Transcription
ACGME INTERNATIONAL(ACGME-I)Clinical CompetencyCommitteesA Guidebook for ProgramsKathryn Andolsek, MD, MPHDuke UniversityJamie Padmore, MScMedstar- GeorgetownKaren E. Hauer, MDUniversity of California – San FranciscoEric Holmboe, MD, MACP, FRCPAccreditation Council for Graduate Medical EducationThe information in the Guidebook is current as of January 2015 andmodified for ACGME-I accredited programs September 2016 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookExecutive SummaryThe Clinical Competency Committee (CCC) is a structure that has emerged asan essential component of the evaluation process in graduate medical education.Because the CCC is a required component of International FoundationalAccreditation for advanced specialty programs, committees are facing questionsregarding structure, function, and process.The purpose of this manual is to provide designated institutional officials (DIOs),program directors, faculty members, CCC members, coordinators, and residentsand fellows with information and practical advice regarding the structure,implementation, function, and utility of a well-functioning CCC. The materialswere prepared for both individual learning and application in a group setting. It isour intent that programs will be able to utilize these materials to have meaningfulfaculty conversations and development on CCC functions and outcomes, andgreater transparency with residents and fellows on the nature of assessment incompetency-based education.This manual provides information related to the following topics:1. CCC purpose2. Structure and membership3. Meeting preparation4. Running the meeting5. Post-meeting documentation and follow-up6. Legal issues and considerations7. Annotated bibliography8. Q&AThere are several appendices included that contain tools for programs and CCCsto utilize. We have also provided a robust reference list to support the variousaspects of CCCs, including assessment, feedback, documentation, groupdynamics, and outcomes.We look forward to your feedback, and hope this manual provides you and yourfaculty with valuable information and tools to enhance your GME program.[1] 2015 Accreditation Council for Graduate Medical Education (ACGME)
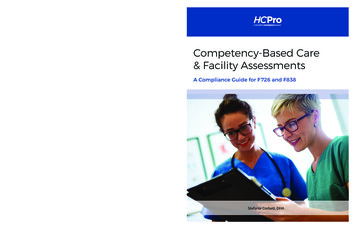
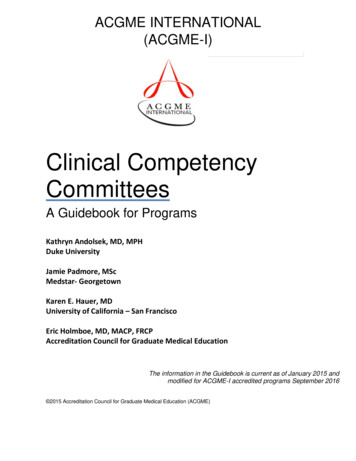
ACGME-I CCCGuidebookIntroductionA Clinical Competency Committee (CCC) is defined by the ACGMEInternational (ACGME-I) as a: required body comprising three or more membersof the active teaching faculty that is advisory to the program director and reviewsthe progress of all residents/fellows in the program.1It is recognized that the CCC represents a new structure and process toprograms. The objectives of these materials are to help programs:1. Recognize the role and purpose of the CCC for individual programs2. Design, create, and implement a CCC3. Run an effective CCC meeting4. Provide feedback to residents or fellows5. Anticipate process questions and academic law considerations6. Analyze evidence supporting CCCs to make the best choices for their ownCCC processThis guidebook is intended to be a practical and useful resource and professionaldevelopment tool to help institutional and program leadership, coordinator(s),faculty members, and residents/fellows understand all aspects of CCCs. Weencourage you to share these materials with your residency or fellowshipprogram faculty and leadership, and use the exercises as part of faculty andcoordinator professional development. These materials can be completedindividually or in a group meeting. The guidebook also provides somesuggestions for faculty development.The CCC is an essential component, but still only one part, of a high performingresidency or fellowship program. It contributes to an effective resident/fellowassessment “system” as outlined in Figure 1. In this figure, the CCC serves theimportant function to synthesize the multiple quantitative and qualitativeassessments. This figure highlights several important points:1. The CCC process will depend on the quality of the assessment program thatincludes a combination of assessment methods.22. Residents and fellows must be active agents in this system; guided selfdirected assessment behaviors by the resident or fellow should be stronglyencouraged.3. The program director within a residency or fellowship program is the ultimatearbiter of whether a resident or fellow will enter unsupervised practice. Theprogram will perform the majority of the assessments that will inform the finalentrustment decision to graduate a resident or fellow from the program. Thisaccountability cannot be over-emphasized: professional self-regulationdepends heavily on the judgment of training programs, as manifest by thefinal evaluation and entrustment made by the program director.