Transcription
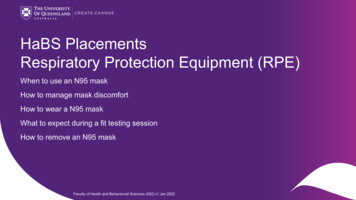
Silica Respirator QuestionnaireINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESPatient name:Employer:To the employer: Answers to questions in Section 1, and to question 9 in Section 2 of Part A, do not require a medical examination.However, certain responses, or patterns of response, may lead the reviewer to request further information, or a medical examination,in order to reach a conclusion regarding the employee’s ability to safely use a respirator.To the employee, Patient ID: Your employer must allow you to answer this questionnaire during normal workinghours, or at a time and place that is convenient to you. To maintain your confidentiality, your employer or supervisor must not lookat or review your answers, and your employer must tell you how to deliver or send this questionnaire to the health care professionalwho will review it.Can you read?YesNoPart A. Section 1. (Mandatory)Every employee who has been selected to use any type of respirator must provide the following information.1. Sex:MaleFemale2. Your height: ft. in.3. Your weight: lbs.4. Your job title:5. A phone number where you can be reached by the health care professional who reviews this questionnaire (include area code):( ) -6. The best time to call you at this number: a.m./p.m.7. Has your employer told you how to contact the health care professional who will review this questionnaire?YesNo8. Check box(es) of the type of respirator you will use. (You can check more than one category).N, R or P disposable respirator (filter-mask, non-cartridge type only).Other type (for example, half- or full-face piece type, powered-air purifying, supplied-air, self-contained breathing apparatus).9. Have you worn a respirator?YesNoIf “yes” what type(s)?Minnesota Occupational HealthSt. PaulEaganBlainemohonline.com1Form Update 5/22/2018
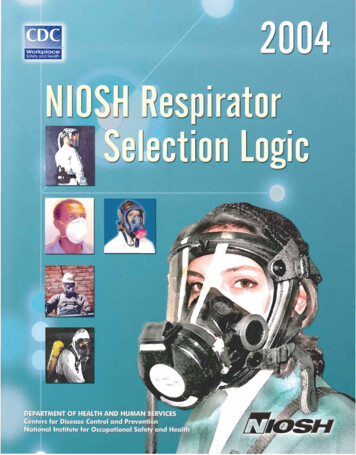
INTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESPart A. Section 2. (Mandatory)Every employee who has been selected to use any type ofrespirator must answer questions 1 through 9 below.Coughing that wakes you early in the morningCoughing that occurs mostly when you are lying down1. Do you currently smoke tobacco, or have you smokedtobacco in the last month?YesNoCoughing up blood in the last month2. Have you ever had any of the following conditions?Wheezing that interferes with your jobWheezingSeizures (fits)Chest pain when you breathe deeplyDiabetes (sugar disease) Anyother symptoms that you think may be related tolung problemsAllergic reactions that interfere with your breathingClaustrophobia (fear of closed-in places)5. Have you ever had any of the following cardiovascular orheart problems?Trouble smelling odorsHeart attack3. Have you ever had any of the following pulmonaryor lung problems?StrokeAsbestosisAnginaAsthmaHeart failureChronic bronchitisSwelling in your legs or feet (not caused by walking)EmphysemaHeart arrhythmia (heart beating irregularly)PneumoniaHigh blood pressureTuberculosisAny other heart problem that you’ve been told aboutSilicosis6. Have you ever had any of the following cardiovascularor heart problems?Pneumothorax (collapsed lung)Lung cancerFrequent pain or tightness in your chestBroken ribsPain or tightness in your chest during physical activityAny chest injuries or surgeries Painor tightness in your chest that interferes withyour jobAny other lung problem that you’ve been told about Inthe past two years, have you noticed your heartskipping or missing a beat4. Do you currently have any of the following symptoms ofpulmonary or lung illness?Heartburn or indigestion that is not related to eatingShortness of breath Anyother symptoms that you think may be related toheart or circulation problems Shortnessof breath when walking fast on level groundor walking up a slight hill or incline Shortnessof breath when walking with other people atan ordinary pace or level ground7. Do you currently take medication for any of the followingproblems?to stop for breath when walking at your own paceon level groundBreathing or lung problemsShortness of breath when washing or dressing yourselfBlood pressure ShortnessSeizures (fits) HaveHeart troubleof breath that interferes with your jobCoughing that produces phlegm (thick sputum)Minnesota Occupational HealthSt. PaulEaganBlainemohonline.com2Form Update 5/22/2018
