Transcription
CASE REPORTJ Neurosurg Pediatr 21:421–427, 2018Treatment of medically refractory seizures withresponsive neurostimulation: 2 pediatric casesMalgosia A. Kokoszka, PhD,1 Fedor Panov, MD,1 Maite La Vega-Talbott, MD,2Patricia E. McGoldrick, NP, MSN, MPA,2 Steven M. Wolf, MD,2 and Saadi Ghatan, MD1Departments of 1Neurosurgery and 2Neurology, Mount Sinai Health System, New York, New YorkThe responsive neurostimulation (RNS) system, an adjunctive treatment for pharmacoresistant partial-onset seizureswith 1 or 2 foci, has been available to patients aged 18 years or older since the device’s FDA approval in 2013. Herein,the authors describe their off-label application of this technology in 2 pediatric patients and the consequent therapeutic benefit without surgical complications or treatment side effects. A 14-year-old nonambulatory, nonverbal malewith severe developmental delay was considered for RNS therapy for medically and surgically refractory epilepsy withbilateral seizure onsets in the setting of a normal radiological examination and a known neuropathological diagnosis oftype I cortical dysplasia. The RNS system was implanted with strip electrodes placed on the left lateral frontal and rightlateral temporal neocortex. At 19 months’ follow-up, cortical stimulation resulted in sustained reduction in both seizurefrequency—3 seizures per day down from 15 to 30 per day—and seizure severity. The patient subsequently underwenta trial of corticothalamic stimulation with a right temporal cortical strip and a left thalamic depth electrode, which resultedin a further 50% reduction in seizure frequency. In a second case, a 9-year-old right-handed female with radiologicalevidence of a small watershed infarct on the left and medically refractory seizures was referred for presurgical evaluation. Invasive monitoring revealed an unresectable seizure focus in the eloquent cortex of the left posterior frontal andparietal lobes. The RNS device was implanted with cortical leads placed at the putative seizure focus. At 21 monthsafter surgery, the patient had been seizure free for 4 months, following a 17-month period in which the seizure frequencyhad decreased from 12 per month to 2 per month, with associated functional and behavioral improvement. The authors’results suggest that RNS may be a palliative option for children with intractable seizures whose condition warrants offlabel use of the surgical device. The improved therapeutic effect noted with time and sustained RNS treatment points toa possible neuromodulatory PEDS17353KEY WORDS responsive neurostimulation; RNS; children; epilepsy; surgical failure; neuromodulationThe responsive neurostimulation (RNS) system(NeuroPace), an FDA-approved adjunctive treatment for adults with medically intractable partialonset seizures arising from 1 or 2 foci,10,17 is not yet approved for children with medically refractory epilepsy(MRE). The device consists of a surgically implanted cranial neurostimulator that is connected to 2 cortical and/ordepth leads containing 4 electrodes each that are placedat the putative seizure focus (foci). The neurostimulatorcontinuously senses electrographic activity and is programmed to deliver electrical stimuli intended to interruptepileptic events. Typical clinical applications include treatment of bilateral temporal epilepsy8 and seizures that arisefrom eloquent cortical regions.12One in 100 children suffer from epilepsy,24 and 30%of cases are medically refractory.14,15 Extratemporal, nonlesional, and multifocal epilepsies, common in childrenwho may be considered for epilepsy surgery, are associated with lower success rates following standard surgicaltechniques, when success is measured by a reduction inseizures and the absence of surgically related neurocognitive deficits.1,5 When the epileptogenic focus or zoneABBREVIATIONS AED antiepileptic drug; DBS deep brain stimulation; ECoG electrocorticography; EEG electroencephalography; FCD focal cortical dysplasia;MRE medically refractory epilepsy; MST multiple subpial transection; RNS responsive neurostimulation; VNS vagus nerve stimulation.SUBMITTED June 23, 2017. ACCEPTED October 17, 2017.INCLUDE WHEN CITING Published online February 2, 2018; DOI: 10.3171/2017.10.PEDS17353. AANS 2018, except where prohibited by US copyright lawJ Neurosurg Pediatr Volume 21 April 2018421Unauthenticated Downloaded 06/20/22 03:38 PM UTC