[2] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookFigure 1 Structure of a High Performing Resident/Fellow Assessment SystemResidents both residents and fellowsFB Feedback loopsD Assessment data and informationThe model is more fully described in Appendix A[3] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookPart 1: Purpose of the CCCPurpose of the Clinical Competency Committee (CCC) for theProgram and AccreditationThe CCC serves several purposes—for the program director, the program itself,the faculty, the residents/fellows, the ACGME-I, and the specialty. See Table 1.The ultimate purpose is to demonstrate our accountability as medical educatorsto the public, that our graduates will provide high quality, safe care to our patientsand maintain the standards of the health care system.Table 1. Purposes of a CCCProgramDirectorFulfill Public Accountability by ensuring: Residents/fellows who successfully complete program can practice the specialtyspecific core professional activities without supervision Create greater “buy-in” from a group of faculty members to make decisionsregarding performance Enhance credibility of judgments about resident/fellow performanceFacilitate role of “advocate” for the resident/fellowProgram1) Develop shared mental model of what resident/fellow performance should “looklike” and how it should be measured and assessed2) Ensure assessment tools sufficient to effectively determine performance acrossthe competencies3) Increase quality, standardize expectations, and reduce variability in performanceassessment4) Contribute to aggregate data that will allow programs to learn from eachother by comparing residents’ and fellows’ judgments against comparabledata5) Improve individual residents/fellows along developmental trajectory6) Serve as system for early identification of residents/fellows who are challenged7) Improve program8) Model “real time” faculty development1) Facilitate more effective assessment that may be easier for evaluatorsHelp faculty develop a shared mental model of the competencies2) May result in simplified “more actionable” assessment tools to help facultydocument more effectively and efficiently what they observe trainees doing inclinical settingsFacultyResident/Fellow 1) Improve quality and amount of feedback; normalize constructive feedbackOffer insight and perspectives of a group of faculty members2) Compare performance against established competency benchmarks (ratherthan only against peers in the same program)3) Allow earlier identification of sub-optimal performance that can improve remedialintervention4) Improve stretch goals for residents/fellows to achieve higher levels ofperformance5) Provide transparency around performance expectations[4] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookACGME-I1) Enhance progress toward competency-based education with outcomesdata2) Establish international benchmarks for trajectory of resident/fellow skillacquisition3) Enhance identification of programs that need to improve (programs whoseresidents/fellows aren’t making progress as compared to national peergroup)4) Provide better measures for public accountability5) Provide feedback loop as to whether -- and when -- programs are able tomeet expectations of the International Review Committee (RC-I) thusenabling reasonable expectations6) Enable continuous quality improvement of residency/fellowship programs7) Document the effectiveness of a nation’s GME efforts in provision ofgraduates prepared to meet the needs of the public.The concept of a CCC is an international phenomenon. The United Kingdominstituted an Annual Review of Competence Progression in 2007. The Canadiansystem also uses Residency Program Committees (RPC) and is exploring howto use a group process as part of its new Milestones-based GME system. CCCsare not new in the US; some programs, such as in internal medicine, used themin the 1980s, in concept, if not in name. The specialty of anesthesiology hasimplemented them within its residencies for many years and required, incollaboration with the American Board of Anesthesiology, that these programsparticipate in the submission of an evaluation of clinical competency of eachresident twice yearly.A program’s creation of a CCC is, in itself, a “developmental” process. We willstart with a brief review of current ACGME-I requirements for a CCC.Programs may identify gaps and potential enhancements by comparing whatthey have in place to the requirements. For newly accredited programs justbeginning to institute a CCC, the next few pages offer a practical roadmap.