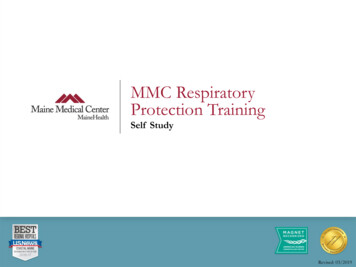
INTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICES8. If you’ve used a respirator, have you ever had any of thefollowing problems?12. Have you ever had an injury to your ears, includinga broken ear drum?YesNoEye irritation13. Do you currently have any of the following hearingproblems?Skin allergies or rashesAnxietyDifficulty hearingGeneral weakness or fatigueWear a hearing aid AnyAny other hearing or ear problemother problem that interferes with your useof a respirator14. Have you ever had a back injury?9. Would you like to talk to the health care professional whowill review this questionnaire about your answers to thisquestionnaire?YesNo15. Do you currently have any of the followingmusculoskeletal problems?Weakness in any of your arms, hands, legs or feetQuestions 10 to 15 must be answered by every employee whohas been selected to use either a full-face piece respirator ora self-contained breathing apparatus (SCBA). For employeeswho have been selected to use other types of respirators,answering these questions is voluntary.Back painDifficulty fully moving your arms and legs Painor stiffness when you lean forward or backwardat the waistDifficulty fully moving your head up or down10. Have you ever lost vision in either eye (temporarily orpermanently)?YesNo Difficultyfully moving your head side to sideDifficulty bending at your knees11. Do you currently have any of the following vision problems?Difficulty squatting to the groundWear contact lenses Climbinga flight of stairs or a ladder carrying morethan 25 lbsWear glassesColor blind Anyother muscle or skeletal problem that interfereswith using a respiratorAny other eye or vision problemRespirator Physical Exam:HEIGHT:Physical ExamWEIGHT:PULSE:NBLOOD PRESSURE (sitting):AbPhysical Exam (cont.)1. Eyes7. Beard/Mustache2. Nose8. Neck3. Oropharynx9. Lung4. Teeth10. Hear5. Outer Ear11. Extremities6. Ear Canal12. TM’sNAbComments:Minnesota Occupational HealthSt. PaulEaganBlainemohonline.com3Form Update 5/22/2018
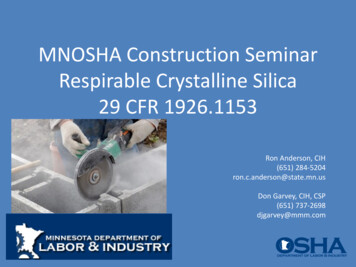
INTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESInitial/Periodic Hazmat Exam Questionnaire1. Are you a member of a HAZ/MAT team?.YesNo2. Have you worn protective equipment (clothes, safety glasses, respirator, hearing protection)?.YesNo3. Have you participated in workplace medical monitoring (blood, urine, chest x-ray, respirator program?.YesNo1. Severe allergic reaction, difficulty breathing or swallowing.YesNo2. Heart pain, palpitations, heart muscle damage.YesNo3. Cough, shortness of breath, wheezing, asthma, lung damage, abnormal breathing tests or chest x-ray.YesNo4. Dizziness, fainting, blackouts, seizure, headaches, fatigue.YesNo5. Arm or leg weakness, numbness, pins/needles sensation.YesNo6. Abnormal liver blood tests, liver damage, hepatitis, weight loss, jaundice.YesNo7. Abdominal pain, stomach or intestinal problems, weight loss, blood in stool.YesNo8. Abnormal kidney blood or urine tests, kidney damage.YesNo9. Rash, skin cancer.YesNo10. Abnormal blood counts, anemia, swollen glands.YesNo11. Heat, cold illness, burns, frostbite.YesNo12. Difficulty with mood, memory, concentration.YesNo1. Hay fever, allergic rhinitis.YesNo2. Asthma, chronic bronchitis, COPD.YesNo3. Heart disease, congestive heart failure, hypertension, atrial fibrillation.YesNo4. Ulcers, Crohn’s disease, diverticulitis.YesNo5. Hepatitis, cirrhosis, liver disease, gallbladder disease.YesNo6. Stroke, seizures, depression, anxiety, dementia, Parkinson’s disease, multiple sclerosis.YesNo7. Leukemia, lymphoma, cancer.YesNo8. Another chronic/serious health condition.YesNo9. Any disability, physical limitation.YesNo10. Have you had