Transcription
2.5ANCC CONTACT HOURSSounding theOBSTRUCTIVE SLEEP APNEA (OSA) is asignificant problem in the United States andworldwide. The prevalence in men is estimatedto be between 3% and 7% and the prevalencein women between 2% and 5%. Obesity isconsidered the main risk factor for OSA, andbeing overweight is also a risk factor. Somepatients with OSA aren’t obese or overweight.OSA occurs in approximately 48% of peoplewho have a body mass index (BMI) greaterthan 28 and is more common with advancingage.1 Less common in children, OSA affectsabout 3% of them.2 Because OSA is oftenunrecognized, it may be untreated and leadto medical and employment problems. Theseproblems can be costly; lead to unintendedinjuries, depression, and anxiety; and affectsocial and family relationships.1,2Take the case of Mr. J, an executive in a publishing company. In the past year, he’s increasedhis work time to 60 hours/week and decreasedhis physical activity level. He’s not exercising atall now, often eats fast food on the go,and has gained 50 pounds. He’s averaging 5 to 6 hours of restless sleepper night. He finds himself losing hispatience or falling asleep at work andyelling at his kids at home. He’s gotteninto two minor car crashes over the pastyear. At his last physical exam, his BP waselevated and he was complaining of gastroesophageal reflux disease (GERD) symptoms.His wife reports that he’s been snoring more andsounds as though he’s choking at times.Most likely, Mr. J is suffering from OSA,which is characterized by repeated periodsof apnea and hypopnea during sleep.1,2 Theseperiods of absent breathing or inadequate34 l Nursing2012 l Aprilwww.Nursing2012.comCopyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
alarmfor patients withobstructive sleep apneaBy Susan Simmons, PhD, ARNP-BC, andBill Pruitt, MBA, RRT, AE-C, CPFTbreathing lead to hypercapnia (increased partialpressure of carbon dioxide in arterial blood) andhypoxemia (decreased partial pressure of oxygen in arterial blood).2,3Because lack of oxygen isn’t compatible withlife, the brain signals a person with OSA towake up and breathe. Repeating this processmany times per night is like getting muggedon every street corner as you try to walk througha large city for 6 to 8 hours. By the end of thenight, you’re not only exhausted mentally,but your cardiovascular system is tired out aswell—in a stressed-out way, rather than in agood way as from exercise.What’s OSA?OSA is characterized by many apneic andhypopneic periods during the sleeping cycle. ForOSA, the definition of apnea is arrest of breathingfor 10 seconds or longer and hypopnea is definedas ventilating 50% or less of normal.2 OSA occurswhen the musculature of the pharynx and tonguerelax during sleep, obstructing ventilation. Manystructures contribute to airway obstruction.4 (SeeAn inside look at OSA.)The lack of ventilation decreases oxygenation, activating the fight-or-flight responseof the sympathetic nervous system, whichleads to an increase in heart rate, BP, respiratory rate, blood glucose levels, and mental activity.2 These changes aren’t conducive to wellrested sleep. Over time, the repeated episodesput a strain on the cardiovascular system, leadingto hypertension as well as daytime sleepiness,nonrestorative sleep, fatigue, and l l Nursing2012 l 35Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
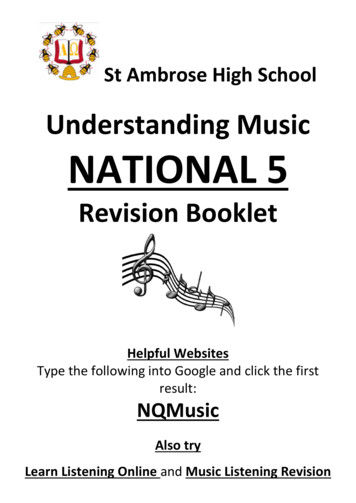
A host of signs and symptomsInitially, the only noticeable problemmay be snoring, which is often considered simply a nuisance, especiallyfor the bed partner. Up to 40% of alladults and 12% of all children reportsnoring.2Eventually, excessive daytimesleepiness and lack of concentrationoccur. Symptoms of daytime sleepiness and impaired concentration maybe so intense that they interfere withthe patient’s ability to function atwork. Falling asleep at work, showing up late, not completing work onschedule, being forgetful, and havingmood changes may diminish an employee’s productivity. Work performance may deteriorate so much thatthe patient is fired or laid off.Hypertension and choking duringsleep, signs of OSA, can increase theheart’s workload. Many signs andsymptoms, including nocturia andrestlessness and fitful sleep, also