 / day for inpatient nonemergency admission in out-of-network �––––––––––Copayment applies to each in-network outpatienttherapy visit only, deductible waived.Coverage is limited to 3,000 / day for inpatient nonemergency admission in out-of-network facilities.30% coinsurance50% coinsurance30% coinsurance50% coinsurance30% coinsurance50% coinsurance30% coinsurance50% coinsuranceRehabilitation services30% coinsurance50% coinsuranceHabilitation services30% coinsurance50% coinsuranceSkilled nursing careDurable medicalequipment30% coinsurance50% coinsuranceCoverage is limited to 130 visits / year.Coverage is limited to 30 inpatient days and 25outpatient visits / year.Coverage is limited to 3,000 / day for inpatient nonemergency admission in out-of-network facilities.Coverage for habilitative services is limited to 30inpatient days and 25 outpatient visits / year.Coverage for neurodevelopmental therapy is limited to25 outpatient visits / year.Coverage is limited to 3,000 / day for inpatient nonemergency admission in out-of-network facilities.Coverage is limited to 60 inpatient days / year.30% coinsurance50% �––––––––––Coverage is limited to 3,000 / day for inpatient nonemergency admission in out-of-network facilities.4 of 8WW0117SSLVCON407PRVIE
Common MedicalEventIf your child needsdental or eye careHospice serviceYour Cost IfYou Use an Innetwork Provider30% coinsuranceYour Cost If YouUse an Out-ofnetwork Provider50% coinsuranceEye examNo chargeNo chargeGlassesNo chargeNo chargeDental check-upNot coveredNot coveredServices You MayNeedLimitations & ExceptionsCoverage is limited to 14 respite days / lifetime.Coverage is limited to insureds under the age of 19.Coverage is limited to one routine exam / year.Coverage is limited to insureds under the age of 19.Coverage is limited to one pair of lenses (2 lenses) andone frame / �––––––––Excluded Services & Other Covered Services:Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.) Bariatric surgery Infertility treatment Routine eye care (Adult) Cosmetic surgery, except congenital anomalies Long-term care Routine foot care Hearing aids Private-duty nursing Vision hardware (Adult) Weight loss programs, except as covered underpreventive careOther Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for theseservices.) Acupuncture Chiropractic care Dental care (Adult) Termination of pregnancyNon-emergency care when traveling outside theU.S.5 of 8WW0117SSLVCON407PRVIE
