Transcription
Primary Care Pharmacists TrainingNetworkInjectable therapies in DiabetesPart 116.3.22‘made ridiculously simple’SpeakerProf. Saqib MahmudFRCP(Edin) FRCP(Glasg) FRCP(London) FRCGP16.3.22Toronto 1921 –Banting & Best
Common sense in not socommon “Voltaire”
Guidelines are not railway lines
Guidelines are better described as hand rails.
Personalized Goals / HbA1c targetsLessstringentMORE STRINGENTCONTROLoShort disease durationoNo hypoglycemiaoLong life expectancyoNo ESS STRINGENT CONTROLo Long disease durationo H/o recurrenthypoglycaemiao Short life expectancyo Multiple co-morbiditieso Not motivated
Glucose-lowering medication in T2D: overall approachTO AVOID CLINICALINERTIA REASSESSAND MODIFYTREATMENTREGULARLY(3-6 MONTHS)FIRST-LINE THERAPY IS METFORMIN AND COMPREHENSIVE LIFESTYLE (INCLUDING WEIGHT MANAGEMENT AND PHYSICAL ACTIVITY )INDICATORS OF HIGH-RISK OR ESTABLISHED ASCVD, CKD OR HF†NOConsider independently of baseline HbA1c or individualized HbA1c target ASCVD PREDOMINATESEstablished ASCVDIndicators of high ASCVD risk (age 55years LVH or coronary, carotid, lowerextremity artery stenosis 50%)PREFERABLY GLP-1 RA with proven CVDbenefit1ORSGLT2i with proven CVD benefit1 if eGFRadequate2If HbA1c above targetIf further intensification is required orpatient is now unable to tolerateGLP-1 RA and/or SGLT2i, chooseagents demonstrating CV safety: For patients on a GLP-1 RA, consideradding SGLT2i with proven CVDbenefit1 DPP-4i if not on GLP-1 RA Basal insulin4 TZD5 SU6 If HbA1c above individualized target proceed as belowHF OR CKD PREDOMINATESParticularly HFrEF (LVEF 45%)CKD: Specifically eGFR 30-60 ml min-1[1.73m]-2 or UACR 30 mg/g, particularly UACR 300 mg/gCOMPELLING NEED TO MINIMISE HYPOGLYCAEMIAPREFERABLYSGLT2i with evidence of reducingHF and/or CKD progression inCVOTs if eGFR adequate3ORIf SGLT2i not tolerated or contraindicatedor if eGFR less than adequate2 addGLP-1 RA with proven CVD benefit1DPP-4iGLP-1 RASGLT2i2TZDIf HbA1c abovetargetIf HbA1c abovetargetIf HbA1c abovetargetIf HbA1c abovetargetSGLT2i2ORTZDSGLT2i2ORTZDGLP-1 RAORDPP-4iORTZDSGLT2i2ORDPP-4iORGLP-1 RACOST IS A MAJOR ISSUE9-10COMPELLING NEED TO MINIMISE WEIGHTGAIN OR PROMOTE WEIGHT LOSSGLP-1 RAEitherwith good/ORSGLT2i2efficacy for8weight lossSU6If HbA1c above targetSGLT2i2TZD10If HbA1c above targetGLP-1 RA withgood efficacyfor weightloss8TZD10SU6If HbA1c above targetIf HbA1c above targetIf HbA1c above targetIf HbA1c above targetContinue with addition of other agents as outlined above Avoid TZD in the setting of HF Chooseagents demonstrating CV safety:For patients on a SGLT2i, consideradding GLP-1 RA with proven CVDbenefit1DPP-4i (not saxagliptin) in the settingof HF(if not on GLP-1 RA)Basal insulin4SU6†Actioned whenever these become new clinical considerations regardless of background glucose-lowering medications.1.Proven CVD benefit means it has label indication of reducing CVD events.2.Be aware that SGLT2i labelling varies by region and individual agent with regard to indicated level of eGFR for initiation and continued use3.Empagliflozin, canagliflozin and dapagliflozin have shown reduction in HF and to reduce CKD progression in CVOTs. Canaglifloz in has primary renal outcomedata from CREDENCE, Dapagliflozin has primary heart failure outcome data from DAPA-HF4.Degludec and U100 glargine have demonstrated CVD safety5.Low dose may be better tolerated though less well studied for CVD effectsIf HbA1c above targetConsider the addition of SU6 OR basal insulin: Choose later generation SU