interfere with sleep, increasing daytimesleepiness and inability to concentrate. Libido changes can impair relationships at home.1,6In children, behavioral signs andsymptoms include hyperactivity, irritability, and aggression as well asdaytime sleepiness, snoring, andnocturnal enuresis. Often the signsand symptoms of OSA are confusedwith attention-deficit hyperactivitydisorder (ADHD). Children may alsoexperience difficulty in school andwith relationships.2Reaching a diagnosisObtain a comprehensive healthhistory, including a sleep history.The health history should includeAn inside look at OSAMany factors contribute to airway obstruction, including the tonsils, tonguevolume, soft-tissue airway structures, length and fullness of the soft palate,and positioning of the jaw structure, specifically the maxilla and mandible.4TongueSoft PalateUvulaEpiglottisquestions about sleep hygiene suchas these: How many hours do you normallysleep each night? Do you wake up refreshed? Do you feel sleepy during the day? Are you fatigued during the day? Do you know if you snore?Assess sleepiness severity by askingthe patient to complete the EpworthSleepiness Scale (ESS). The ESS willprovide information about the impactof excessive sleepiness on daily activities and quality of life.6,7 (The ESSwas developed by Dr. Murray Johns.Individuals, including clinicians andresearchers, can obtain it for free fromhttp://epworthsleepinessscale.com/.All other users must have a license touse it. See the website for details.)The ESS, which is self-administered,measures the chance of falling asleepin eight common scenarios. Scoringfor each situation ranges from 0, notlikely to fall asleep, to 3, highly likelyto fall asleep. ESS scores have beenfound to correlate well with sleepstudy results.Perform a thorough physical assessment. Obtain vital signs as wellas height, weight, and neck circumference. Pay special attention to theupper and lower respiratory systems. Anatomic abnormalities thatincrease the risk of OSA include nasal obstruction as a result of septaldeviation and turbinate hypertrophy.Other factors that contribute to OSAinclude abnormalities of the palate,uvula, tonsils, and tongue (includingposterior placement and thickeningof the palate, a thick or long uvula,enlarged tonsils, and large tonguevolume).6,8,9 Assess the cardiovascular system as well as the thyroidgland. (See Risk factors for OSA.)Diagnostic testingReferral to a sleep center for a sleepstudy and evaluation is an excellent36 l Nursing2012 l Aprilwww.Nursing2012.comCopyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
way to confirm OSA. Sleep centersoften use self-administered assessment tools such as the ESS. Healthcare providers will thoroughly examine the patient, looking at physicalcharacteristics such as neck and upper respiratory tract structure andfunction as well as cardiac and pulmonary function. These providersare also well-versed in medicationsand other conditions that may interfere with sleep, such as sedatives,stimulants, and alcohol; neurologicconditions, including depression andnarcolepsy; sleep movement disorders, such as restless legs syndrome;and hypothyroidism.10A sleep study involves an overnight stay unless the patient is a shiftworker and normally sleeps duringthe day; in this case, the study isdone during the daytime. The entiresleep process, including sleep movements and awakenings, is video recorded. The overnight sleep evaluation includes and records a numberof parameters including an electroencephalogram for brain wave activity,electrooculogram for eye movement,chin electromyogram to detect bruxism (teeth grinding), airflow, oxygensaturation (SpO2), respiratory effort,and heart rate or ECG to detect dysrhythmias. The leg electromyogrammay also be recorded to detect periodic limb movements that often contribute to sleep disturbances.6OSA is then measured for severity(mild, moderate, or severe) as indicated by the number of OSA episodesper hour. The number of events perhour is also called the apnea-hypopneaindex (AHI) or respiratory disturbanceindex (RDI).6 (See Determining severityof OSA.)Some portable monitoring devicesfor the home have been approved bythe FDA, but they’re not offered inall areas