Transcription
ORIGINAL ARTICLEClinical Outcomes of BRYAN Cervical Disc Arthroplasty:A Prospective, Randomized, Controlled, Multicenter TrialWith 24-month Follow-upRick C. Sasso, MD,* Joseph D. Smucker, MD,w Robert J. Hacker, MD,z and John G. Heller, MDyStudy Design/Setting: Prospective, randomized, 3-center, clinicaltrial.Objective: To prospectively compare the outcomes of cervicalarthroplasty with the BRYAN Cervical Disc Prosthesis (Medtronic Sofamor Danek, Inc, Memphis, TN) to anterior cervicaldiscectomy and fusion (ACDF).Summary of Background Data: Surgical treatment of cervicaldisc pathology commonly involves techniques that employdiscectomy and fusion (ACDF). This ‘‘gold-standard’’ technique has demonstrated good clinical and radiographic outcomes.Common adverse effects of this procedure are associated withthe adjacent level degeneration and bone-graft harvest. Severalinvestigators have independently reported successful short-termoutcomes with the BRYAN Cervical Disc Prosthesis. Inaddition, a significant body of knowledge has been collectedregarding the wear patterns and adjacent level effects of thisdevice in human and animal models.Methods: As part of an FDA IDE trial, 3 centers collectedprospective outcomes data on 115 patients randomized in a 1:1ratio to ACDF (Control group) or arthroplasty with theBRYAN Cervical Disc Prosthesis (Investigational group).Results: Demographic and surgical data were generally similarin the 2 populations. Outcomes data collected at routinepostoperative intervals for 24 months demonstrated that theInvestigational group had statistically significant (P 0.05)improvements as assessed by the Neck Disability Index, theNeck Pain Score, and SF-36 Physical component scores. Theimprovement in the Mental Component Subscore values forthe BRYAN and control groups was equivalent at 24 months(P 0.055). Arm pain relief was similar in both groups(P 0.152). During the course of the 2-year follow-up,4 patients in the Control group required surgical interventionReceived for publication April 26, 2006; accepted December 3, 2006.From the *Indiana Spine Group, Clinical Orthopaedic Surgery, IndianaUniversity School of Medicine, Indianapolis, IA; wDepartment ofOrthopaedic Surgery, The University of Iowa, Iowa City, IA;zOregon Neurosurgery Specialists, Eugene, OR; and yEmory SpineCenter, Department of Orthopaedic Surgery, Emory University,Atlanta, GA.Reprints: Joseph D. Smucker, MD, Department of Orthopaedics,The University of Iowa, 200 Hawkins Drive, 01017 JPP, Iowa City,IA 52242 (e-mail: joe@smuckermd.com).Copyright r 2007 by Lippincott Williams & WilkinsJ Spinal Disord Tech Volume 20, Number 7, October 2007and 3 patients in the Investigational group required ACDF foradjacent level disease.Conclusions: At 24 months, cervical arthroplasty with theBRYAN Cervical Disc Prosthesis compares favorably withACDF as defined by standard outcomes scores.Key Words: Bryan Cervical Disc, cervical arthroplasty, randomized, prospective, cervical fusion, outcomes(J Spinal Disord Tech 2007;20:481–491)The cervical discs function in load bearing and motiontransfer. Much is known about the macro-biologyof the intervertebral disc. Disc degeneration and thesubsequent manifestations that ensue in the cervical spineare also well documented. For many years, the surgicaltreatment for pathology in the cervical intervertebral dischas been limited to procedures that remove pathologicdisc material and address the bony and neurologicpathology in the region of the excised disc. Anteriorcervical discectomy and fusion (ACDF) is a provenintervention for patients with radiculopathy and myelopathy.1 Because of the limitations specific to thisprocedure, investigators