Your Rights to Continue Coverage:Federal and State laws may provide protections that allow you to keep this health insurance coverage as long as you pay your premium. There are exceptions,however, such as if: You commit fraud The insurer stops offering services in the State You move outside of the coverage areaFor more information on your rights to continue coverage, contact the plan at 1 (855) 857-9959. You may also contact your state insurance department at 1 (800)562-6900 or www.insurance.wa.gov.Your Grievance and Appeals Rights:Contact the Washington State Office of the Insurance Commissioner at 1 (800) 562-6900 or www.insurance.wa.gov.Does this Coverage Provide Minimum Essential Coverage?The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provideminimum essential coverage.Does this Coverage Meet the Minimum Value Standard?In order for certain types of health coverage (for example, individually purchased insurance or job-based coverage) to qualify as minimum essential coverage, theplan must pay, on average, at least 60 percent of allowed charges for covered services. This is called the “minimum value standard.” This health coverage doesmeet the minimum value standard for the benefits it provides.Language Access Services:SPANISH (Español): Para obtener asistencia en Español, llame al 1 (855) �––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next –––––––6 of 8WW0117SSLVCON407PRVIE
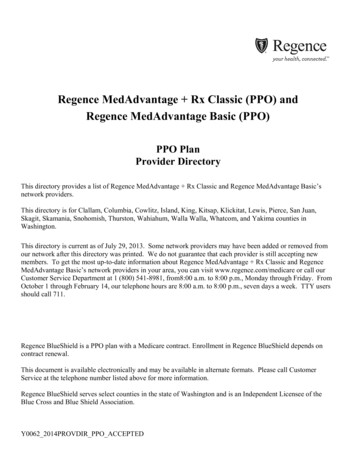
About these CoverageExamples:These examples show how this plan might covermedical care in given situations. Use these examplesto see, in general, how much financial protection asample patient might get if they are covered underdifferent plans.This isnot a costestimator.Don’t use these examples toestimate your actual costsunder this plan. The actualcare you receive will bedifferent from these examples,and the cost of that care willalso be different.See the next page forimportant information aboutthese examples.Having a babyManaging type 2 diabetes(normal delivery)(routine maintenance ofa well-controlled condition) Amount owed to providers: 5,400 Plan pays: 2,870 Patient pays: 2,530 Amount owed to providers: 7,540 Plan pays: 3,090 Patient pays: 4,450Sample care costs:Hospital charges (mother)Routine obstetric careHospital charges (baby)AnesthesiaLaboratory testsPrescriptionsRadiologyVaccines, other preventiveTotal 2,700 2,100 900 900 500 200 200 40 7,540Patient pays:DeductiblesCopaysCoinsuranceLimits or exclusionsTotal 3,000 20 1,280 150 4,450Sample care costs:PrescriptionsMedical Equipment and SuppliesOffice Visits and ProceduresEducationLaboratory testsVaccines, other preventiveTotal 2,900 1,300 700 300 100 100 5,400Patient pays:DeductiblesCopaysCoinsuranceLimits or exclusionsTotal 420 2,070 0 40 2,5307 of 8WW0117SSLVCON407PRVIE
Questions and answers about the Coverage Examples:What are some of the assumptionsbehind the Coverage Examples? Costs don’t include premiums.Sample care costs are based on nationalaverages supplied by the U.S. Department ofHealth and Human Services, and aren’t specificto a particular geographic area or health plan.The patient’s condition was not an excluded orpreexisting condition.All services and treatments started and endedin the same coverage