with lower risk of hypoglycaemia Consider basal insulin with lower risk of hypoglycaemia 76.7.8.9.10.Choose later generation SU to lower risk of hypoglycaemia, Glimepiride has shown similar CV safety to DPP-4iDegludec / glargine U300 glargine U100 / detemir NPH insulinSemaglutide liraglutide dulaglutide exenatide lixisenatideIf no specific comorbidities (i.e. no established CVD, low risk of hypoglycaemia and lower priority to avoid weight gain or no weight-related comorbidities)Consider country- and region-specific cost of drugs. In some countries TZDs relatively more expensive and DPP-4i relatively cheaperUpdates to the 2018 consensus report are indicated in red fontBuse et al. Diabetes Care 2019; doi:10.2337/dci19-0066: dci190066; Buse JB et al. Diabetologia 2019;doi:10.1007/s00125-019-05039-wIf quadruple therapy required, orSGLT2i and/or GLP-1 RA not toleratedor contraindicated, use regimen withlowest risk of weight gainPREFERABLYDPP-4i (if not on GLP-1 RA)based on weight neutrality Insulin therapy basal insulin with lowestacquisition costORConsider DPP-4i OR SGLT2i with lowestacquisition cost10If DPP-4i not tolerated orcontraindicated or patient already onGLP-1 RA, cautious addition of: SU6 TZD5 Basal insulinASCVD, atherosclerotic CVD; CVD, cardiovascular disease; CKD, chronic kidney disease; CV, cardiovascular;DPP-4i, dipeptidyl peptidase 4 inhibitors; eGFR, estimated glomerular filtration rate; GLP-1 RA, glucagon like peptide-1 receptor agonist; HbA1c,hemoglobin A1c; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; LVEF, left ventricular ejection fraction; LVH, left ventricularhypertrophy; MACE, major adverse cardiovascular event; SGLT2is, sodium glucose like cotransporter 2 inhibitors; SU, sulfonylureas; T2D, type 2 diabetes;TZD, thiazolidinediones; UACR, urine albumin creatinine ratio
FIRST-LINE THERAPY IS METFORMIN AND COMPREHENSIVE LIFESTYLE(INCLUDING WEIGHT MANAGEMENT AND PHYSICAL ACTIVITY)ASCVD predominates Established ASCVD Indicators of highASCVD risk (age 55years LVH orcoronary, carotid,lower extremity arterystenosis 50%)HF OR ineCLINICAL1cINERTIA HbAREASSESSorANDindividualizedMODIFY TREATMENTREGULARLYHbA(3-6MONTHS)1c targetASCVDPREFERABLYPREDOMINATESGLP-1 RA Particularly HFrEF (LVEF 45%) CKD: Specifically eGFR 30-60 mlmin-1 [1.73m]-2 or UACR 30 mg/g, particularly UACR 300 mg/gSGLT2iORwith proven CVD benefit1 if eGFR adequate2CKD or HF predominatesPREFERABLYwith proven CVD benefit1SGLT2iLOOK FOR INDICATORS OFHIGH-RISK OR ESTABLISHEDASCVD, CKD OR HF†If HbA1c above target Basal insulin TZD (avoid in HF) SUwith evidence of reducing HF and/or CKD progression inCVOTs if eGFR adequate3ORIf SGLT2i not tolerated or contraindicatedor if eGFR less than adequate2 addGLP-1 RAwith proven CVD benefit1
FIRST-LINE THERAPY IS METFORMIN AND COMPREHENSIVE LIFESTYLE(INCLUDING WEIGHT MANAGEMENT AND PHYSICAL ACTIVITY)GLP-1 RASGLT2iIf HbA1c above targetSGLT2iCOMPELLING NEED TOMINIMISE WEIGHT GAINOR PROMOTE WEIGHTLOSSTOAVOIDCLINICALINERTIA REASSESSANDMODIFY TREATMENT REGULARLY(3-6 MONTHS)Either/ORGLP-1 RAwith good efficacyfor weight loss8SGLT2iIf HbA1c above targetIf HbA1c abovetarget Basal insulin TZD (avoid in HF) SUGLP-1 RA
Intensifying to injectable therapiesGLP1 RAINSULIN.are the preferred choice toinsulinIn patients who need thegreater glucose-loweringeffect of an injectablemedicationGLP1 RAbeforeInsulinGLP1 RAINSULINFor patientswith extreme andsymptomatichyperglycaemia