any type of surgery.YesNoHave you ever experienced any of the following symptoms or conditions due to workplace exposure?Have or have had any of the following medical conditions?11. In previous jobs, did you have any occupational exposure to respirable silica:.YesNoIf yes, what was your job?12. What is your current level of occupational exposure to respirable silica?13. What is your current job?14. What is your anticipated level of future occupational exposure to respirable silica?15. Describe any personal protective equipment currently used, or to be used, to protect against respirable silica exposure:Minnesota Occupational HealthSt. PaulEaganBlainemohonline.com4Form Update 5/22/2018
INTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESHave/had any of the following musculoskeletal conditions:1. Back injury, strain, herniated disc, recurring ache.2. Neck problems, neck pain, whiplash.3. Bursitis, tendonitis.4. Foot or ankle problems.5. Fractures.6. Hand, wrist, elbow problem.7. Knee or shoulder problems.YesYesYesYesYesYesYesNoNoNoNoNoNoNoWhat year was your last diphtheria/tetanus booster?Have you completed the series of three Hepatitis B injections?.YesNoList all medications you are currently taking:Previous EmploymentEmployerJob TitleDates EmployedProvider notes:Exposure historyPlease DESCRIBE any of the following exposures that may have occurred in the course of previous or current employment, or as a result of ongoing hobbies:Asphalt Roofing MaterialsConcrete ProductsPorcelain EnamelingDental LabFoundriesJewelryMakingCut StonePotteryReady-mix ConcreteRailroadsShipyardsStructural Clay ProductsSupport for Gas/Oil OperationsMinnesota Occupational HealthSt. PaulEaganBlainemohonline.com5Form Update 5/22/2018
Tuberculosis Testing DocumentationINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESPatient information:EMPLOYEE TO FILL OUT1. Have you ever had a previous Mantoux test?YesNo2. What were the results?PositiveNegative3. Were you ever treated for TB?YesNoIf Yes, when?If Yes, when?Employee/Applicant signature: Date: /MonthDay/YearNURSE/MA TO FILL OUTEmployee receiving:TB History Questionnaire2-Step Mantoux (baseline)1-Step Mantoux (annual)2-Step TST Administration# 1 Date:Time:Lot:QuantiferonTST ReadingLocation:Given By:Date:Time:Result (mm)Read by:Location:Given By:Date:Time:Result (mm)Read by:Exp:# 2 Date:Time:Lot:Exp:QUANTIFERON TB Blood TestName of TB blood testQuantiferon TB TestDate of blood drawRESULTSInterpretation of ox LaboratoriesMinnesota Occupational HealthSt. PaulEaganBlainemohonline.com6Form Update 5/22/2018
TuberculosisTuberculosis HistoryHistory QuestionnaireQuestionnaireTuberculosisHistory QuestionnaireTuberculosisTuberculosis HistoryHistory QuestionnaireQuestionnairePatientPatient information:information:INTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESINTEGRATED, COMPREHENSIVE OCCUPATIONAL HEALTH SERVICESPatientinformation:PatientPatient information:information:EarlyEarly DetectionDetection ofof TuberculosisTuberculosisThisquestionnaireThis questionnaire givesgives guidanceguidance inin identifyingidentifying individualsindividuals withwith suspectedsuspected oror confirmedconfirmed TBTB soso thatthat thethe appropriateappropriate controlscontrols cancan bebe promptlypromptly urknowledge.Early Detection of TuberculosisEarlyDetectionof givesTuberculosis in identifying individuals with suspected or confirmed TB so that the appropriate controls can be promptly initiated.TB(PartThisquestionnaireTB HistoryHistory(Part 1)1)gives guidanceThisquestionnaireguidance in identifying individuals with suspected or confirmed TB so that the appropriate controls can be promptly tifyingindividuals withsuspectedtheor confirmedTB so that the appropriate Yescontrols canNobe promptlyinitiated.1.Haveyoueverhadaa n’t knowknowComplete the questions inin partspartsTB1-3.Pleaseanswer thesethese questionsquestions toto the bestbest ofof youryour knowledge.knowledge.Completethequestionsinparts 1-3.Pleaseanswerthese questions to the best of your normalChestX-ray?.YesNoDon’tknowTB