period.There are no other medical expenses for anymember covered under this plan.Out-of-pocket expenses are based only ontreating the condition in the example.The patient received all care from in-networkproviders. If the patient had received carefrom out-of-network providers, costs wouldhave been higher.What does a Coverage Exampleshow?Can I use Coverage Examples tocompare plans?For each treatment situation, the CoverageExample helps you see how deductibles,copayments, and coinsurance can add up. It alsohelps you see what expenses might be left up toyou to pay because the service or treatment isn’tcovered or payment is limited. Yes. When you look at the Summary ofDoes the Coverage Example predictmy own care needs? No. Treatments shown are just examples.The care you would receive for thiscondition could be different based on yourdoctor’s advice, your age, how serious yourcondition is, and many other factors.Does the Coverage Example predictmy future expenses? No. Coverage Examples are not costestimators. You can’t use the examples toestimate costs for an actual condition. Theyare for comparative purposes only. Yourown costs will be different depending on thecare you receive, the prices your providerscharge, and the reimbursement your healthplan allows.Benefits and Coverage for other plans,you’ll find the same Coverage Examples.When you compare plans, check the “PatientPays” box in each example. The smallerthat number, the more coverage the planprovides.Are there other costs I shouldconsider when comparing plans? Yes. An important cost is the premiumyou pay. Generally, the lower your premium,the more you’ll pay in out-of-pocketcosts, such as copayments, deductibles,and coinsurance. You should alsoconsider contributions to accounts such ashealth savings accounts (HSAs), flexiblespending arrangements (FSAs) or healthreimbursement accounts (HRAs) that helpyou pay out-of-pocket expenses.Questions: Call 1 (855) 857-9959 or visit us at 73.If you aren’t clear about any of the underlined terms used in this form, see the Glossary.You can view the Glossary at www.cciio.cms.gov or call 1 (855) 857-9959 to request a copy.8 of 8WW0117SSLVCON407PRVIE
DISCRIMINATION IS AGAINST THE LAWThis Notice has Important Information. Regence complies with applicable Federal civil rights laws and does not discriminate onthe basis of race, color, national origin, age, disability, or sex. This notice has important information about your application orcoverage. Look for key dates in this notice. You may need to take action by certain deadlines to keep your health coverage or helpwith costs. You have the right to get this information, and other information about your application or coverage, in your ownlanguage at no cost. Call 855-857-9944. (TTY: 711)HELP IN OTHER LANGUAGESThe following translations help people who do not read English