[5] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookPart 2: CCC Structure and MembershipDesigning and Creating a CCCTo design and create a CCC, it is useful to start with “the requirements.” TheACGME-I’s expectations for a CCC are in the International Foundational ProgramRequirements, which stipulate the minimum requirements for a CCC in everyresidency and fellowship program (see Requirement V.A.). Once the CCC fulfillsthe International Foundational Program Requirements, programs are free toinnovate!The ACGME-I has provided additional guidance for CCCs in Frequently AskedQuestions (FAQs) for International Foundational Requirements.While there are no specific requirements for the CCC found in the InstitutionalRequirements (IR), there is at least one institutional requirement that may beuseful to consider. The sponsoring institution is responsible for programs’developing “conditions for reappointment, non-renewal of appointment, or nonpromotion,” and requires that the resident agreement/contract must contain orprovide a reference to conditions for reappointment, non-renewal of appointment,or non-promotion (International Institutional Requirement II.D.4.d.).CCCs may be an excellent mechanism to identify those criteria in part or, at thevery least, with which to align Milestone performance. Consider how Milestonesand your program’s specialty-specific educational objectives fit into yourprogram’s criteria for promotion and/or renewal of a resident’s/fellow’sappointment. Remember, these are intended to be used as a formativeframework to guide curriculum, assessment, and CCC deliberations in programs;however, Milestones are also one guide to inform CCC deliberations that lead to asummative judgment for a resident’s/fellow’s promotion and graduation. However,Milestones should not be used as the sole criteria for these important decisions.Questions to ask of your program include: Are any clarifications or adjustments in your criteria for promotion and/ornon-renewal required? Are any changes in your agreement of appointment necessary to reflectMilestone reporting to the ACGME-I? Are any changes in your grievance policy necessary?You may find you do not need to make any changes at all, but the developmentof a CCC provides an excellent opportunity to review your current performancestandards, promotion criteria, and assessment processes, and align theMilestones and the CCC with them. Your designated institutional official (DIO),Office of GME, Legal Department, and Human Resources may provide usefulguidance.[6] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookHow well do you know the CCC Requirements?Appendix B is a multiple choice “quiz” on the current ACGME-I requirements for aCCC. Consider having your CCC members and key faculty leaders take this quizas a fun faculty development exercise!The ACGME-I’s CCC requirements are fairly minimal (See Table 2). There areonly five requirements.Table 2. International Foundational Requirements for a CCCThe program director must appoint CCCFoundationalRequirementV.A.Composed of members of the residency facultyV.A.1.a)Must have written description of responsibilities including itsresponsibilities to the sponsoring institutions and to theprogram directorV.A.1.b)Should review all resident/fellow evaluations by allevaluatorsShould make recommendations to the programdirector regarding resident/fellow progress,including promotion, remediation, dismissalV.A.1.c).(1)V.a.1.c).(2)Appendix C contains a template that may help you design your CCC by “walkingyou through” its various components. By filling in the blanks provided, you cangenerate a draft document that will help you fulfill the requirement for a “writtendescription of the responsibilities” of the CCC. Some program directors maydevelop the written description of the CCC on their own. Others will ask the CCC tocreate it as one of its initial activities as a group, or appoint a subset of the faculty.The template provides a checklist of items to consider.Creating, developing, and improving a CCC does require time and effort. Sharingbest practices across programs and institutions, having strong institutional supportfrom the DIO for shared resources across programs within an institution, andappreciating that there will be a ‘learning curve’ for new programs can facilitate thelong-term effectiveness of a CCC. Ultimately, the CCC process will helpresidencies/fellowships do what they have always been responsible for doing, butnow with more structure and clearer purpose.Creating and implementing a CCC provides the program with excellent opportunitiesto enhance two other ACGME-I requirements: 1) Annual Program Evaluation andImprovement; and, 2) Faculty Development.[7] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookFaculty development will be needed at three levels: 1) the program director; 2) theengaged faculty members who join the CCC or Program Evaluation Committee(PEC); and, 3) the faculty members in the trenches who are not fully involved ineducational programming or administration, but who are actively teaching andassessing. Each group will have different needs. Program directors and CCCmembers will need a deeper understanding of the Milestones, assessment, groupprocess, and program evaluation; faculty members in the trenches need tounderstand what key elements of assessment information they need to contributeto the larger “whole” for consideration by the program director and CCC.3,4,5 Thesefaculty members must be trained to use assessment methods and tools