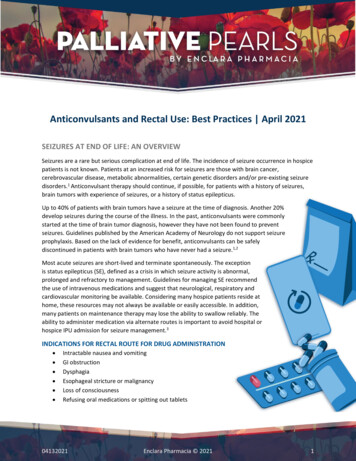
M. A. Kokoszka et al.incorporates functional regions, options such as multiplesubpial transections (MSTs) or vagus nerve stimulation(VNS) have not proven as effective as resection.2,25Treatment with the RNS system is effective in reducing seizures emanating from eloquent cortical regions,12has similar efficacy in mesial temporal and extratemporalepilepsies,10 and has the potential to treat multifocal epilepsies, particularly germane to the pediatric population.We describe our early and favorable experience with theoff-label application of this technology in 2 pediatric patients with MRE.Case ReportsCase 1: Medically and Surgically Refractory EpilepsyHistoryA 14-year-old nonverbal boy with severe developmental delay and a history of clinically significant aberrantbehaviors exacerbated by his epilepsy initially presentedwith West syndrome at 4 months of age and went on todevelop medically intractable focal seizures, which localized to his right frontal lobe. His MRI findings wereunremarkable, and genetic testing failed to disclose anyknown predisposition to epilepsy. At 5 years of age, at another institution, he underwent single-stage right frontallobectomy yielding a neuropathological diagnosis of typeI focal cortical dysplasia (FCD). At the age of 7, he presented to our center with worsening developmental delayand MRE with a dominant atonic semiology. Further surgical interventions included a complete corpus callosotomy, which alleviated the atonic seizures but gave way torapidly generalizing seizures and a continued functionalbehavioral decline with little improvement after palliativeVNS device placement. Periodic postcallosotomy scalpelectroencephalography (EEG) monitoring demonstrateda predominance of left temporal and posterior quadrantseizures. In light of the suggestion of laterality, as seen ina subset of patients after callosotomy,20 invasive monitoring with bilateral strip electrodes was performed to moredefinitively assess laterality, and this revealed both leftand right-sided interictal epileptiform abnormalities withall clinical events originating on the left. Given the patient’s progressive decline in development and behavior,as well as the focal seizure onsets from the left temporal lobe and posterior quadrant confirmed by subsequentmonitoring with grid and strip electrodes, a palliativetemporal lobectomy and posterior quadrantectomy wasundertaken. Neuropathological analysis revealed focalchronic inflammation and diffuse abnormalities suggestive of type Ic FCD. The patient continued to have seizures, now localizing to the right temporal and left frontallobe.Surgical Plan and Preoperative ConsiderationsBecause of the patient’s history of ablative surgical failure, multifocal and mutable MRE, and neuropathologicaldiagnosis of possible type I cortical dysplasia, more resective surgery was not considered, and team consensus wasreached for the off-label use of the RNS system as the onlynonresective therapeutic approach that had not been triedin this patient. Target zones for 2 strip electrodes were422FIG. 1. Case 1. Placement of the RNS system. A: Coronal MR imageof the patient’s brain preimplantation. B: Postoperative scan showingthe RNS device with strip electrodes placed on the left lateral frontaland right lateral temporal neocortex and depth electrodes in the anteriorthalamic nuclei bilaterally.identified based on a cumulative analysis of the patient’sinvasive and noninvasive EEG findings from a period ofmore than 2 years, starting with the results of monitoringwith bilateral strips, which narrowed down the patient’smost highly epileptogenic foci to the left lateral frontaland right lateral temporal neocortex. In addition, the anterior thalamic nuclei bilaterally were agreed on as potentialtargets for stimulation with depth electrodes since somesuccess had been seen with deep brain stimulation (DBS)for epilepsy in clinical trials.7,26Insurance approval was navigated through appeal andsurgeon-to–insurance plan medical director discussions ofthe benefit of RNS in the adult population and the lack of aviable alternative for this pediatric patient. There were noadditional out-of-pocket expenses required of the familyunder their private insurance