1Biggest challengeTimely initiation andintensification‘major issue’2More often T2Dpatients are left in poorglycaemic control3Preparationfor future Rx optionsHigher the HbA1c – thegreater the risk ofcomplicationsDiscussing the eventual need forinsulin at diagnosis of T2Dor early on.Challenges
11TAB ONEAdd your own text hereBarriers to startinginsulinProvider’sperceptionA. Insulin therapy is toocomplex to manage in abusy primary care practiceB. May cause weight gainC. Increase the risk ofhypoglycaemia
TAB ONEAdd your own text here1Patients Concerns & beliefs that insulincausesA. weight gain, hypoglycaemia,interference with life.B. late stage complications eg,gangrene, amputationC. Indication of imminentdeterioration or deathBarriers tostarting insulinPatient’sperceptions2
1TAB ONEAdd your own text hereOverview of3GLP1 RA Low risk of hypos Promote weight loss Effective HbA1c reduction by 1%(11mmol/mol) Can be combined with insulin Principal advantage over insulin is tofacilitate weight loss and reduceappetite, increase satietyCV benefits with some agents
GLP-1 secreted uponthe ingestion of food
Intensifying to injectable therapiesIn patients who need the greaterglucose-lowering effect of aninjectable medication*GLP-1 receptoragonists† arethe preferredchoice to insulinFor patients with extreme andsymptomatic hyperglycaemiaInsulin‡ isrecommended*If Hb1Ac above target despite dual/triple therapy †Consider choice of GLP-1 receptor agonist considering patient preference, HbA1c lowering, weight-lowering effect or frequency of injection. IfCVD, consider GLP-1 receptor agonist with proven CVD benefit; ‡Consider insulin as preferred to GLP-1 receptor agonist if symptoms of hyperglycaemia are present, or evidence of ongoingcatabolism (polyuria, polydipsia or weight loss). CVD, cardiovascular disease;GLP-1, glucagon-like peptide-1; HbA1c, glycosylated haemoglobin.Davies MJ et al. Diabetes Care. 2018;41:2669–2701; Davies MJ et al. Diabetologia. 2018;61:2461–2498.
Use of concomitant oral therapy when intensifying to injectablesSGLT-2iSGLT-2iBeware: DKA (euglycaemia) Instruct on sick-day rules Do not down-titrate insulinover-aggressivelySUConsider stopping SU if prandialinsulin initiated or on a premixinsulin regimenIf on SGLT-2i continueIf on SGLT-2i, continuetreatmenttreatment.Consider adding SGLT-2iConsider adding SGLT-2i if: if: Established CVDEstablishedCVD IfHbA1c is abovetarget or asaid weightIf HbAreduction1c above targetor as weight reductionaidSU stopIf on SU,stopororreducereducedosedoseby 50% when basal insulininitiatedisinitiatedMetforminDPP-4iContinue treatment withMetforminmetforminStop DPP-4i if GLP-1RAinitiated is initiatedGLP-1RATZDStop TZD whencommencing insulin ORreduce dose3CVD, cardiovascular disease; DKA, diabetic ketoacidosis; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist; HbA1c, glycosylatedhaemoglobin; SGLT-2i, sodium-glucose cotransporter-2 inhibitor; SU, sulphonylurea; TZD, thiazolidinedioneDavies MJ et al. Diabetes Care 2018. dci180033; Davies MJ et al. Diabetologia 2018;61(12):2461-2498
Positioningin thecurrenttreatmentpathways After metformin with excess weight or presenceof ASCVD/ risk factors Can be added on at any stage / duration ofdisease Choice of GLP1 and which patient isindividualized to the clinical need and patientpreference Can be combined with SG:T2i for synergisticeffect for robust and effective weight loweringas well as glycaemic control Can be added on to patients who have been oninsulin(any regimes and developed huge amountof insulin resistance and lost control
Available GLP1 therapiesWhich one?