alignedwith the purpose of the curricular experience they are supervising or overseeing.Your PEC, which undertakes the annual program evaluation resulting in one ormore improvements, may select implementing and/or improving the CCC as oneof its enhancements for the academic year. If the PEC chooses this goal, becertain the CCC improvement plan is reflected in the PEC’s analysis and actionplan(s).The ACGME-I also expects program engagement in faculty development. Facultydevelopment is one of the required program components reviewed by the PEC inthe Annual Program Evaluation and Improvement process (InternationalFoundational Program Requirement V.D.). The CCC faculty role will typicallyinclude the need for much faculty development. The ACGME-I recognizes thatalthough evaluation is a core faculty competency, most faculty will need additionaltraining in the evaluation process. This training can include evaluation processtraining (how to interpret aggregated evaluation data), understanding how manyassessments are needed for each Milestone, assurance of data quality, andapplication of Quality Improvement methods to the evaluation processes.5 TheCCC provides an opportunity for faculty development for other program facultymembers, as well: to understand the CCC process and how its evaluations ofresidents/fellows fit into the overall assessment of resident/fellow performanceusing the Milestones and other specialty-specific curricular goals and objectives.General Principles:The size of the residency or fellowship will affect constructing and running a CCCmeeting. For the purposes of this Guidebook, “small programs” are considered tobe those with fewer than 15 total learners; “medium programs” are considered to bethose with 15-to-75 learners; “large programs” have more than 75 learners.[8] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookOne committee or more: Large programs: may need to have several CCCs (“sub-CCCs”); somemay become experts in one “year” of the program (i.e., oversee all PGY1s,), while others might focus on a program activity (i.e., responsible forthe research component or the quality improvement component) If “sub-CCCs” are used, it is essential that they still have robustmembership and review processes to ensure all residents/fellows arethoroughly reviewed, discussed, and provided with an opportunity toreceive high quality feedback. There also needs to be a mechanism tointegrate information from sub-CCCs, and ensure each sub-CCC is usingthe same standards and procedures. Medium or small programs: one CCC can likely oversee allresidents/fellows, but again, it will depend on the curricular design of theprogram and local resources.Committee membership: The program director must appoint the CCC, which at a minimum hasprogram physician faculty members as its members. In general, threemembers is considered the smallest number essential for a gooddiscussion. The program director should select faculty members whoteach and observe residents/fellows, but also consider how nonphysician faculty members can provide valuable input. The program director may appoint additional members who must bephysician faculty members for the same or other programs, or other“health professionals who have extensive experience with the program’sresidents in patient care and other health care settings (e.g., nurses,physician assistants, nurse practitioners, social workers, etc.).” Role of advisors/mentors: Program directors may want to considerwhether there is an inherent conflict of interest in a faculty member beingan advocate for a resident/fellow (as his/her advisor mentor) and“judging” performance (as a CCC member). On the other hand, advisorsand mentors may benefit from being observers to the CCC and hearingor contributing information to the discussion. They may also be able toconvey the impressions of the CCC to their residents/fellows. “Right size” – large enough to reflect diversity of perspectives; smallenough to be “manageable” in terms of faculty development about CCCrole, and participation in meeting discussions “Right people” – CCC members must be committed and able to attend allor nearly all meetings; erratic attendance will not allow the continuitycritical to assess resident/fellow performance over time. Each membermust be willing to make honest decisions, even when it’s tough. Term limits: Consider whether appointments should be “in perpetuity,” orfor a defined term limit. “In perpetuity” appointments should be coupledwith regular addition of new members for fresh perspectives; if enactingterm limits, consider staggering appointments so that not everyone turnsover at once.