plan.OperationDepth electrodes were placed in the anterior thalamicnuclei bilaterally, with strip electrodes placed on the leftlateral frontal and right lateral temporal neocortex (Fig.1). Given the patient’s distorted anatomy from prior craniotomies, preoperative volumetric MRI with and without contrast and CT were performed, and an anterolateraltrajectory to the anterior thalamic nuclei was applied using Leksell frame-based navigation (Elekta InstrumentsInc.) and FrameLink software (Medtronic Inc.). Burrholes were placed over the left middle frontal gyrus andthe right superior temporal gyrus for the strip electrodes,without navigation guidance. The current RNS system hasthe capacity for 2 leads to be connected to the neurostimulator, and the neocortical strips were initially connected tothe device. These lobar strip electrodes were chosen giventheir involvement in the patient’s preoperative ictal andinterictal EEG signatures. Intraoperative electrocorticography (ECoG) demonstrated frequent spike activity fromboth strip electrodes but a characteristic low-amplitudereading from the thalamic depth electrodes.Postoperative CourseEarly postoperative ECoG data indicated that as thestimulation settings increased over 3 months from acharge density of 0.5 to 1.3 mC/cm2, there was a drop inJ Neurosurg Pediatr Volume 21 April 2018Unauthenticated Downloaded 06/20/22 03:38 PM UTC
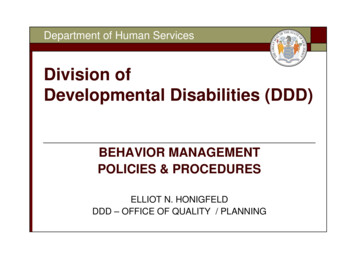
M. A. Kokoszka et al.FIG. 2. Case 1. Initial response to stimulation. A and B: In each plot, the top 2 channels represent the frontal cortical strip andthe bottom 2 channels represent the temporal strip. The color spectrograms (middle) reflect the power of the ECoG signal at givenfrequencies over time, with light blue/green indicating little to no power and darker red indicating high power in that frequency atthat time. The lowest plot is an enlargement of a section in the upper plot, with the vertical line across the channel second from thetop indicating episode detection and the continuous vertical lines across all channels representing the device delivering stimulation. The early-stimulation ECoG of a morning episode shows a seizure lasting 20 seconds. The ECoG of a morning episodeafter 8 months of stimulation shows a shortened episode (approximately 12 seconds) with decreased severity. C: Graph showinga reduction in daily events and in the number of long episodes ( 10 seconds) per month, indicating a response to an increase instimulation settings.the daily rate of detections of abnormal electrographicpatterns, suggesting that the patient responded favorablyto higher stimulation settings. Stimulation also appearedto shorten the seizures (Fig. 2). At 19 months’ followup, the patient had received an average of approximately2300 stimulations per day (alternating bursts of 100- and200-Hz stimulations were delivered: 100 Hz at 1.3 mC/cm2 and 2.5 mA; 200 Hz at 2.0 mC/cm2 and 4.0 mA; allwith a 160-msec pulse width and 100-msec burst duration), and he had experienced a significant decrease in sei-zures, from a preoperative baseline of 15–30 seizures perday down to approximately 3 seizures per day. The family also reported decreased seizure severity with shorterrecovery times, especially during daily morning events,whereas prior to the implant the patient’s semiology involved hypertonicity of the entire body, severe facial flushing, and sialorrhea and foaming from the mouth, which allresolved with RNS therapy. The patient also experiencedrelated improvements in behavior, attentiveness, and levelof engagement, as reported by the school.J Neurosurg Pediatr Volume 21 April 2018423Unauthenticated Downloaded 06/20/22 03:38 PM UTC
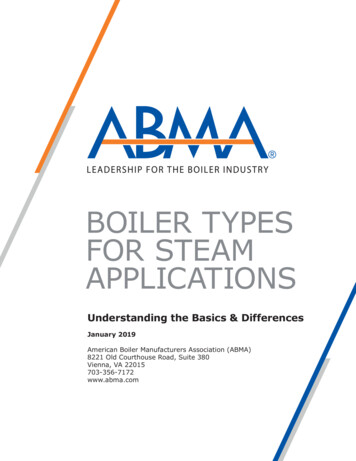