GLP1 injection sitesClinical trial design and results template24
InitiatingGLP1How1One dailyVictoza / liraglutide2Once weeklyStart 0.25mg weekly – 1monthOzempic/semaglutidetitrate to 0.5mg month 234Start with 0.6mg dose dailyfor a week, then 1.2mgCan be increased to 1.8mgStay on 0.5mg or increase to 1mgOnce weeklyTrulicity/ dulaglutideRecommended dose is1.5mg weeklyAlso available in 0.75mg doseOnce weeklyBydureon BciseSingle dose prefilled pen,no titration.GLP1 therapies
1Hba1c reduction & weight loss.TABA.ONEAdd your own text hereB. Ozempic, Victoza & Trulicity canbe used up to eGFR 15,Bydureon up to eGFR 50C. Compliance, tolerability, sideeffectsD. No BM monitoring requiredE. Switching from one GLP1 toanotherMonitoring& review4
1?TAB ONEAdd your own text hereWho are the bestcandidates forInsulin / GLP-1 RAor SGLT2icombination?1. T2D patients failing toachieve glycaemic targetswith basal insulin2. Above Over weight /high BMIs3. Recurrent Hypoglycaemiawith insulin regimeintensification
GLP1 RA in Combination with basal insulin1Basal InsulinPronouncedPPG control3Basal InsulinWeight loweringNo increase in hypoglycaemiaSGLT2iControlsNocturnal & FPGGLP1 - RA2ModestWeight gain.GLP1 - RA4
Expert patient’s perspectivesof GLP1
Expert patient’sperspectives ofGLP1
After treatment with GLP1 RAHis current HbA1c is 34,(remission range)3/12 ago was also 36His BMI is now 34,previously was 45Before treatment with GLP1 RA
1ooooShort actingNovorapid /FIASP- Novo NordiskHumalog / lispro(lyumjev)- LillyApidra Sanofi- AventisTrurapi (biosimilar aspart)3PremixedinsulinNovomix 30 - Novo Nordisko Human Actrapid -- Novo Nordisko Humulin S - Lillyo Insuman Rapid - Sanofi- AventisRapid actingAnalogue2o Human Mixtard 30 - Novo Nordisko Humulin M3 - Lillyo Insuman Comb 15,25,50- Sanofi- AventisBiphasic InsulinAspartTypes of Insulins45o Humalog Mix 25 – Lillyo Humalog Mix 50 - LillyBiphasic InsulinLispro.o Human Insulatard - Novo Nordisko Humulin I - Lillyo Insuman Basal - Sanofi- Aventis7Long actingAnalogueo Insulin Degludec(Tresiba) - Novo NordiskoooIntermediateacting - NPH6Insulin Glargine (Lantus) – SanofiInsulin Detemir (Levemir) – Novo NordiskBiosimilar glargine (Abasaglar – Lilly)o(Semglee - Mylan)Extendedlong-acting8
ooooNovorapid /FIASP- Novo NordiskHumalog / lispro(lyumjev)- LillyApidra, Trurapi (biosimilar aspart)SanofiRapid actingAnalogue27Long actingAnalogueooooInsulin Glargine (Lantus) – SanofiInsulin Detemir (Levemir) – Novo NordiskBiosimilar glargine (Abasaglar – Lilly)(Semglee - Mylan)Types of InsulinsBrand names of the products are used to differentiate various types of insulins.Actrapid, Novorapid, FIASP, Insultard, Mixtard, Levemir, Novomix and Tresiba are registered trademarks of Novo Nordisk. Humulin, Humalog and Abasaglar are registered trademarks of Eli Lilly. Insuman, Apidra and Lantus are registetrademarks of Sanofi.
InitiatingInsulinWhenAPoor control onmaximum multipleoral therapiesBLong duration ofT2D poor controlCFailure to get toHbA1c targetDBMs consistently doublefigures / Hba1c 11% (97 )complications eg; worseningneuropathy or retinopathy,leg ulcers, digital gangrenedespiteintensificationInitial A1C than 9%( 75mmol/mol)DKA.Indications to initiate insulin
Ideal Basal/Bolus Insulin – elementary principal75BreakfastLunchDinnerGlucoseBolus InsulinBase InsulinPlasmaInsulin 50( yler J, Kelley’s Textbook of Internal Medicine 2000.
Initiating InsulinHow?3 Steps
1Initiation(usually bedtime) Alternative – Pre-mixed insulin(twice daily) Titrate dose of basal insulinaccording to FPG levels3 once daily – Basal insulinIntensificationBasal plus GLP- 1 RA SGLT2iTitration2 Basal bolus(1x short acting/prandial insulin) Basal bolus(2 - 3 x short acting/ prandial insulin)OR
Initiating InsulinWhich insulin?