understand their rights and responsibilities and who to call for help.Including these translations is a federal requirement for all health plans sold on the state or federal marketplaces.Spanish: Este aviso tiene información importante. Regence cumple con las leyes de derechos civiles federales aplicables yno discrimina sobre la base de raza, color, nacionalidad, edad, discapacidad o sexo. Este aviso tiene información importantesobre su solicitud o cobertura. Busque las fechas importantes en este aviso. Es posible que tenga que tomar alguna acción en undeterminado plazo para mantener su cobertura de salud o ayuda con los costos. Usted tiene derecho a obtener esta informacióny otra información sobre su solicitud o cobertura, en su propio idioma y sin costo. Llame al 855-857-9944. (TTY: 711)Chinese Traditional: 本通知含有重要資訊。Regence ��您申請或承保的相關資訊。請撥打 855-857-9944 索取。(聽障專線:711)Vietnamese: Thông báo này có Thông tin Quan trọng. Regence tuân thủ luật pháp Liên bang về quyền công dân hiện hành vàkhông phân biệt đối xử theo chủng tộc, màu da, nguồn gốc quốc gia, độ tuổi, khuyết tật hoặc giới tính. Thông báo này có thôngtin quan trọng về đơn đăng ký hoặc bảo hiểm của quý vị. Tìm những ngày chính trong thông báo này. Quý vị có thể cần hànhđộng trước một số thời hạn để duy trì bảo hiểm sức khỏe của mình hoặc được giúp đỡ có tính phí. Quý vị có quyền lấy thông tinnày và thông tin khác về đơn đăng ký hoặc bảo hiểm, bằng ngôn ngữ của mình miễn phí. Gọi số 855-857-9944. (TTY: 711)Korean: 이 공지 사항에는 중요 정보가 들어 있습니다. Regence은 해당 연방 민권법을 준수하며 인종, 피부색, 출신 국가, 연령,장애, 또는 성별에 따라 차별하지 않습니다. 이 공지 사항에는 해당 신청서 또는 적용 범위에 관한 중요한 정보가 있습니다. 이 공지사항의 주요 날짜를 찾아 보십시오. 해당 건강 보험을 그대로 유지하거나 비용을 지원 받으려면 특정 기한까지 조치를 취하셔야합니다. 귀하는 모국어로 작성된 본 정보나 해당 신청서 또는 보장 범위에 대한 기타 정보를 무료로 받을 수 있는 권리가 있습니다.855-857-9944로 연락하십시오. (TTY: 711)01012017.01LF12SNoticeNDMARegence
Russian: В данном Уведомлении содержится важная информация. Regence несет обязательства по соблюдениюприменимых норм федерального законодательства о гражданских правах и не допускает дискриминации по признакурасы, цвета кожи, национального происхождения, возраста, статуса инвалидности или пола. В данном уведомлениисодержится важная информация о вашем заявлении или страховом покрытии. Обратите внимание на ключевые даты,указанные в данном уведомлении. Возможно, вам нужно предпринять некоторые действия к определенному сроку, чтобсохранить страховое покрытие или получить помощь с расходами. Вы имеете право получить данную, а также прочуюинформацию о вашем заявлении или страховом покрытии на родном языке бесплатно. Позвоните по номеру 855-8579944. (TTY: 711)Tagalog: Ang Abiso na ito ay may Mahalagang Impormasyon. Ang Regence ay sumusunod sa mga naaangkop na Pederalna batas sa mga karapatang sibil at hindi nagdidiskrimina batay sa lahi, kulay, bansang pinagmulan, edad, kapansanan, okasarian. Ang