M. A. Kokoszka et al.FIG. 3. Case 2. Placement of the RNS system. A: Preoperative axial MR image demonstrating evidence of a small watershed infarct on the left. B: Intraoperative photograph showing craniotomy and cortical lead placement over the putative epileptogenic zone.Leads second and fourth from the top were connected to the device. C: Postoperative scan showing the RNS system in place.Corticothalamic Stimulation TrialThe patient’s daily medication regimen included 4 antiepileptic drugs (AEDs) at stable preimplantation doses,and his parents were concerned about the medication burden and the short- and long-term effects on the patient’shealth. This prompted discussions of a corticothalamicstimulation trial in which the cortical strip would serve asthe site of epileptogenic pattern detection and both surfaceand thalamic electrodes would deliver responsive stimulation. To determine which thalamic electrode to activate,we used telemetry to turn off and sequentially test thestrip electrode that provided the optimal effect on seizurefrequency and severity. We saw increased seizure frequency and severity during periods of diagnostic left unilateralstimulation, so a clinical plan was devised to disconnectthe left frontal strip electrode, connect the left thalamicdepth electrode, and leave the right temporal strip electrode in place for cortical detection and stimulation. At thetime of electrode revision, the battery was also replaced.After 1 month of corticothalamic stimulation with thevoltage set to 0.5 mA and a 0.3-mC/cm2 charge density,the patient had a preliminary 50% reduction in seizurefrequency compared with unilateral cortical stimulationand is set to continue thalamic stimulation with increasingsettings.Case 2: Eloquent CortexHistoryA 9-year-old right-handed girl suffering from MREand comorbid panhypopituitarism was referred for presurgical evaluation. She had mild baseline right hemiparesiswith MRI evidence of a small watershed infarct in the leftparietal lobe (Fig. 3). Her seizures had started when she424was 18 months old and became intractable at age 5 years.The parents described a progressively worsening seizureand medication burden as well as constant fatigue, frequentfalling, slow academic progress, and impaired speech thatat times could only be understood by her family. ScalpEEG suggested her seizures emanated from the left temporal lobe, away from the MRI-demonstrated lesion.Invasive monitoring with grid and strip electrodes identified an epileptogenic zone in the left posterior frontal andparietal lobes that co-localized to her language and Rolandic cortical regions. Extraoperative stimulation mappingat 3 mA using an Ojemann cortical stimulator (IntegraLifeSciences) triggered significant afterdischarges andelectroclinical seizures mimicking the patient’s semiology in these regions, which were suppressed with higheramplitude stimulation, suggesting the potential for a favorable therapeutic response to direct cortical stimulation.Surgical Plan and Preoperative ConsiderationsBecause of our center’s long-standing experience withsubdural recordings guiding a lesional approach,9 RNSwas not initially planned. However, given the patient’s extraoperative recordings and response to stimulation during brain mapping, we presented the option of RNS to thefamily rather than an ablative procedure such as MST and/or incomplete resection, which would statistically yieldsuboptimal results and be irreversible.As in case 1, insurance approval was granted after surgeon-to–insurance plan medical director discussions, aswell as the additional information that this system had already been successfully implanted in another child at ourcenter. There were no additional out-of-pocket expenses tothe family, who also had a private insurance plan.J Neurosurg Pediatr Volume 21 April 2018Unauthenticated Downloaded 06/20/22 03:38 PM UTC
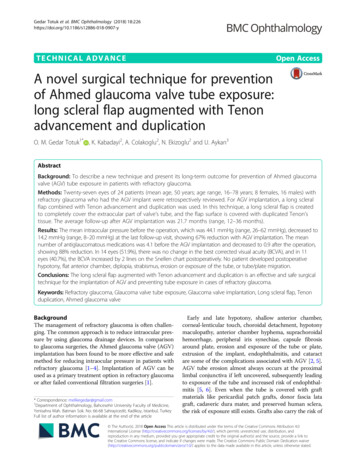
M. A. Kokoszka et al.OperationTwo months after explantation of grid and strip electrodes, we proceeded with the RNS procedure given concerns regarding the bacterial colonization that could contaminate and potentially infect a more permanent implant.We based this decision on our prior practice of waiting 4–8weeks after bilateral subdural strip electrode placement tomove forward with a unilateral grid study. An RNS devicewas placed with 4 cortical strips in the angular and supramarginal gyrus regions (Fig. 3). Intraoperative ECoGdemonstrated rhythmic epileptiform discharges from themost rostral and caudally placed leads, which were connected to the device.Postoperative CourseThe stimulation parameters established for this patientduring the first 5 months resulted in an approximately80% reduction in her seizures, with continued improvement over the next 3 months without a change in settings(200-Hz stimulation was delivered between the 2 leadsat 2.0 mA and 1.0 mC/cm2, pulse width of 160 msec, andburst