have developed alternatives tofusion that attempt to address the kinematic andbiomechanical issues inherent to fusions.2–7Reoperation rates for adjacent segment degeneration have been documented at a rate of 2.9% of patientsper annum, and 25.6% of patients undergoing cervicalfusion will have surgery for recurrent symptoms within 10years of the index fusion.8 Other reports have helped toshed light on the recurrence of neurologic symptoms anddegenerative changes adjacent to fused cervical levels.9,10Segments adjacent to a fusion have an increased range ofmotion and increased intradiscal pressures.11,12Pseudarthrosis is another complication encounteredwith anterior cervical fusion procedures. There is arelationship between the rate of pseudarthrosis and thenumber of levels fused. Brodke and Zdeblick13 reported a97% fusion rate in single-level ACDF, which decreasedto 83% with fusion at 3 levels. Bohlman et al1 reportedan 11% pseudarthrosis rate in single-level fusions thatincreased to 27% with multilevel fusions.Complications associated with autologous iliac crestharvest, traditionally used as a fusion graft in ACDF, are481
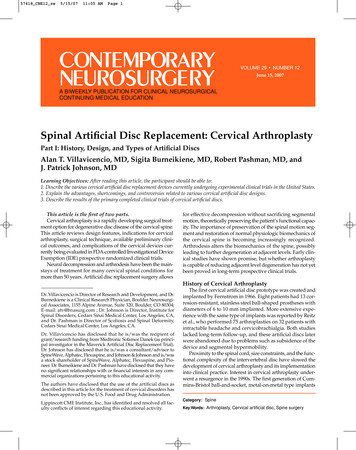
J Spinal Disord TechSasso et alalso well documented. Sandhu et al14 reported acomplication rate of 1% to 25% with such procedures.Complications such as acute and chronic pain, infection,meralgia paresthetica, and pelvic fracture are known tooccur at harvest donor sites.15,16Total intervertebral disc replacement (TDR) isdesigned to preserve motion, avoid limitations of fusion,and allow patients to quickly return to routine activities.The primary goals of the procedure in the cervical spineare to restore disc height and preserve segmental motionafter removing the source of nerve root or spinal cordcompression. A secondary intention is the preservation ofnormal motion at adjacent cervical levels, which may betheorized to retard later adjacent level degeneration. Itavoids the morbidity of bone-graft harvest.17,18 It alsoavoids complications such as pseudarthrosis, issuesattributed to anterior cervical plating, and cervicalimmobilization side effects.The BRYAN Cervical Disc Prosthesis (MedtronicSofamor Danek, Inc, Memphis, TN) is a 1-piece,biarticulating, metal-on-polymer, unconstrained devicewith a fully variable instantaneous axis of rotation that isnot dependent on supplemental fixation2,3 (Figs. 1, 2). Ithas a polyurethane sheath that is designed to containwear debris and prevent soft tissue ingrowth. Eachendplate is porous coated to promote bony ingrowthfor long-term device stability. Although initial clinical usecommenced in Europe during January 2006, the BRYANcervical disc replacement became the first such device toinitiate a clinical trial in the United States in May 2002.The purpose of this paper is to report a subset of datafrom 3 of the clinical investigative centers for the FDAIDE trial.MATERIALS AND METHODSPatientsOne hundred and fifteen patients were enrolled andfollowed prospectively at 3 centers involved in a multicenter, FDA IDE trial for the BRYAN Cervical DiscProsthesis. Patients with single-level, symptomatic, cervical radiculopathy or myelopathy refractory to nonoperative interventions were randomized in a 1:1 ratio to asingle-level ACDF with allograft and plate (Control Volume 20, Number 7, October 2007group) or single-level cervical arthroplasty with theBRYAN Cervical Disc Prosthesis (Investigational group).Preoperative imaging studies included plain radiographs,magnetic resonance imaging, and computed tomography.The latter was helpful in excluding significant spondylosisand facet joint arthrosis.SurgeryThe surgical technique was similar in