abiso na ito ay may mahalagang impormasyon tungkol sa iyong aplikasyon o coverage. Hanapin ang mgaimportanteng petsa sa abiso na ito. Maaaring kailangan mong gumawa ng hakbang hanggang sa mga partikular na takdang arawupang mapanatili mo ang iyong coverage sa kalusugan o tulong sa mga gastusin. May karapatan kang makuha angimpormasyong ito, at iba pang impormasyon tungkol sa iyong aplikasyon o coverage, sa iyong sariling wika nang walang bayad.Tumawag sa 855-857-9944. (TTY: 711)Ukrainian: Це повідомлення містить важливу інформацію. Regence дотримується застосовного федеральногозаконодавства про громадянські права та не проводить політику дискримінації за расовою приналежністю, кольоромшкіри, походженням, віком, інвалідністю та статевою ознакою. Це повідомлення містить важливу інформацію пропов’язану з вами програму або страхове покриття. Зверніть увагу на ключові дати в цьому повідомленні. Щоб зберегти засобою план медичного страхування або право отримувати грошову допомогу, можливо, вам потрібно буде вжитивідповідні заходи, для яких установлено певні часові обмеження. Ви маєте право на безкоштовне отримання рідноюмовою як цієї інформації, так і будь-якої іншої, пов’язаної з програмою чи страховим покриттям. Телефонуйте за такимномером: 855-857-9944 (телетайп: 711).Mon-Khmer, Cambodian: សេចក្ត �័ត៌មានេំខាន់ ។ Regence នមានការលរ ើសលអើងច្បំល ោះពូ ជសាសន៍ ពណ៌សមបុ រ សញ្ជាតិលដ្ើម អាយុ ពិការភាព ឬលេទ្ល យើ ។លសច្បក្ត ��ំពី ក្យសុំ �ខភាពរបស់អនក្ ។សូ មរក្លមើលកាលបរ ិលច្បេ �្បក្ត ី ជូ នដ្ំណឹងលនោះ ។ អន ក្អាច្បត្តូវចាត់ វ �មកាលបរ ិលច្បេ �្ាបាននូ �ខភាព ឬបានទ្ទ្ួ លការជួ �្លៃ ថលទ ំសុខភាពរបស់អនក្ ។អន ក្មានសិទ្ធិទ្ទ្ួ លបានព័ត៌មានលនោះ និងព័ត៌មានដ្ថ្ទ្ អំពី ក្យសុំ �ខភាពរបស់អនក្ ជាភាសាថដ្លអន �ប់បង់ត្បាក្់ល ើយ ។ លៅមក្លលខ 855-857-9944 ។ (អន ក្ពិបាក្សាតប់ �ត្បើ TTY សូ មលៅមក្លលខ ៖ 711)01012017.01LF12SNoticeNDMARegence
Japanese: �まれています。Regence �話ください: 855-857-9944。(TTY: 711)Amharic: ይህ ማሳሰቢያ ጠቃሚ መረጃ ይዟል፡፡ Regence በሚተገበረው የፌደራል ሲቪል መብቶች ህግጋት በዘር፣ በቀለም፣ በመጡበት ብሄር፣ እድሜ፣ የአካል ጉዳት ወይምፆታ መድሎ አይደረግም፡፡ ማሳሰቢያው ስለ ማመልከቻዎትና ሽፋን ጠቃሚ መረጃ አለው፡፡ በዚህ ማሳሳቢያ ላይ ቁልፍ ቀናትን ይፈልጉ፡፡ በተወሰኑ የመጨረሻ ቀናት የጤና ሽፋኑ ላይወይም የወጪን ድጋፍ እንዲቀጥል እረምጃ መውሰድ ያስፈልጋል፡፡ ይህንን መረጃ እንዲሁም በማመልከቻዎት ወይም ሽፋኑ ላይ ሌሎችንም መረጃዎች በራስዎን ቋንቋ ያለምንም ክፍያየማግኘት መብት አሎት፡፡ 855-857-9944 ይደውሉ፡፡ (ቲቲዋይ፡- 711)Cushite/Oromo: Beeksisni kun odeeffannoo barbaachisaa qabatee jira. Regence Ulaagaa seera mirga Siivilii Federaalaa kanguutuu fi sanyii, bifa, lammummaa, umrii, miidhama qaamaa ykn saala irratti hundaa’ee addaan hinqoodne dha. Beeksisni kuniyyannoo ykn haguuggii kara keessan irratti odeeffannoo barbaachisaa qabatee jira. Guyyoota furtuu beeksisa kana keessa jiranilaalaa. Haguuggii fayyaa ykn gargaarsa keessan eeggachuuf hanga dhuma yeroo ta’eetti tarkanfii ta’e gatii bastanii fudhachuuqabdu. Odeeffannoo kana fi waa’ee iyyannoo ykn haguuggii keessanii kaffaltii tokko malee afaan keessaniin argachuuf