1TAB ONEAdd your own text hereInitiating InsulinAWhich insulin shouldbe used initiallyfor T2DM ? Begin with BASALinsulin such as InsulinGlargine Onset – 1-2hrs Duration of action – upto 24 hours Injected at bed-time
1TAB ONEFPGofhere5 - 7mmol/lAddTargetyour owntext Patients to self titrate gently byincreasing the dose by 1 U every night 2 U every 3 days until FPG target of 5 –7 mmol/L If fasting hypoglycaemia occurs, thedose of bedtime basal insulin shouldbe reducedDose titrationBasal insulin asadd on to OHAsB
1TAB ONEAdd your own text hereInitiating InsulinCWhat dose? a set dosage of 10 U ofglargine daily,or by using weight-basedequations
Injection sites
How do I count carbohydrate?
Macronutrient Conversion to Blood Glucose
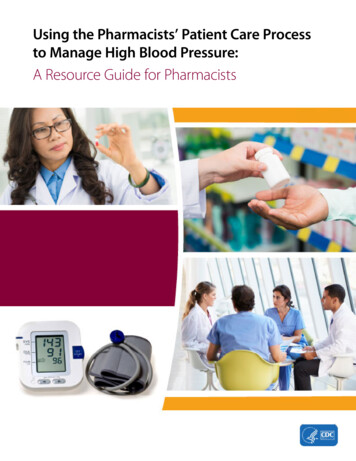
What is aninsulin-tocarbohydrateratio? An insulin-to-carb ratio tells you how muchrapid acting insulin you need for specificamount of carbohydrate It allows you to dose your insulin based on theamount of carbohydrate that you eat at a meal For example, an insulin-to-carb ratio of 1:10means 1 unit of insulin will cover 10 grams ofcarbohydrate Some people have a different insulin-to-carbratio for breakfast than at other meals To use an insulin-to-carb ratio, you need tocount the carbohydrate at a meal.
Add up the carbohydrate in your meal or snackExample:1 cup cooked rice 45 g½ cup green beans .0 gHow do Icountcarbohydrate?3 oz grilled chicken breast .0 g Salad greens and dressing .0 g1 cup strawberries. . .7 gTotal Carbohydrate52 gTake the total carbohydrate and divide it by the second number in the insulin-tocarb ratioExample: If your insulin to carb ratio is 1:10, then 1 unit of insulin will cover 10 grams ofcarbohydrate 52 grams of carbohydrate 10 5.2 This means you would need 5 units of insulin to cover this meal (round thenumber down to 5).
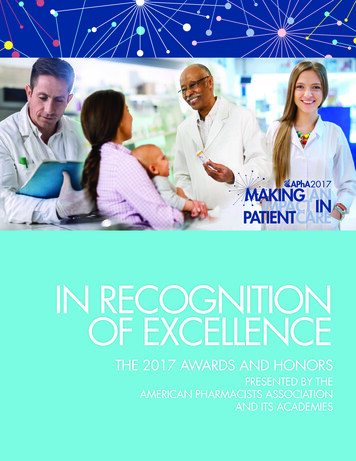
Lipohypertrophy Injection sites should be examinedonce a year Patients should be taught to inspecttheir own sites and should be giventraining in site rotation, correctinjection technique as well as indetection and prevention Switching injections fromlipohypertrophic to normal tissueoften requires a decrease in the doseof insulin injected
Lipohypertrophyis also associatedwith needlereuse
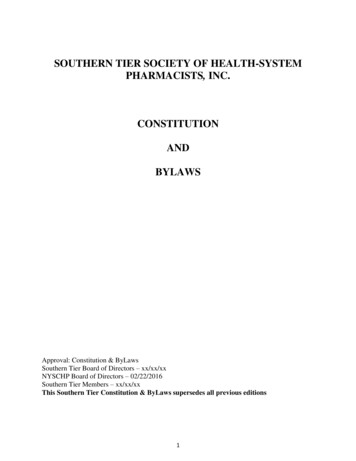
I-port
Factors That Affect Absorption Insulin should be injected in subcutaneouslayer where absorption is predictable andconsistent Accidental absorption in muscle can speedup insulin absorption and causehypoglycaemia
Bydureon Bcise GLP1 therapies Initiating GLP1 How. TAB ONE 1 Add your own text here A. Hba1c reduction & weight loss. B. Ozempic, Victoza & Trulicity can be used up to eGFR 15, Bydureon up to eGFR 50 C. Compliance, tolerability, side effects D. No BM monitoring required E. Switching from one GLP1 to another