Transcription
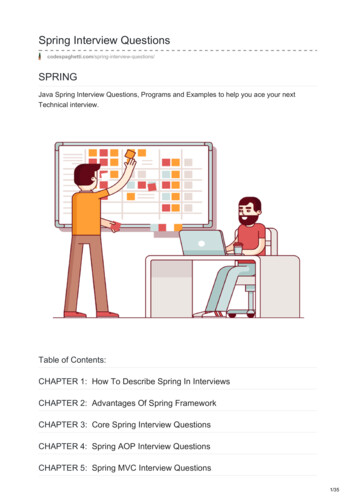
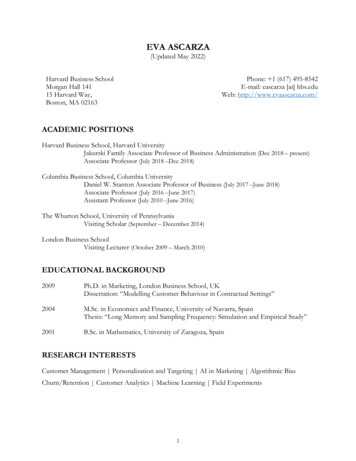
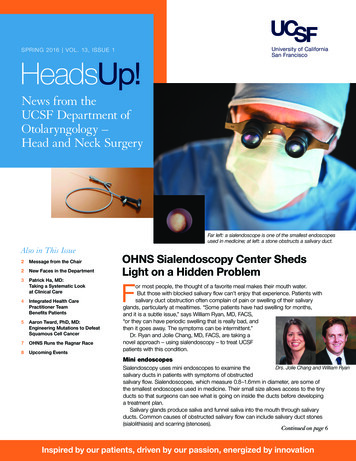
SPRING 2016 VOL. 13, ISSUE 1HeadsUp!News from theUCSF Department ofOtolaryngology –Head and Neck SurgeryFar left: a sialendoscope is one of the smallest endoscopesused in medicine; at left: a stone obstructs a salivary duct.Also in This Issue2Message from the Chair2New Faces in the Department3Patrick Ha, MD:Taking a Systematic Lookat Clinical Care4Integrated Health CarePractitioner TeamBenefits Patients5Aaron Tward, PhD, MD:Engineering Mutations to DefeatSquamous Cell Cancer7OHNS Runs the Ragnar Race8Upcoming EventsOHNS Sialendoscopy Center ShedsLight on a Hidden ProblemFor most people, the thought of a favorite meal makes their mouth water.But those with blocked salivary flow can’t enjoy that experience. Patients withsalivary duct obstruction often complain of pain or swelling of their salivaryglands, particularly at mealtimes. “Some patients have had swelling for months,and it is a subtle issue,” says William Ryan, MD, FACS,“or they can have periodic swelling that is really bad, andthen it goes away. The symptoms can be intermittent.”Dr. Ryan and Jolie Chang, MD, FACS, are taking anovel approach – using sialendoscopy – to treat UCSFpatients with this condition.Mini endoscopesDrs. Jolie Chang and William RyanSialendoscopy uses mini endoscopes to examine thesalivary ducts in patients with symptoms of obstructedsalivary flow. Sialendoscopes, which measure 0.8–1.6mm in diameter, are some ofthe smallest endoscopes used in medicine. Their small size allows access to the tinyducts so that surgeons can see what is going on inside the ducts before developinga treatment plan.Salivary glands produce saliva and funnel saliva into the mouth through salivaryducts. Common causes of obstructed salivary flow can include salivary duct stones(sialolithiasis) and scarring (stenoses).Continued on page 6Inspired by our patients, driven by our passion, energized by innovation
Message from the ChairUCSF is the Nation’s #1 OHNSDepartment for NIH FundingOur UCSF Department of Otolaryngology – Head and Neck Surgerynow ranks #1 in the nation in NIH funding in Otolaryngology!Our research footprint at UCSF has rapidly expanded in thepast few years. This expansion is enabled by resources, recruitment, andthe institution’s commitment to cancer care at the UCSF Helen DillerFamily NCI-Designated Comprehensive Cancer Center at Mission Bay.Associate Vice Chancellor Jennifer Grandis, MD’seffort in the Head and Neck Oncology Lab is now upand running and expanding through her partnershipwith Patrick Ha, MD. UCSF is now participating in ahead and neck oncology-focused SPORE programfrom the NIH.Other areas of traditional research strength withinour department are also growing. Hearing researchand central auditory processing research within theColeman Lab and Epstein Lab is secured bycontinuous NIH funding earned by our team over thepast three decades. Dylan Chan, MD, PhD, has a newR21 grant to study connexin 26; Young-Wook Jun,Andrew H. Murr, MDPhD, has been funded with multiple grants devoted tonano particle research (he just had a paper accepted to Cell!); and JohnHoude, PhD, and Sri Nagarajan, PhD, continue an extremely successfulcollaboration incorporating imaging technology. And this is not even thewhole story.The department is also in the midst of major clinical recruitments. Thisyear we will add two new pediatric otolaryngologists who will work at bothUCSF Benioff Children’s Hospital Oakland and Benioff Children’s HospitalSan Francisco, two new skull base and rhinology surgeons, and avestibular otologist/neurotologist to round out our fantastic otology team.Our clinical activities continue to address unusual problems. As youwill read in the cover story of this edition of Heads Up!, Jolie Chang, MD,and William Ryan, MD, are taking a novel approach to treating patientswith salivary duct obstruction. They are using sialendoscopy to helpdiagnose salivary duct blockage problems and to guide minimally-invasivesurgical techniques to treat the problems.And yet there is more to come. Please visit our new website(http://ohns.ucsf.edu) to become informed about the major strides beingmade in expert clinical care, research innovation, and a continuingtradition of