both groupsto the point of interbody fusion/arthroplasty. A standardSmith-Robinson approach was made to expose thesymptomatic level. After appropriate exposure andlocalization of the disc, a discectomy was performed.After discectomy, a local decompression was accomplished via foraminotomies and resection of osteophytesand/or the posterior longitudinal ligament at the treatingsurgeon’s discretion.Endplate preparation for ACDF was completedwith a high-speed burr and an appropriately sizedCornerstone SR fibular allograft (Medtronic SofamorDanek, Inc, Memphis, TN) was placed in the preparedinterspace. All ACDF patients underwent anteriorcervical plating with the Atlantis Vision Cervical PlateSystem (Medtronic Sofamor Danek, Inc, Memphis, TN).Preparation of the endplates for arthroplasty wasaccomplished in the standard technique. The BRYANdisc milling technique creates 2 concave surfaces via amilling jig. Sizing of the BRYAN cervical disc wasdetermined with a combination of templates and preoperative radiographic studies including computed tomography.19 The center of the disc space was determinedintraoperatively by a jig that defines the uncovertebraljoints and finds the center. With knowledge of the centerof the disc space, a milling fixture was anchored to thevertebral bodies. This fixture controlled the cutting toolswhich mill the endplates to the exact geometry of thedevice endplates providing immediate stability (Fig. 3).19Insertion of the TDR was accomplished underlateral fluoroscopy to assure adequate depth. Beforeinserting the BRYAN disc, the implant was filled withsaline as an initial lubricant.19 The prosthesis was thenplaced into the milled interspace (Fig. 3). Before closureof the incision, appropriate placement of the TDR wasFIGURE 1. The BRYAN Cervical Disc Prosthesis(r Courtesy of Medtronic Sofamor Danek, Memphis, TN; with permission).31482r2007 Lippincott Williams & Wilkins
J Spinal Disord Tech Volume 20, Number 7, October 2007Multicenter BRYAN Disc StudyTABLE 1. Demographic InformationVariableFIGURE 2. The BRYAN Cervical Disc Prosthesis Design(r Courtesy of Medtronic Sofamor Danek, Memphis, TN;with permission).31confirmed with anteroposterior and lateral fluoroscopicimaging.Data CollectionPreoperative demographic data, surgical data, andoutcomes data were collected on all patients. Clinicaloutcome tools included: Neck Disability Index (NDI),Arm Pain Score (VAS), Neck Pain Score (VAS), andSF-36. Outcome assessments were made preoperativelyand at 6 weeks, 3 months, 6 months, 12 months, and24 months. Collected data were statistically analyzed andtabulated (Tables 1, 2).Radiographic angular motion at the target level wastracked on digital radiographs using quantitative motionanalysis software (QMA, Medical Metrics, Houston, TX)to calculate the functional spine unit motion parametersby 2 blinded, trained observers. The recorded values ofangulation at the treated levels are the absolute valueof extension minus flexion from the 2 readers’ measurements. These values were tabulated and statisticallyanalyzed as presented in Tables 7A and 7B.Age (y)Mean SDHeight (in)Mean SDWeight (lbs)Mean SDSex [N (%)]MaleFemaleRace [N (%)]WhiteBlackAsianHispanicOtherMarital status [N (%)]SingleMarriedDivorcedSeparatedWidowedEducation level [N (%)] High schoolHigh school High schoolTobacco used [N (%)]YesNoAlcohol used to relieveneck pain [N (%)]YesNoPreoperative workstatus [N (%)]Currently workingNot workingInvestigational(N 56)Control(N 59)P*42.5 7.846.1 7.80.01567.9 3.567.7 3.70.728173.6 42.6180.8 39.20.34330 (53.6)26 (46.4)32 (54.2)27 86 (10.7)13 (23.2)37 (66.1)8 (13.6)18 (30.5)33 (55.9)0.56212 (22.2)42 (77.8)10 (16.9)49 (83.1)0.6352 (3.7)52 (96.3)3 (5.1)56 (94.9)1.00041 (73.2)15 (26.8)42 (71.2)17 (28.8)0.838*For continuous variables, P values are from analysis of variance and forcategorical variables, they are from Fisher exact test.Statistical AnalysisStatistical analysis was performed using SAS (SASInstitute Inc, Cary, NC). For continuous variables,statistical analysis and P values were calculated byanalysis of variance and for categorical values a Fisherexact text was employed. A paired t test was used tocalculate the statistical significance of change from thepreoperative score in SF-36, NDI, Neck Pain, and ArmPain categories. It was also employed for the analysisof motion scores at the target level when change frompreoperative angulation was recorded.RESULTSDemographic and Surgical DataFIGURE 3. Endplate preparation and BRYAN TDR implantinsertion (r Courtesy of Medtronic Sofamor Danek, Memphis,TN; with permission).19r2007 Lippincott Williams & WilkinsOne hundred and fifteen patients were randomizedin a 1:1 ratio to either a BRYAN Cervical Disc (N 56)or an anterior cervical fusion with allograft and a plate(N 59). There were 30 males and 26 females in theBRYAN group and 32 males and 27 females in the fusiongroup. The average age was 42 years (BRYAN) and 46years (Control). No statistically significant differenceswere noted in the demographics of the Investigational and483
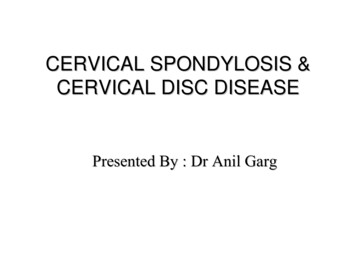
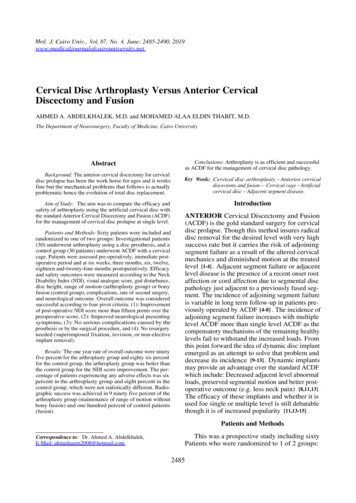
J Spinal Disord TechSasso et alTABLE 2. Surgical and Discharge DataVariableOperative time (h)Mean SDBlood loss (mL)Mean SDHospital stay (d)Mean SDTreatment levels [N (%)]C3-C4C4-C5C5-C6C6-C7External orthosis [N (%)]NoneSoft collarRigid collarHaloCervical braceOtherControl(N 59)P*1.7 0.51.1 0.4 0.00164.6 49.649.2 39.60.9 0.40.6 ative0.068 0.0016 wk0.5793 mo34210001(60.7)(37.5)(0.0)(0.0)(0.0)(1.8)Volume 20, Number 7, October 2007TABLE 3A. Summary of SF-36 Health Survey ScoresInvestigational(N 56)(1.8)(3.6)(48.2)(46.4) 5494001(8.5)(83.1)(6.8)(0.0)(0.0)(1.7) 0.0016 mo*For continuous variables, P values are from analysis of variance and forcategorical variables, they are from Fisher exact test.12 mocontrol populations with the exception of age (P 0.015)(Table 1).The average operative time for the Control groupwas 1.1 hours and the BRYAN group 1.7 hours(P 0.001). Average blood loss was similar. Averagehospital stay was 0.5 days (Control) and 1 day (BRYAN)(P 0.001). Additional surgical data are reported inTable 2.24 moVariablePCSNMean SDMCSNMean SDPCSNMean SDMCSNMean SDPCSNMean SDMCSNMean SDPCSNMean SDMCSNMean SDPCSNMean SDMCSNMean SDPCSNMean SDMCSNMean SDInvestigationalControlP*5634.2 7.35932.0 7.10.1115646.3 12.45949.0 9.50.1935542.8 9.05838.9 8.90.0255553.2 8.65849.8 9.50.0515448.3 8.25745.8 9.50.1335453.7 7.95749.9 10.40.0374949.0 9.65445.3 11.20.0794955.3 6.15451.2 10.80.0205550.8 9.35446.7 10.70.0365554.4 8.45452.6 9.00.2823650.5 9.63544.6 10.60.0163654.6 7.73550.5 10.10.055*P values for change from preoperative in each group are from paired t test.Outcomes DataThe changes in the mean SF-36 Physical Component Subscores (PCS) were notable (Table 3A, Fig. 4).The mean preoperative score for the BRYAN group was34, whereas it was 32 for the Control group (P 0.111).The 12-month follow-up PCS data were available for 109patients (55 BRYAN and 54 Control). At this interval,the mean PCS had increased to 51 for the BRYAN groupand 47 for the Control (P 0.036). At 24 monthspostoperatively, the mean PCS for the BRYAN groupwas 50, whereas the Control group mean was 45(P 0.016). At that same time point, the PCS changefrom the preoperative score (Table 3B) was significant inboth the Investigational and Control groups (P 0.001).The mean