duration of 100 msec; Fig. 4). At 15 months after surgery, the settings had been gradually adjusted so that stimulation was being delivered between the contacts withineach lead at 2.5 mA and 2.5 mC/cm2, with no changes tothe pulse width or burst duration. The detection settingswere also changed, and the patient received an average ofapproximately 3300 stimulations per day. This numberdecreased over the next 2 months to approximately 570stimulations per day without further setting changes.At the 17-month follow-up, the patient’s seizure frequency had decreased from 12 per month to about 2 permonth, and the number of AEDs was reduced to 3 versus the 6 when she was first referred to our center. Herseizures were milder, she no longer fell, and she becamemore aware and talkative, with improved attention in class.Her school attendance also improved: prior to treatmentwith the RNS system, she would typically miss 1 day perweek, either because of a seizure at school or because of adifficult postictal recovery after a seizure at home. Afterstarting treatment with RNS, she did not miss any schooldays because of epilepsy.At the 21-month follow-up, the patient had been seizurefree for 4 months. Despite lead placement in functionalareas of the cortex, the patient is unaware of stimulation,similar to what has been established in the adult population.3,12DiscussionWith the off-label use of RNS, we have demonstratedearly therapeutic benefit from this device in children,without associated adverse events or surgical complications. Improvements in seizure control and behavior, patient tolerability, and parental satisfaction bring optimismthat application of the RNS system can be expanded toyounger populations, in which it has the potential to overcome some of the current obstacles to successful controlof MRE and may eventually demonstrate even strongerindications for use. While formal availability of this technology to the pediatric patient is dependent on the manu-FIG. 4. Case 2. Possible neuromodulatory effect of RNS. Graph showing the number of electrographic events decreasing over time, without achange in device settings.facturer obtaining FDA approval, we hope that this reportcan serve as a reference in informal discussions of potential off-label applications with health care providers, parents, and insurers.Impediments to early epilepsy surgery in children aremultifactorial and result in the underutilization of thistherapy.21 Practitioner reluctance to recommend6,23 andparental unwillingness to accept22 epilepsy surgery canbe tied to, among other factors, the irreversibility in decision making: operations that involve ablation, resection,or disconnection early in life and the risks that they entailcannot be undone. Seemingly favorable and “definitive”disconnections or resections can give way to subsequentsecondary seizure onsets at distant sites, presumably dueto an underlying genetic substrate and the poorly understood nature of epilepsy networks in the immature brain,and can account for many surgical failures.13 Treatmentwith the RNS system is reversible and modulatory ratherthan ablative; it can be modified with time and maturationof the brain, as well as technological advances. Becauseof its capacity for chronic recording of brain activity, itsuse can lead to an improved ability to localize seizurefoci and greater confidence in resective treatment planning and can provide a means of longer-term study ofepileptogenic networks in an immature, plastic system, inaddition to its therapeutic benefit. These considerations,when brought to the attention of the parents in each of ourcases, made for ready acceptance of the proposed surgical plan.Direct stimulation of the epileptogenic zone in response to preprogrammed patterns to suppress seizures atthe onset is the principle of RNS, but improvements withtime in response to sustained RNS therapy are also possible, similar to what has been observed with VNS therapy18and with DBS trials for epilepsy.7,26 The RNS pivotal trialresults revealed improved seizure control over time,10 and,more recently, mean 7-year follow-up data have showncontinually elevating rates of seizure reduction.3 This effect may be due to plasticity and what could be termed“circuit training,” akin to what has been seen in the dystonia literature with neuromodulation,11 and this sort ofneuromodulatory learning may be better suited to the lessmature epileptic networks encountered in children.28By modulating epileptogenic zones in the patient incase 1, we have been able to reduce the number of dailyevents and shorten the length of his seizures and their seJ Neurosurg Pediatr Volume 21 April 2018425Unauthenticated Downloaded 06/20/22 03:38 PM UTC