[9] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebook Residents cannot serve on the CCC. Having residents responsible for thehigh-stakes decisions regarding their colleagues is not allowed. On theother hand, residents have a major role in providing input into thecompetencies of their peers through the multi-source/multi-raterassessment process (previously also called “360-degree feedback”). Non-physician program staff members, such as program coordinators,cannot serve on the CCC, but can attend to provide support to the CCC. Special considerations:o Small programs may have a challenging time identifying individualsfor the CCC as many of these programs also have a limited numberof faculty members. Many fellowships will find themselves in thisposition. In addition to program faculty members, consider invitingfaculty members from other disciplines or settings for which thelearner provides substantial consultation. Many small programs arealso tied to specific clinical settings; consider inviting non-physicianfaculty members from these settings who have ongoing contactwith the learner to sit on the CCC (e.g., a nurse leader from adialysis unit for a nephrology fellowship program, a nurseanesthetist for a surgery fellowship, or a discharge planner from aspecific clinical unit).o Medium programs may also encounter some of the same problemsas small programs, and may still need to use a sub-committeeprocess to facilitate CCC deliberations. Role/responsibility of each CCC member: French et. al. presentGuidelines for Committee Members:6o Know role on the committeeo Follow-through with assigned taskso Be educated on purpose and responsibilities of the committee,Milestones and the specialty’s specific educational objectives, thereview process, and committee guidelineso Do “one’s part” to maintain a collegial atmosphere within thecommitteeo Ensure own “voice” is heardAppendix D lists additional details. These include the essential requirement forconfidentiality. Larger CCCs may assign members a subset of theresidents/fellows to review in advance of a meeting. It will be important to identifywho will convey the CCC results to the program director (if not in attendance)and to the resident/fellow.[10] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookCommittee chair:The International Foundational Program Requirements are silent on the issue ofwho should serve as chair of the CCC. Think through who would be the rightchair for your program: the program director? the associate program director?another faculty member? a rotating responsibility among members? Select theindividual who will best solicit broad input regarding resident/fellow performanceand ensure all voices are heard. French et. al. present Guidelines for CommitteeChairs:6 Be the expert for the committee on the Milestones and the specialty’sspecific educational goals and objectives Encourage a positive working environment and open communication fromall members Ensure members know their roles, as well as the Milestones andspecialty’s educational goals and the review process/guidelines Keep meetings on task and move towards the common goal Make certain the coordinator or designated member maintainsdocumentation and meeting minutesIn addition, the CCC chair should be familiar and comfortable with effective groupprocess (see Part 4, Running the CCC Meeting, below) and major assessmentmethods.Program director role:There is no mandatory role for the program director, and he or she can be chair,member, or observer, or not attend at all.7 If present, he or she should not“detract” from the participation of other team members by prematurely insertinghis or her perspective on a given resident’s/fellow’s performance. In the sameway, the program director shouldn’t determine the performance of eachresident/fellow and then bring these to the CCC for ratification. The CCC shouldbe able to perform its assessment of resident/fellow competency, judged againstthe Milestones and the specialty’s specific educational goals and objectives, toconvey to the program director. If the program director is present at CCCmeetings, he or she should make sure other CCC members’ voices areencouraged (e.g., asking other members to discuss residents/fellows and reachconsensus decisions before adding his or her own comments). Some programdirectors find it very useful to have another faculty chair the CCC; so they canfunction better as the resident advocate and mentor and avoid the residentviewing the CCC judgments as “only” those of the program director. On the otherhand, the program director indeed has the final responsibility for reporting anddetermining the Milestone developmental level for each resident/fellow. Theprogram director should also ensure the residents/fellows are aware of theMilestones which have been reported to the ACGME-I. The program director hasthe final responsibility for determining Milestone acquisition, and reporting to theACGME-I.Coordinator Role:The coordinator is not a CCC member, and will not be “judging” residentperformance. Nonetheless, a coordinator can have a major role before, during,[11] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCand following a CCC meeting. Before the meeting, the coordinator can helpGuidebookprepare and organize the data for the CCC. During