preoperative SF-36 Mental ComponentSubscore (MCS) was 46 and 49 for the BRYAN andControl groups, respectively (P 0.193). By 24 monthsafter the surgery, the mean MCS values were 55 for theBRYAN group and 50 for the Control group (P 0.055)(Table 3A). At that same time point, the MCS changefrom the preoperative score (Table 3B) was significant inthe Investigational group (P 0.005) and insignificant inthe Control groups (P 0.565).The mean preoperative NDI scores were 47 and 49for the BRYAN and Control groups, respectively484TABLE 3B. SF-36 Health Survey Scores—24 mo ChangePeriodPreoperative24 moVariablePCSNMean SDMCSNMean SDPCS change frompreoperativeNMean SDP*MCS change frompreoperativeNMean SDP*InvestigationalControl5634.2 7.35932 7.15646.3 12.45949 9.53615.8 9.5 0.0013512.4 11.0 0.001365.8 11.60.005351.1 11.00.565*P values for change from preoperative in each group are from paired t test.(P 0.454) (Table 4A). Twelve-month follow-up datawere available for 109 patients (55 BRYAN and 54Control) with the mean NDI scores falling to 10 in ther2007 Lippincott Williams & Wilkins
J Spinal Disord Tech Volume 20, Number 7, October 2007FIGURE 4. SF-36 PCS Scores—a graphical representation.32BRYAN group and 18 among the Control patients. Thedegree of improvement was significantly greater in theBRYAN cohort at this time point (P 0.012). Two-yearfollow-up data were available for 71 patients (36 BRYANand 35 Control). At this interval, the mean NDI forscores the BRYAN and Control groups were 12 and 23,respectively (P 0.006). At the 2-year interval, the NDIchange from the preoperative score (Table 4B) wassignificant in both the Investigational and Control groups(P 0.001).The mean neck pain VAS values preoperativelywere 72 and 73 for the BRYAN and Control groups,respectively (P 0.845) (Table 5A, Fig. 5). Twelvemonth follow-up data were available for 109 patients(55 BRYAN and 54 Controls) with the mean VAS valuesimproving to 17 in the BRYAN group and to 27 in theMulticenter BRYAN Disc StudyControl patients. The degree of neck pain improvement atthis time point was equivalent between the 2 groups(P 0.056). For the 71 patients reaching 2-year followup (36 BRYAN and 35 Control), the mean VAS for theBRYAN group was 19 and for the Control group 36. Bythis time point, the neck pain improvement seemed to besignificantly better for the BRYAN patients (P 0.014)(Fig. 5). In addition to the group-to-group differencesnoted, both groups demonstrated a significant improvement in comparison with their preoperative scores(P 0.001) (Table 5B).The mean arm pain VAS values (Table 6A)preoperatively were 70 (BRYAN) and 71 (Control). At12 months, follow-up data were available for 109 patients(55 BRYAN and 54 Controls) with the mean BRYANarm pain VAS values improving to 12 and mean Controlvalues improving to 22 (P 0.037). For the 71 patientsreaching 2-year follow-up, the mean arm pain VAS forthe BRYAN group was 17, whereas it was 27 for theControl group (P 0.152). Although no group-to-groupdifferences were noted at 24 months, both groupsdemonstrated a significant improvement in comparisonwith their preoperative scores (P 0.001) (Table 6B).Target-level Motion AnalysisCervical vertebral bodies were tracked on the digitalradiographs using quantitative motion analysis software(QMA, Medical Metrics, Houston, TX) to calculate thefunctional spine unit motion parameters. As expected,significantly more motion (3, 6, 12, and 24 mo) wasretained in the disc replacement group than the platedgroup at the index level. The disc replacement groupTABLE 4A. NDI ScoresPeriodPreoperative Pain Score6 wk Pain Score3 mo Pain Score6 mo Pain Score12 mo Pain Score24 mo Pain ScoreVariableInvestigational (N 56)Control (N 59)NMean SDNMean SDNMean SDNMean SDNMean SDNMean SD5646.5 17.25519.5 16.35413.4 13.54911.8 13.4559.9 12.93611.6 15.65948.7 15.15829.0 17.45722.8 20.05420.5 19.55417.8 19.03523.1 18.6P0.4540.0030.0050.0100.0120.006TABLE 4B. NDI Scores—24 mo ChangePeriodNeck Disability Index ScoresPreoperative Pain Score24 mo Pain ScoreVariableNMean SDChange from preoperativeNMean SDP*Investigational (N 56)Control (N 59)5646.5 17.25948.7 15.136 28.9 15.0 0.00135 23.7 19.9 0.001*P values for change from preoperative in each group are from paired t test.r2007 Lippincott Williams & Wilkins485
J Spinal Disord TechSasso et al Volume 20, Number 7, October 2007TABLE 5A. Neck Pain ScoresPeriodPreoperative Pain Score6 wk Pain Score3 mo Pain Score6 mo Pain Score12 mo Pain Score24 mo Pain ScoreVariableInvestigationalControlNMean SDNMean SDNMean SDNMean SDNMean SDNMean SD5672.0 24.75528.5 24.15423.6 22.74922.2 23.05517.2 22.43618.5 26.25872.8 24.05835.7 26.35734.9 29.55432.7 30.15427.0 30.43535.6 30.6P0.8470.1310.0260.0520.0560.014TABLE 5B. Neck Pain Scores—24 mo ChangePeriodPreoperative Pain Score24 mo Pain ScoreVariableNMean SDChange from preoperativeNMean SDP*InvestigationalControl5672.0 24.75872.8 24.036 48.2 30.5 0.00135 36.4 31.1 0.001*P values for change from preoperative in each group are from paired t test.retained an average of 7.3 degrees at 12 months and 7.0degrees at 24 months (Table 7A). In the 24-monthBRYAN group, this did not represent a statisticallysignificant change from the preoperative measuredangulation at the target level (P 0.104). In contrast,the average range of motion in the fusion group was 1.3degrees at the 3-month follow-up and gradually decreasedto 0.9 degrees at 24 months, a significant change from thepreoperative measurements (P 0.001) (Table 7B).ComplicationsOver the 24-month follow-up period, a total of 7subsequent surgical interventions were performed in thestudy population (4 Control, 3 Investigational). Allsubsequent surgical interventions were performed by theinitial treating surgeon at the discretion of that surgeon(Table 8). One patient in the Control group (JA17,Table 8) required a posterior cervical fusion for symptomatic nonunion. Another patient in the Control group(LA07, Table 8) required revision ACDF for nonunion,which was performed with allograft and rhBMP-2(INFUSE, Medtronic Sofamor Danek, Memphis, TN)and revision anterior cervical plating. This same patientlater required posterior fusion with autograft for arecurrent nonunion. Two patients in the Control grouprequired ACDF for adjacent level disease during the24-month period (VA11 and VA20, Table 8).Three patients in the Investigational group requiredACDF for adjacent level disease during the 24-monthfollow-up period (VA 25, 35, and 59, Table 8). There wereno incidents of radiographic or clinical implant complications noted at the target surgical levels (BRYAN discreplacement) in the Investigational group. No spontaneous fusion or heterotopic ossification (HO) events wereobserved in the Investigational group.DISCUSSIONFIGURE 5. Neck Pain Scores—a graphical representation.32486At the time of this writing, multiple cervical discarthroplasty devices are involved in US IDE trials. Nodevice has yet obtained FDA approval. This 24-month,3-site series represents a subset of the 31 institutionsinvolved in the FDA IDE trial for the BRYAN cervicaldisc replacement. As expected, the 1:1 randomizationprocess yielded demographically similar study groups.The surgical data were similar in many respects with atrend toward longer hospital stay and longer operativetime in the Investigational BRYAN group. Our studydemonstrates significant improvement (Investigationalr2007 Lippincott Williams & Wilkins