M. A. Kokoszka et al.verity (Fig. 2). At 24 months post–RNS device placement,direct brain stimulation has proved to be more beneficialthan any other surgical intervention. The patient’s knownpathological diagnosis of type I FCD and the history ofseizure onsets that had evolved over time from the rightto the left hemisphere are predictive of failure via resection or disconnection, but palliative resective surgery wasthe only surgical option we could offer this family beforethe RNS system became available. To our knowledge, theefficacy of the RNS system has not been systematicallystudied in patients with FCD, but in our first case, RNS appears capable of influencing the patient’s chaotic networkpresumed to be associated with diffuse type I FCD. Earlyresults of corticothalamic stimulation in this case lend credence to the utility of influencing the patient’s epileptogenic network rather than a putative focus.In our second case, in which seizures emanated fromthe eloquent regions of speech and sensorimotor corticesin the dominant hemisphere, prior options would have involved palliative MSTs or VNS, with the success rate foreach being better than further medical therapy alone2,25but still promising less improvement than that observedin similar cases in adults with RNS.12 Our patient’s morethan 80% decrease in seizures is better than the median70% seizure reduction reported in adults with frontal andparietal functional cortex foci,12 and the capacity for continued improvement over time at the same stimulation settings and the recent period of seizure freedom predict thepotential for ongoing efficacy.Only one of our patients has had a considerable seizurefree period, but in both of our cases, the therapeutic effectof RNS and the associated benefits are already evident,even as stimulation parameters are still being adjusted.Significant quality-of-life improvements have been notedin adults treated with RNS,16 in whom changes in seizureworry, health discouragement, and attention/concentrationwere the top 3 benefits—and such changes can be morepronounced in children. A major component of seizureworry for parents is the sudden unexpected death in epilepsy (SUDEP) risk,19 and the latest data demonstrate asignificantly lower risk of SUDEP in adults receiving RNSthan in patients with MRE and no surgical intervention.4In pediatric surgical candidates with MRE, in which therisk of death can be 100 times greater than that in children newly diagnosed with epilepsy,27 the use of this device should provide substantial solace to parents. Improvements in attention and concentration, reflected in both ofour patients according to parental, scholastic, and caregiver reports, would be expected to have a significant impacton socialization, relationships, education, and vocationalpotential in pediatric patients.We have had no adverse outcomes in either of our patients, and the latest data from the RNS pivotal trial donot indicate any increased long-term risk. Adults treatedwith the RNS system have a 3% risk of implant site infection with the neurostimulator implant procedure, a ratethat does not increase with subsequent neurostimulator replacements,29 such that over the lifespan of a child, whenmore interventions will be necessary given the duration oftreatment, the risk of infection should remain acceptable.Anatomically, the device is implanted in a ferrule within426the skull where it sits flush with the skull surface, therebyobviating the risk of skin erosion that can be associatedwith wires and generators placed in children. Placementof the device in the patient’s cranium—behind the hairlineand without any visible protuberance, such as wires in theneck or a pulse generator in the body—reduces concernsover stigma in understandably self-conscious children,adolescents, and parents. Thus, we see no special concernsin placing this device in the pediatric population as longas the RNS device is placed flush with the