mirgaqabdu. Bilbilaa 855-857-9944. (TTY: 711)Arabic: إلى قوانين الحقوق المدنية الفيدرالية المعمول بها وال تمارس التمييز على أساس العرق أو اللون أو األصل القومي أو السن Regence تمتثل . يحتوي هذا اإلخطار على معلومات مهمة فقد تحتاج إلى اتخاذ إجراء ما قبل . ابحث عن التواريخ الرئيسية في هذا اإلخطار . يحتوي هذا اإلخطار على معلومات مهمة عن الطلب أو التغطية الخاصة بك . أو اإلعاقة أو الجنس لديك الحق في الحصول على هذه المعلومات والمعلومات األخرى المتعلقة بالطلب . بعض المواعيد النهائية للحفاظ على التغطية الصحية الخاصة بك أو تلقي مساعدة بخصوص التكاليف )711 : (الكتابة عن بُعد للصم .855-857-9944 اتصل بالرقم . أو التغطية الخاصة بك بلغتك مجا ًنا Punjabi: ਇਸ ਨੋਟਿਸ ਟ ਿੱ ਚ ਮਹਿੱ ਤ ਪੂਰਨ ਜਾਣਕਾਰੀ ਹੈ। Regence ਲਾਗੂ ਫੈਡਰਲ ਨਾਗਰਰਕ ਅਰਿਕਾਰਾਂ ਦੇ ਕਨੂੂੰਨ ਦੇ ਅਨੁਰੂਪ ਹੈ ਅਤੇ ਜਾਰਤ, ਰੂੰ ਗ, ਰਾਸ਼ਟਰੀ ਮੂਲ,ਉਮਰ, ਅਪਾਰਹਜਤਾ, ਜਾਂ ਰਲੂੰਗ ਦੇ ਅਿਾਰ ‘ਤੇ ਭੇਦਭਾਵ ਨਹੀਂ ਕਰਦਾ। ਇਸ ਨੋਰਟਸ ਰਵਿੱ ਚ ਤੁਹਾਡੇ ਬੇਨਤੀ-ਪਿੱ ਤਰ ਅਤੇ ਸੁਰਿੱਰਿਆ ਬਾਰੇ ਮਹਿੱ ਤਵਪੂਰਨ ਜਾਣਕਾਰੀ ਹੈ। ਇਸ ਨੋਰਟਸਰਵਿੱ ਚ ਮੁਿੱ ਿ ਰਮਤੀਆਂ ਵੇਿੋ। ਤੁਹਾਨੂੂੰ ਤੁਹਾਡੀ ਰਸਹਤ ਸੁਰਿੱਰਿਆ ਰਿੱ ਿਣ ਜਾਂ ਲਾਗਤਾਂ ਨਾਲ ਮਦਦ ਕਰਨ ਲਈ ਰਨਯਤ ਰਮਆਦ ਸੀਮਾਵਾਂ ਦੁਆਰਾ ਕਾਰਵਾਈ ਕਰਨ ਦੀ ਲੋ ੜ ਹੋ ਸਕਦੀਹੈ। ਤੁਹਾਨੂੂੰ ਇਹ ਜਾਣਕਾਰੀ, ਅਤੇ ਆਪਣੇ ਬੇਨਤੀ ਪਿੱ ਤਰ ਜਾਂ ਸੁਰਿੱਰਿਆ ਬਾਰੇ ਹੋਰ ਜਾਣਕਾਰੀ ਆਪਣੀ ਭਾਸ਼ਾ ਰਵਿੱ ਚ ਰਬਨਾ ਰਕਸੇ ਲਾਗਤ ਤੋਂ ਪਰਾਪਤ ਕਰਨ ਦਾ ਅਰਿਕਾਰ ਹੈ। 855857-9944 ‘ਤੇ ਕਾਲ ਕਰੋ। (TTY: 711)01012017.01LF12SNoticeNDMARegence
German: Diese Mitteilung enthält wichtige Informationen. Regence hält die Grundrechte der USA ein und es finden keineDiskriminierungen aufgrund von Rasse, Hautfarbe, nationaler Herkunft, Alter, Behinderung oder Geschlecht statt. Diese Mitteilungenthält wichtige Informationen über Ihren Antrag oder die entsprechende Versicherungsdeckung. Beachten Sie wichtige Fristen indieser Mitteilung. Sie müssen unter Umständen Maßnahmen innerhalb bestimmter Fristen ergreifen, um IhrenKrankenversicherungsschutz zu erhalten oder eine Kostenerstattung zu erhalten. Sie haben das Recht, diese Informationen undandere Informationen über Ihren Antrag oder Ihren Versicherungsschutz kostenlos in Ihrer Sprache zu erhalten. Rufen Siefolgende Nummer an 855-857-9944. (Fernschreiber: 711)ີ່ ສາຄັນ. Regence ສອດຄ້ ມຂ້ ມLaotian: ແຈູ ນທ້ ງການສະບັບນີ່ ອງກັບກີ່ າດ້ ວຍ ິ ສດທີ່ ຽວຂ້ ອງິ ພື ອງຂອງຣັຖບານກາງ ີ່ ທກົ ດໝາຍ ວົ ນລະເມ້້ີ່ແລະ ບມການຈາແນກ ເຊຸ , ຄວາມເປັ ນຄິ ວ, ຊາດກາເນດ, ອາຍ້ ງການສະບັບນື ອຊາດ, ສຜິ ການ ຫື ເພດ. ແຈົ ນພີ່ີ່້ .້ ມມຂູ ນທສາຄັນກຸ ້ ມຄອງ. �ແຈີ່ ຽວກັບການນາໃຊ້ ຂອງທີ່ ານ ຫ້ ງການສະບັບນື ການຄີ່ ງ ເພີ່ື ອ ໃຫີ່ ໄດທຸ ້ ມຄອງສຸ ຂະພາບຂອງທີ່ ານອາດຈະຕ້ �ບເຂດເວລາໃດໜ້ ື ສບຕ້ ຮັບການຄີ່ ານ ຫືີ່້້ ມ້ ມການຊູ ນນ ແລະ ຂູ ນອຸ ້ ມຄອງຂອງທີ່ ວຍເຫ້ ານງີ່ ານມິ ສດເອີ່ ຽວກັບການສະໝັກ ຫີ່ ານື ອທາງດື ນກື ການຄົ ບປະມານ. ທົ າຂີ່ ທເປີ່ ເສຍຄີ່ 855-857-9944. (TTY: 711)ັ ນພາສາຂອງທີ່ ານໂດຍບີ່ າໃຊ້ ຈີ່ າຍ. ຕິ ດຕ01012017.01LF12SNoticeNDMARegence
Regence BlueShield: Silver Connect 4000 (73) Providence-Swedish Health Coverage Period: 01/01/2017 - 12/31/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Eligible Family Plan Type: PPO