J Spinal Disord Tech Volume 20, Number 7, October 2007Multicenter BRYAN Disc StudyTABLE 6A. Arm Pain ScoresPeriodPreoperative Pain Score6 wk Pain Score3 mo Pain Score6 mo Pain Score12 mo Pain Score24 mo Pain ScoreVariableInvestigationalControlNMean SDNMean SDNMean SDNMean SDNMean SDNMean SD5669.8 19.05515.5 22.25415.8 23.04915.6 24.45511.9 19.63616.8 28.25970.7 23.75823.5 25.95722.0 30.75424.0 28.85422.2 30.23526.9 30.3P0.8320.0780.2340.1160.0370.152TABLE 6B. Arm Pain Scores—24 mo ChangePeriodPreoperative Pain Score24 mo Pain ScoreVariableNMean SDChange from preoperativeNMean SDP*InvestigationalControl5669.8 19.05970.7 23.736 48.9 27.2 0.00135 42.9 37.0 0.001*P values for change from preoperative in each group are from paired t test.group vs. Control group) in multiple outcome measuresat 12 and 24 months including: SF-36 PCS, NDI, andneck pain VAS. Although both surgical groups hadstatistically significant improvement in all outcomemeasures at 24 months with respect to their preoperativescores, the outcome-based group-to-group comparison atthe follow-up intervals is highly suggestive of the benefitof the Investigational implant in the 24-month periodexamined by this study.Our results with regard to surgical outcomes aresimilar to those of other investigators and represent thelargest single randomized, controlled, prospective seriesof patients with BRYAN Disc arthroplasty followed to 24months. Goffin et al3 reported early results of a multicenter study of the BRYAN Disc performed at a singledisc space in 60 patients for the treatment of radiculopathy or myelopathy owing to disc herniation orspondylosis failing at least 6 weeks of conservativetreatment. Exclusion criteria included previous cervicalspine surgery, axial neck pain as the sole symptom,significant anatomic deformity, and radiographic evidence of instability (translation 2 mm or 11 degreesof angulation compared with the adjacent level). Patientoutcomes were determined by the Cervical Spine Research Society and SF-36 instruments. Clinical successrates at 6 months and 1 year were 86% and 90%,respectively, exceeding the study’s targeted success rateof 85%. Unfortunately, the study’s findings have beensubject to some skepticism, because there was no Controlgroup.In a separate report, Goffin et al4 have recentlypublished the intermediate-term results of this multicenterr2007 Lippincott Williams & Wilkinsstudy. The study was expanded to include a second armevaluating the treatment of 2 adjacent disc levels. Thesingle-level arm had 103 patients enrolled with 100reaching the 1-year mark and 51 reaching 2-year followup. The bilevel study arm was comprised of 43 patientswith 1-year data completed on 29 patients and 2-year dataavailable on 1 patient. Success rates in the single-levelstudy at 6 months, 12 months, and 24 months were 90%,86%, and 90% respectively. In the bilevel study, thesuccess rate at 6 months was 82% and 96% at 1 year. Nodevice failures or subsidence were observed in any patient.At 1-year follow-up, flexion-extension range of motionper level averaged 7.9 degrees in the single-level arm and7.4 degrees in the bilevel arm.Anderson et al2 described the follow-up results of 73patients who had greater than 2-year follow-up status ona 1-level BRYAN Disc Arthroplasty. Forty-five of thesepatients were rated as excellent, 7 as a good, and 13 asfair. Only 8 patients had a poor rating at the 2-yearfollow-up. SF-36 functional outcome data demonstratedsignificant improvement from preoperative to 3-monthpostoperative time points. These outcomes remainedstable 24 months after the surgery. There was noradiographic evidence of subsidence of implants. Eightynine percent of all patients had at least 2 degrees ofmotion at 1 and 2 years. Average range of motion was8 degrees. There was one early anterior device migrationassociated with a partially milled cavity.This same report noted the results of 30 patientswho had 2 level disc arthroplasty and had reached the 1year end point in follow-up. Twenty-one of the patientswere rated as excellent, 3 good, 5 fair, and 1 poor.487