skull surface, toavoid the risk of skin erosion.In keeping with the long-term results in adults that showcontinued improvement with time,3,10 we believe that theRNS device holds significant promise for the treatment ofepilepsy in the immature brain. By employing a modulatory rather than a destructive surgical modality for seizurecontrol in children, together with ECoG data acquisitionthat can guide further medical and surgical management,epilepsy surgery can reach a broader population, as itstands to gain wider acceptance from parents and referring practitioners.References1. Ansari SF, Maher CO, Tubbs RS, Terry CL, Cohen-GadolAA: Surgery for extratemporal nonlesional epilepsy in children: a meta-analysis. Childs Nerv Syst 26:945–951, 20102. Benifla M, Otsubo H, Ochi A, Snead OC III, Rutka JT: Multiple subpial transections in pediatric epilepsy: indicationsand outcomes. Childs Nerv Syst 22:992–998, 20063. Bergey GK, Morrell MJ, Mizrahi EM, Goldman A, King-Stephens D, Nair D, et al: Long-term treatment with responsivebrain stimulation in adults with refractory partial seizures.Neurology 84:810–817, 20154. Devinsky OKR, Duckrow RB, Fountain NB, Gwinn RP,Leiphart JW, Murro AM, et al: SUDEP rate in patients withmedically intractable partial onset seizures treated withbrain responsive stimulation, in American Epilepsy SocietyAnnual Meeting, 2016 (Abstract) (https://www.aesnet.org/meetings events/annual meeting abstracts/view/191742)[Accessed December 19, 2017]5. Englot DJ, Breshears JD, Sun PP, Chang EF, Auguste KI:Seizure outcomes after resective surgery for extra-temporallobe epilepsy in pediatric patients. J Neurosurg Pediatr12:126–133, 20136. Erba G, Moja L, Beghi E, Messina P, Pupillo E: Barrierstoward epilepsy surgery. A survey among practicing neurologists. Epilepsia 53:35–43, 20127. Fisher R, Salanova V, Witt T, Worth R, Henry T, Gross R, etal: Electrical stimulation of the anterior nucleus of thalamusfor treatment of refractory epilepsy. Epilepsia 51:899–908,20108. Geller EB, Skarpaas TL, Gross RE, Goodman RR, BarkleyGL, Bazil CW, et al: Brain-responsive neurostimulation inpatients with medically intractable mesial temporal lobe epilepsy. Epilepsia 58:994–1004, 20179. Ghatan S, McGoldrick P, Palmese C, La Vega-Talbott M,Kang H, Kokoszka MA, et al: Surgical management of medically refractory epilepsy due to early childhood stroke. JNeurosurg Pediatr 14:58–67, 201410. Heck CN, King-Stephens D, Massey AD, Nair DR, JobstBC, Barkley GL, et al: Two-year seizure reduction in adultswith medically intractable partial onset epilepsy treated withresponsive neurostimulation: final results of the RNS SystemPivotal trial. Epilepsia 55:432–441, 201411. Isaias IU, Alterman RL, Tagliati M: Deep brain stimulationJ Neurosurg Pediatr Volume 21 April 2018Unauthenticated Downloaded 06/20/22 03:38 PM UTC
M. A. Kokoszka et al.12.13.14.15.16.17.18.19.20.21.22.23.24.for primary generalized dystonia: long-term outcomes. ArchNeurol 66:465–470, 2009Jobst BC, Kapur R, Barkley GL, Bazil CW, Berg MJ, BergeyGK, et al: Brain-responsive neurostimulation in patients withmedically intractable seizures arising from eloquent andother neocortical areas. Epilepsia 58:1005–1014, 2017Kokoszka MA, McGoldrick PE, La Vega-Talbott M, RaynesH, Palmese CA, Wolf SM, et al: Epilepsy surgery in patientswith autism. J Neurosurg Pediatr 19:196–207, 2016Kwan P, Arzimanoglou A, Berg AT, Brodie MJ, Allen HauserW, Mathern G, et al: Definition of drug resistant epilepsy:consensus proposal by the ad hoc Task Force of the ILAECommission on Therapeutic Strategies. Epilepsia 51:1069–1077, 2010Kwan P, Brodie MJ: Early identification of refractory epilepsy. N Engl J Med 342:314–319, 2000Meador KJ, Kapur R, Loring DW, Kanner AM, Morrell MJ:Quality of life and mood in patients with medically intractable epilepsy treated with targeted responsive neurostimulation. Epilepsy Behav 45:242–247, 2015Morrell MJ: Responsive cortical stimulation for the treatment of medically intractable partial epil
sented to our center with worsening developmental delay and MRE with a dominant atonic semiology. Further sur - gical interventions included a complete corpus calloso-tomy, which alleviated the atonic seizures but gave way to rapidly generalizing seizures and a continued functional-behavioral decline with little improvement after palliative