and insurance may not payfor them. Portable monitoring can bewww.Nursing2012.comused for screening but not for diagnosis.6,11Managing OSAThe incidence of OSA increases inpatients who are obese, smoke, drinkalcohol, and use sedatives.10 If thesefactors are present, counsel the patient and offer support to encouragethe patient to make lifestyle changesthat address these issues contributingto OSA.The definitive treatment for OSAis positive airway pressure (PAP) delivered as continuous positive airwaypressure (CPAP), bilevel positive airway pressure (BPAP), or auto positiveairway pressure (APAP) modes during sleep. PAP keeps the structuresof the pharynx and tongue from collapsing during sleep, thus inhibitingor eliminating the airway obstruction. CPAP and BPAP are appliedthrough an oral, nasal, or oronasalinterface. These devices are securedby soft headgear and adjustablestraps. Using PAP improves sleep,decreases daytime sleepiness, improves concentration, and reducesBP. Effective treatment also reducesthe number of motor vehicle crashesinvolving patients with OSA.12Medicare guidelines have approvedthe use of CPAP in patients withmoderate or severe OSA; that is,in those with 15 or more apnea/hypopnea episodes per hour. Theuse of CPAP is also approved for patients with fewer than 15 documentedepisodes per hour if they also haveexcessive daytime sleepiness (noted byan ESS score of 10 to 12), hypertension, and/or cardiovascular disease.6Trained technicians in the sleeplab can achieve the optimal amountof pressure for the patient with aPAP device. They monitor the patient as he or she sleeps, adjustingthe mask and pressure to achieveoptimal results, keeping apnea/Risk factors for OSA1,3,6 History of snoring History of excessive daytimesleepiness Complaints of fatigue, nonrestorativesleep Large neck circumference (women, 16 inches [41 cm]; men, 17 inches[43 cm])1,4 BMI 306 Male gender Increased age Craniofacial abnormalities Smoker or previous smoker Alcohol use History of cardiovascular diseaseincluding:6- hypertension- coronary artery disease- heart failure- dysrhythmias History of cerebrovascular disordersincluding:6- transient ischemic attacks- stroke- dementia History of depression Erectile dysfunction Hypothyroidism16 Postmenopausehypopnea episodes in the mildrange, preferably less than 10 episodes per hour.CPAP requirements can changeover time and aren’t “one pressure fitsall.” Patients who are more obese andhave shorter, fatter necks tend totolerate higher pressures than thinnerpatients and those with longer, thinner necks. Often after the first month,pressure is decreased by around1.5 cm H2O. As airway edema decreases with treatment, less pressureis thought to be needed. PAP mayneed to be adjusted through themonths and years as patients changeweight, medications, and other variables. Sleep studies are repeated ifsnoring, daytime sleepiness, or othersigns or symptoms return.6April l Nursing2012 l 37Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
APAP can be used to titrate pressure and meet the patient’s changingneeds. As the patient changes position, sleep stages, or has differentneeds on different nights, the deviceself-adjusts accordingly, which mayimprove adherence to therapy.6Normally, OSA is diagnosed via afull-night sleep study and PAP optimal treatment is established on a second full night. Due to concerns suchas cost or time, a split-night studycan be ordered to diagnose OSA andtreatment during one visit. A splitnight study may be done if the AHIis 40/hour or greater during a minimum of 2 hours of recording (or ifthe AHI is 20 to 40/hour plus clinicaljudgment justifies the split study).6However, a split-night study maynot enable the clinician to determinethe full extent of the problem or itmay not be long enough to diagnosethe problem. A split-night study mayalso not be long enough to properlyfit the PAP device and adjust pressurefor optimum treatment, so unless thebenefits outweigh the need for thetwo-night study, a two-night study ispreferred over the split-night study.6Although CPAP significantly improves the patient’s signs and symptoms, adherence can be an issue.Patients have difficulty toleratingPAP if the mask is too tight, if leaksoccur and