History (Part tknow1. Have you ever had a positive TB Skin Test?.YesNoDon’t ��tknow abnormalChestX-ray?.YesNoDon’tknowIf yes,was positive?YesNoDon’t knowknow2. Haveyouwereeveryouhadtoldan itabnormalChest.X-ray? .YesNoDon’t2.Have youyou recentlyever hadanabnormalChestX-ray?Tuberculosis?.YesNoDon’t �tknow3. Have you recently had the mucus you cough up tested for TB?.YesNoDon’t know3. Haveyourecentlyhaditthemucusyou cough up tested for TB?.YesNoDon’t tive?.YesNoDon’t Ifyes,howlongago?. If yes, were you told it was positive?.YesNoDon’t know HaveIf yes,wereyoutoldtreatedit waspositive?.YesNoDon’t fectious.NoDon’t5. HaveHave youyou everever beenbeen toldtreatedfor InfectiousInfectious TB?TB?. YesYesNoDon’t Infectious Tuberculosis?Tuberculosis?.YesNoDon’t4. Haveyoueverbeentold you have(checkInfectiousTuberculosis? .YesNoDon’tIfyes,howmanymedications?one).122 knowIfyes,howlongago?. Ifyes,howmanymedications?(checkone).122 If yes, how long ago?. esNoDon’tAre youstill takingtakingTB medicine?.medicine?.YesNo5. HaveHaveyou evereverbeen treatedtreatedwith medicationmedicationfor InfectiousInfectious TB?TB? .YesNoDon’t knowknow5. B?.YesNoDon’t eckone).122 youtakeall themedicine untilthe one).health care professional said you were done?. 1Yes IfDidyes,howmanymedications?(check2No2 AreIf yes,howmanymedications?(check contactone).122 gmedicine?.No6. DoDoyoulivewith/haveyoubeen inin closeclose contact withwith someonesomeone whowho waswas recentlyrecently diagnoseddiagnosed withwith TB?TB? . YesYesNoDon’t knowknowAreyoustilltaking TBTBmedicine?.YesNo Part2) d you take all the medicine until the health care professional said you were done?.YesNo DoDidyoutakea allthe medicineuntilthehealthcareprofessionalsaid youwere .incontactsomeonewhoYesNoDon’t1. DoDo youyou livehavewith/havea coughcough youthat beenhas livewith/haveyoubeenin closeclosecontactwithsomeonewho waswas recentlyrecently diagnoseddiagnosed withwith TB?TB? .YesNoDon’t ��t .Doyoucoughupbloodormucus?.YesNoCurrent Symptoms (Part nYesNo3. DoHavelostaa youryourappetite?YesNo1.Doyouyouhavecoughthat hashasAren’tlastedhungry?longer .than threethree oucoughupbloodormucus?.YesNo4. DoHavelost weight(morethan 10.lbs) in the last two months without trying to? . YesYesNo2.youyoucoughup bloodor mucus?No2.Do youcoughup bloodor .youlostyourappetite?Aren’t.No5. HaveDo youhave(needto hungry?change bedclothesbedclothesbecause theythey areare wet)?.wet)? . YesYesNo3.Haveyoulostnightyour pCurrentPatientStatus(Part3)6. eFeverChillsChestPain4. Have you lost weight (more than 10 lbs) in the last two months without trying to? .YesNo4.Haveyoulostnightweight(morethan to10 lbs).in bedclothesthe last two months withouttrying to? . aseexplain:5.Doyoucurrentlyhavenightsweats(needto changechangebedclothes becausebecause theythey areare gebedclothesbecausetheyarewet)?.YesNo t3)If yes, listhereMantouxStep1 CurrentPatient Status (Part 3)MantouxStep 1 CurrentPatient Status lytakinganyYesNoAreyoucurrentlypregnant?.YesNoAre you currently taking any medications?medications? ployee/Applicantsignature:Date: f yes, list hereMonth / Day / Year Ifyes,listhereMonthDay No YearAreyoucurrentlypregnant?.YesAre you currently pregnant?.Nopregnant?. YesAreyou currentlypregnant?.Yes TOUxTEST(IfStep2isrequired)Employee/Applicant signature: Date: // //Employee/Applicantsignature:Date:Month /Day /YearMantouxMonthDayYearMantoux StepStep 22 CurrentCurrent PatientPatient yOUR2NDMANTOUxTEST(IfStep2isrequired)Are you currentlytakingqUESTIONSany medications?.NoANSwERTHE BELOwAT THETIME Of yOUR 2ND MANTOUx TEST (If Step 2 is required) YesANSwERTHEBELOwqUESTIONSAT THE TIME Of yOUR 2ND MANTOUx TEST (If Step 2 is required) IfhereMantouxStep2PatientIf yes,yes, listlisthereMantouxStep2 CurrentCu
Silica Respirator Questionnaire To the employer: Answers to questions in Section 1, and to question 9 in Section 2 of Part A, do not require a medical examination. However, certain responses, or patterns of response, may lead the reviewer to request further information, or a medical examination,