the meeting, he/she may takeminutes and capture key aspects of the discussion. Following the meeting,he/she can be part of communicating the results to the program director (if not inattendance), scheduling meetings with residents/fellows and the program directoror the designated faculty member to review the decisions, including Milestonestatus, and assisting the Program Director in submitting Milestone information oneach resident/fellow to the ACGME-I. Coordinators can also provide feedbackthrough the program’s assessment system, such as participating in multi-sourceassessment instruments.Meetings:Meeting logistics will need to be carefully considered including location,frequency and length of the CCC meetings. CCCs may wish to meet morefrequently than the minimum reporting requirement of “twice yearly,” especiallyduring the committee’s developmental phase.[12] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookPart 3: Preparing for Effective CCC MeetingsPreparing for a CCC MeetingDeveloping a Shared Mental ModelPerhaps the most important aspect of preparing for a CCC meeting is to makesure the members develop a shared mental model of what resident/fellowperformance looks like, and understand their roles and responsibilities on thecommittee, as well as how the CCC operates to judge resident/fellowperformance. This may necessitate a “meeting before the meeting,” or allocatingsufficient time at the beginning of the first CCC meeting for this discussion.Having a written description of the CCC process, and providing facultydevelopment for committee members will facilitate this process. Some programsfind it useful to discuss a relevant article at the CCC meeting as part of facultydevelopment. See the references and annotated bibliography for somesuggestions.Faculty members should reach a common understanding on the meaning of thenarratives of each Milestone in the context of their specialty. This will almostalways require group conversation. It may be worthwhile to have each facultymember perform self-assessment using the Milestones and the program’sspecialty-specific educational objectives as a faculty development exercise.Faculty members should be trained to compare each resident’s/fellow’sperformance to the Milestones and attainment of the program’s specialty-specificeducational objectives as a whole, not just to the performance of other or ‘typical’residents/fellows in the program. The committee may also benefit fromindividually assessing one or more recent program graduates using theMilestones and the program’s specialty-specific educational objectives, and thendiscussing as a CCC to determine a group consensus.Inventory Where the Milestones and the Program’s Specialty-SpecificEducational Objectives are Represented in the ProgramCCCs should inventory (or review an inventory conducted by others) where eachMilestone is currently taught and assessed in the program. Teaching may occuron a specific rotation, or in the context of a program activity, such as leadingMorbidity & Mortality rounds.The inventory should help to identify gaps in both curriculum and assessment:1. Milestones or specialty-specific educational objectives for which theprogram has no good learning opportunities or assessment tools inplace at the present time; and,2. rotations/activities the program believes add value, but for which thereis no Milestone or educational objective.The CCC can identify how to best address these gaps, perhaps by delegatingthe review to a designated faculty member.[13] 2015 Accreditation Council for Graduate Medical Education (ACGME)
ACGME-I CCCGuidebookThe assessment information and data that inform CCC deliberations shouldfollow several key principles: The assessment program will need to include multiple forms of assessmentand utilize multiple assessors. No single assessment method or tool issufficient to judge something as varied and complex as clinical competence. The combination of assessments will depend to some extent on the specificneeds of the specialty and the local context. Core methods of assessments should include direct observation of a specificcomponent (e.g., care of individual patients, procedures, etc.), multi-sourcefeedback, multiple choice test/in-service examination, longitudinal evaluations(e.g., rotational evaluation forms), audit of clinical performance, andsimulation. The specific assessment tools used will depend on the specialtyand local context. The key point to remember is that the true assessment“instrument” is not the tool or form itself, but rather the individual using it. Thetool or form simply guides the individual performing the assessment. Faculty members and others involved in a
Accreditation Council for Graduate Medical Education The information in the Guidebook is current as of January 2015 and modified for ACGME-I accredited programs September 2016 . For newly accredited programs just beginning to institute a CCC, the next few pages offer a practical roadmap.