blow air into the face oreyes, or if nasal dryness is an issue.Properly fitting the mask is essential,and adding heated humidificationmay make the patient more comfortable. Thorough patient educationbefore initiating PAP therapy andfollow-up after the initial setup alsohelps improve adherence. Changingfrom a CPAP to a BPAP system maybe more comfortable. With this system, a different amount of pressureis provided during exhalation, usually less than that of inhalation. Patients who need CPAP pressures38 l Nursing2012 l AprilDetermining severityof OSA6SeverityEpisodes per hour ofapnea/hypopneaMild5-14Moderate15-30Severe 30greater than 15 cm H2O and patients who have pulmonary barotrauma, ear infections, or abdominaldistension from increased airwaypressures often do better on BPAP.6,12Increasing the amount of pressureslowly over time is called ramping; itlets the patient fall asleep first, whichmay make the device more comfortable. Most CPAP devices include theramping feature. In patients withoutnasal obstruction problems, the use ofnasal pillows or a nasal mask may bemore comfortable than a face mask.The patient may need a chin strap tomaintain an open airway.6,10,12Some problems from using CPAPare related to the mask or the drynessof the air. The pressure applied cancause dryness of the nasal passagesleading to congestion, rhinitis, and/orepistaxis. Pressure on the face fromthe mask or air leakage around themask can lead to skin irritation, allergies, or skin breakdown. Advise thepatient to keep the nasal passagesmoist (for example, with over-thecounter saline nasal spray or gels) andbe sure that the mask fits properly.Adding a humidifier can also helpmaintain airway moisture. If nasalsprays and humidification don’t work,the patient can try a heated humidified system as discussed earlier.Patients with claustrophobia maynot be able to tolerate any type of device. Many patients wear the devicefor part of the night only. As many as50% of patients don’t wear the deviceas prescribed.10,12More options for managing OSAPatients with mild OSA may betreated with custom made oralappliances (OAs), which aregenerally fitted by dentists, to keepthe tongue from obstructing theairway. OAs are recommended foruse in those patients with mildOSA who qualify for CPAP butdon’t want to use it and in patientswith mild-to-moderate OSA whodon’t respond to CPAP or in whomCPAP has failed. If an OA is used,a sleep study is recommended afterinitiation of the appliance to confirmits effectiveness.6Surgical treatments including palatal procedures are often used to treatpatients who snore, but they haven’tbeen consistently effective for OSA.1,6Surgery may be tried for patientswhen adequate control of OSA hasn’tbeen achieved with lifestyle changesand optimal treatment and adherence with PAP. Palatal surgery ofteninvolves uvulopalatoplasty, which isremoval of the uvula and part of thesoft palate.1,6Weight loss can help patients withOSA. Patients who haven’t been able tolose weight with dietary changes andwho have a BMI of 40 or more, or whohave comorbidities with a BMI of 35or more, can achieve major weight losswith bariatric surgery.6Occasionally, the anatomy of thepatient’s jaw may be part of the reason for the obstruction and treatment may include measures to movethe jaw and tongue forward and increase the airway diameter. Maxillomandibular surgery is invasive, andthe jaw must be wired shut duringthe healing process. Complicationsinclude paresthesias and mandibularmalposition, as well as general surgical complications such as bleeding,infection, and complications of general anesthesia. Maxillomandibularsurgery can alleviate OSA in up towww.Nursing2012.comCopyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