J Spinal Disord TechSasso et al Volume 20, Number 7, October 2007TABLE 7A. Summary of Angular Motion at Treated* LevelsInvestigationalPeriodPreoperative3 mo6 mo12 mo24 moVariableAngulation at theNMean SDAngulation at theNMean SDAngulation at theNMean SDAngulation at theNMean SDAngulation at theNMean SDControlReader 1Reader 2AveragewReader 1Reader 2Averagew1406.30 3.991746.39 3.691366.51 3.371227.06 4.281559.21 5.181208.15 4.431755.26 3.001696.78 3.621685.97 3.13761.49 1.44771.06 1.04721.26 0.991746.34 3.871667.89 4.211657.12 3.83781.80 3.25821.09 1.31731.37 1.721386.29 4.101378.21 4.771367.27 4.28801.19 1.34680.77 0.99630.94 0.81686.01 4.30587.88 4.43577.04 4.29441.12 1.34380.79 0.73330.85 0.71target leveltarget leveltarget leveltarget leveltarget level*The values of angulations at treated levels are the absolute value of (EXT-FLEX) from the 2 readers’ measurements.wIf the value of 1 of 2 readers’ is missing, then the average is treated as missing.TABLE 7B. Summary of Angular Motion at Treated* Levels—24 mo ChangeInvestigationalPeriodPreoperative24 moVariableAngulation at the target levelzNMean SDChange from preoperative for angulationat the target levelzNMean SDP*ControlReader 1Reader 2AveragewReader 1Reader 2Averagew1406.30 3.991746.39 3.691366.51 3.371227.06 4.281559.21 5.181208.15 4.43470.87 6.390.357522.07 4.610.002411.40 5.390.10439 5.64 4.18 0.00134 8.42 5.87 0.00128 6.52 4.36 0.001*The values of angulations at treated levels are the absolute value of (EXT-FLEX) from the 2 readers’ measurements.wIf the value of 1 of 2 readers’ is missing, then the average is treated as missing.zP values for change from preoperative in each group are from paired t test.A significant improvement in SF-36 functional outcomemeasures was noted postoperatively. There was noradiographic evidence of subsidence in the 2-levelpatients. At 1 year, 84% of patients had at least 2 degreesof motion at both disc levels. The average amount ofmotion at each disc level was also 8 degrees. There wasone posterior migration of a device, again associated witha partially milled cavity. Complications in the study as aTABLE 8. tional/C5-6Adjacent LevelSupplemental FixationPosterior cervical fusionat C5-6Posterior cervical fusionafter revision evision ACDF withrhBMP-2 and anteriorspinal instrumentationwith Atlantis ller.VA-Hacker.488r2007 Lippincott Williams & Wilkins
J Spinal Disord Tech Volume 20, Number 7, October 2007whole included: 1 cerebrospinal fluid leak, 1 esophagealinjury, 4 hematoma evacuations, and 3 revision decompressions.2Sekhon20 reported early results of 7 patients withcervical spondylotic myelopathy who were treated withanterior decompression and reconstruction with theBRYAN Disc. Follow-up ranged from 1 to 17 months.On average, the Nurick grade improved by 0.72 andOswestry NDI scores improved by 51.4 points. Improvement in cervical lordosis was noted in 29% of thepatients. No complications were repor
in a 1:1 ratio to either a BRYAN Cervical Disc (N 56) or an anterior cervical fusion with allograft and a plate (N 59). There were 30 males and 26 females in the BRYAN group and 32 males and 27 females in the fusion group. The average age was 42 years (BRYAN) and 46 years (Control). No statistically significant differences