86% of certain patients.13 Daytimesleepiness that persists may be relatedto inadequate treatment or nonadherence to treatment.In general, medications (stimulants)approved for excessive daytime sleepiness are generally initiated when ESSscores remain at 10 or greater despiteeffective PAP treatment and when noother cause for sleepiness has beenidentified.6 The sleep center or theprimary care provider should closelyfollow patients being treated withmedication.Modafinil, considered standardtreatment, is an oral wakefulnesspromoting agent indicated to improvewakefulness in adult patients withexcessive sleepiness associated withnarcolepsy, OSA, and shift workdisorder.14 It’s generally well tolerated;headache is the most common adversereaction. Many patients usingmodafinil feel better, and some thinkthat they don’t need to use PAP. Continue to educate patients about needfor PAP as the mainstay of treatmentfor OSA.6Oxygen supplementation mayhelp some patients but isn’t recommended as a primary treatment forOSA.6Be on alert for complicationsAlthough the exact reason forsystemic hypertension that developsfrom OSA isn’t known, possiblefactors include hypoxia andhypercapnia, which increasesympathetic nervous system activity.These same mechanisms may alsoincrease the patient’s risk ofdeveloping other cardiovascularproblems, including myocardialischemia, heart failure, stroke, anddysrhythmias. In one 10-year study,patients with severe, untreated OSAwere 2.5 times more likely to have afatal cardiovascular event and 2.68times more likely to have a nonfatalwww.Nursing2012.comThe incidence of OSAincreases in patients whoare obese, smoke, drinkalcohol, and use sedatives.cardiovascular event than patientswith treated OSA, snorers withoutOSA, and controls.2Glucose intolerance, insulin resistance, and diabetes are potentialcomplications of OSA. Screen patients with OSA for diabetes. Theincidence of diabetes ranges fromabout 3% in those with mild OSA to15% in those with severe OSA.2Overall mortality is also increasedin patients with OSA. The more severe the disease, the greater the mortality. Those with moderate-to-severeOSA have a mortality of 33% over14 years, compared with 6.5% inpatients with mild OSA. These statistics are derived after adjusting forage, gender, BP, lipid levels, BMI,and other risk factors.2Rates of obesity increase as lengthof sleep decreases. Risk of obesity isless in patients who sleep at least7 hours per night. The hormones thathelp control appetite are thought tobe affected by lack of sleep. Leptin,an appetite suppressant, is reducedand ghrelin, an appetite stimulant, isincreased during sleep deprivation.Sympathetic nervous system activation, via OSA, may also influenceweight through changes in cortisol,growth hormone, inflammatorymarkers, and glucose metabolism. Inone study, those who slept 5 hours orless a night had a 65% increased riskof obesity compared with those whoslept 7 hours or more per night.Obesity is also a cardiovascular riskas well as a risk factor for diabetes,both potential complications ofOSA.2Due to OSA or its treatment withPAP, patients with OSA are likely tobe depressed. Besides helping withdepression, antidepressants may possibly lessen sleep apnea by decreasing rapid eye movement sleep. Evenso, the American Academy of SleepMedicine doesn’t recommend treating patients with OSA with selectiveserotonin reuptake inhibitors, theantidepressants used most often totreat depression.6Nursing interventionsNursing interventions begin withidentifying patients at risk for OSA.Assess every patient for potential riskfactors as part of your patient’s healthhistory, even if the patient hasn’texpressed concerns about signs andsymptoms of OSA, such as snoringand excessive daytime sleepiness.Pay particular attention to patientswith neurobehavioral problems suchas anxiety, depression, anger, andADHD; cardiovascular problemssuch as hypertension, heart failure,angina and/or myocardial infarction,dysrhythmias, or stroke; type 2diabetes; and/or obesity.Sleep deprivation may also resultfrom poor sleep hygiene as well asOSA. If the patient history suggestsApril l Nursing2012 l 39Copyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
poor sleep habits, discuss proper sleephygiene with your patient. Topicscan include going to bed and arisingat the same time every day, includingdays off; using the bedroom for onlysleep and sex; and keeping the roomdark and cool.Consider discussing “GoingGreen” with your patient: Green forthe environment and green for thewallet! Because obesity contributesto the development of OSA and canresult from OSA, encourage reducingand maintaining body weight. Oneway for your patient to be “green”is to walk or ride a bike to work, iffeasible. Another way is for your patient to increase the intake of “green”foods and foods of other colors byeating more vegetables and fruitsand reducing high-calorie and highfat foods, such as those that are fried,processed, or have a high glycemicindex. Doing these “green” interventions will put “green” in the patient’spocket by saving money on auto fueland maintenance costs as well asdecreasing food costs. Losing weightincreases “green” in the pocket bydecreasing health risks associatedwith obesity such as cardiovasculardisease, diabetes, and cancer. Manyof these health issues are also riskfactors associated with OSA.Smoking cessation will decreasethe risk of OSA as well as put “green”in your patient’s pocket by decreasingdaily costs and potential healthcarecosts related to the risks of smoking.Discuss other lifestyle changes withyour patient, such as decreasing orabstaining from alcohol and sedatives,especially before bedtime. These substances may contribute to sleep disruption and relaxation of the musclesof the oral airway, leading to airwayobstruction.9Sleeping position can affect thetongue’s position. Having the patientraise the head of the bed with a wedge40 l Nursing2012 l AprilHaving the patient raise thehead of the bed can keepthe tongue forward andreduce GERD symptoms.device, use a hospital-type bed, orelevate the legs of the head of thebed on blocks can not only keepthe tongue forward but also reduceGERD symptoms. Sleeping in a lateral position will move the tonguelaterally and prevent obstruction.Patients should avoid using extrapillows to elevate their head becausethis tends to cause cervical flexionand increased intra-abdominal pressure, increasing the risk of both OSAand GERD.6,10 Patients who do betterwith positional changes are typicallyyounger and thinner and have lesssevere OSA.6,10Another major concern to discussat each appointment with your patient is excessive daytime sleepiness,which may lead to motor vehiclecrashes and injuries at work. An Australian study demonstrated that truckdrivers with ESS scores greater than18 had almost three times more colli-sions than truck drivers without OSA.In an Internet study of over 35,000participants, respondents with OSAreported having collisions and nearmiss collisions two times more oftenthan drivers who didn’t have OSA.Patients with OSA using drivingsimulations have performance values similar to drivers impaired byalcohol.The U.S. Department of Transportation published guidelines inearly 2008 for commercial motorvehicle drivers with OSA. According to these recommendations, drivers should be screened for OSA and,if the problem is diagnosed, treatedeffectively. These drivers need continued monitoring of the problemand treatment. Nurses should inform patients that their judgment islikely to be impaired and that theyneed to effectively use PAP and anyprescribed medications, and to participate in close follow-up to protectthemselves and others from motorvehicle crashes.15Waking up to the risksNurses should be aware that OSAincreases with age and know the riskfactors for OSA. Those with riskfactors for OSA should be referred toa sleep center.1,6,10Our executive, Mr. J, was referredto a sleep center and was found tohave moderate OSA. He was fittedwith a CPAP device at a setting of12 cm H2O and was followed upmonthly for the first 6 months toensure proper use and to answer hisquestions. After that time, he wasfollowed every 6 months. He wastaught about sleep hygiene andmaintaining a proper body weightthrough diet and exercise. Aftercontinuing to complain of excessivedaytime sleepiness, he was startedon modafinil. To date, he uses hisCPAP most nights of the week andwww.Nursing2012.comCopyright 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
his hypertension is well-controlled.He’s getting 7 to 8 hours of sleepmost nights and is more productiveboth at work and at home. He sayshe feels like a new and youngerman, is better able to concentrate, isno longer taking naps in the officebehind a closed door, and has moreenergy and fewer headaches. Hiswife and kids say he’s much nicer tolive with as well, and he no longersnores when using his CPAP. REFERENCES1. Park JG, Ramar K, Olson EJ. Updates on definition,consequences, and management of obstructive sleepapnea. Mayo Clin Proc. 2011;86(6):549-555.2. Valerio TD. Much more than a nuisance: healthconsequences of sleep disorders. Adv Nurse Pract.2009;17(9):57-60.3. Eckert DJ, Malhotra A. Pathophysiology ofadult obstructive sleep apnea. Proc Am Thorac Soc.2008;5(2):144-153.4. Isono S. Obstructive sleep apnea of obese adults:pathophysiology and perioperative airwaymanagement. Anesthesiology. 2009;110(4):908-921. 5. Lam JC, Sharma SK, Lam B. Obstructive sleepapnoea: definitions, epidemiology and naturalhistory. Indian J Med Res. 2010;131(2):165-170.12. Shapiro GK, Shapiro CM. Factors thatinfluence CPAP adherence: an overview. SleepBreath. 2010;14(4):323-335.6. Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinicalguideline for the evaluation, management andlong-term care of obstructive sleep apnea in adults.J Clin Sleep Med. 2009;5(3):263-276.13. Meslemani D, Jones LR. Skeletal surgery insleep apnea. Curr Opin Otolaryngol Head Neck Surg.2011;19(4):307-311.7. Gurubhagavatula I. Consequences of obstructivesleep apnoea. Indian J Med Res. 2010;131:188-195.8. Zonato AI, Martinho FL, Bittencourt LR, deOliveira Camponês Brasil O, Gregório LC, Tufik S.Head and neck physical examination: comparisonbetween nonapneic and obstructive sleep apneapatients. Laryngoscope. 2005;115(6):1030-1034.9. Haeck PC, Swanson JA, Iverson RE, Lynch DJ;ASPS Patient Safety Committee. Evidence-basedpatient safety advisory patient assessment andprevention of pulmonary side effects in surgery.Part 1. Obstructive sleep apnea and obstructivelung disease. Plast Reconstr Surg. 2009;124(4 suppl):45S-56S.10. WebMD. Sleep Disorders Health Center. .htm.11. Collop NA, Anderson WM, Boehlecke B, et al.Portable monitoring task force of the AmericanAcademy of Sleep Medicine: clinical guidelines forthe use of unattended portable monitors in thediagnosis of obstructive sleep apnea in adultpatients. Portable Monitoring Task Force of theAmerican Academy of Sleep Medicine. J Clin SleepMed. 2007;3(7):737-747.14. Provigil (modenafil) tablets prescribinginformation. Frazer, PA: Cephalon, Inc.; 2010. http://provigil.com/media/PDFs/prescribing info.pdf.15. Department of Transportation. Expert panelrecommendations: obstructive sleep apnea andcommercial motor vehicle driver safety. 16. Rinaldi V, Casale M, Faiella F, Pappacena M,Salvinelli F. Sleep-disordered breathing and CPAP:overview of sleep-disordered breathing. 2011. iew.Susan Simmons is a family NP at Olathe MedicalServices in Olathe, Kan. Bill Pruitt is senior instructorand director of clinical education in cardiorespiratorysciences at the School of Allied Health at the Universityof South Alabama in Mobile, Ala. Both authors aremembers of the editorial board of Nursing2012.The authors and planners have disclosed that theyhave no financial relationships related to this r more than 27 additional continuing education articles related torespiratory topics, go to NursingCenter.com/CE. Earn CE credit online:Go to http://www.nursingcenter.com/CE/nursing andreceive a certificate within minutes.INSTRUCTIONSSounding the alarm for patients with obstructive sleep apneaTEST INSTRUCTIONS To take the test online, go to our secure website athttp://www.nursingcenter.com/ce/nursing. On the print form, record your answers in the testanswer section of the CE enrollment form on page 42.Each question has only one correct answer. You maymake copies of these forms. Complete the registration information and courseevaluation. Mail the completed form and registrationfee of 24.95 to: Lippincott Williams & Wilkins, CEGroup, 2710 Yorktowne Blvd., Brick, NJ 08723. We willmail your certificate in 4 to 6 weeks. For faster service,include a fax number and we will fax your certificatewithin 2 business days of receiving your enrollmentform. You will receive your CE certificate of earned contacthours and an answer key to review your
ness and impaired concentration may be so intense that they interfere with the patient's ability to function at work. Falling asleep at work, show-ing up late, not completing work on schedule, being forgetful, and having mood changes may diminish an em-ployee's productivity. Work perfor-mance may deteriorate so much that