expertise in teaching and mentorship.Warmly,Andrew H. Murr, MDChairman, Professor of Clinical Otolaryngology – Head and Neck Surgery,Roger Boles, MD Endowed Chair in Otolaryngology EducationDepartment of Otolaryngology – Head and Neck Surgery2HeadsUp! Spring 2016New Facesin the DepartmentThe Department of Otolaryngology – Head and NeckSurgery is being bolstered withthe addition of a seasonedadministrator and threeoutstanding academicians.In December2015 MaryBobel, MBA,joined UCSFas the ChiefAdministrativeOfficer for theDepartmentsof OHNSand Radiology. Ms. Bobel hasextensive management experiencein institutional academic settings.She served as the manager of theDepartment of Radiology at theStanford University School ofMedicine and worked withinStanford’s Office of InstitutionalPlanning. Previously, she managedthe Department of Radiologyat the University of Chicago PritzkerSchool of Medicine. Ms. Bobelholds a BA, an MA and an MBAfrom Stanford University.Dan Johnson,PhD will joinUCSF OHNSas a Professorin June, 2016.He matriculatedat PrincetonUniversity, wherehe obtainedan MA and PhD in MolecularBiology. Dr. Johnson completed apostgraduate fellowship at UCSFfrom 1988–1993. He then came upthrough the ranks within theDepartment of Medicine at theUniversity of Pittsburgh until hebecame a professor there in 2012.Dr. Johnson has been on the editorialboard of Cancer Research and is thesection editor of Leukemia. He hasbeen honored with the G. DavidRoodman Excellence in MentorshipAward from the Hematology/Oncology Fellows at Pitt in 2014.Continued on page 6
Interview: Patrick Ha, MDTaking a Systematic Look at Clinical CarePatrick Ha, MD, was named Chief of Head and Neck Oncologic Surgery at UCSF when he joined theDepartment of Otolaryngology – Head and Neck Surgery in October 2015. Heads Up! recently caught upwith Dr. Ha and asked him about his new role at UCSF:What attracted you to UCSF?Over the course of 20 years I was atJohns Hopkins – completing medicalschool, otolaryngology residencytraining, a fellowship, and serving onthe faculty. When I heard about thisopportunity at UCSF, several aspectsof the position intrigued me. There isa very well-rounded clinical team aswell as great potential for growth.That is, we just moved to a new campusand there is a new cancer centerdirector, Dr. Alan Ashworth, and a newClinical Translational Science Institutedirector, Dr. Jennifer Grandis, whoboth recently moved to UCSF. So theculmination of all these forces, bothclinical and research, made this a veryappealing opportunity.Describe your role as new chiefof head and neck surgery?From a clinical standpoint I am directorof operations for the Division of Headand Neck Surgical Oncology at MissionBay. I make sure everything runsappropriately, that we have the rightstaffing, and that we have the rightpeople from a physician standpoint.I view my role on a larger scale asa clinical provider – trying to providethe best care for my own patients, butalso thinking about the role moresystematically. One initiative that theinstitution has been really excitedabout is the concept of the UnitBased Leadership Team, or UBLT,which follows the philosophy ofLean Toyota Management. The goalsare to institute continuous processimprovement and to create systemsthat are sustainable and also increasesatisfaction for providers and staff –to make the workplace both happierand more streamlined. These efforts willallow for a better patient experience,improve the efficiency of healthcaredelivery, and improve patient access.For example, we have decreasedour wait time for patients to be seen.One of the metrics that UCSF uses isthe percentage of patients who areseen within two weeks. Currently ourdivision’s numbers are at 90 percent,which is well above our institutional goal,but I would like to see that go evenhigher. So we have done some thingsthat have really made a difference interms of providing access to care, andwe will continue to assess our results.From another clinical standpoint,my role is to integrate the team. I wouldsubmit that our patients are amongthe most complex – from an oncologicand general provider standpoint –in terms of the number of resourcesand individuals that touch the patientduring their treatment. Patient careareas include medical oncology,radiation oncology, dental oncology,oral surgery, nutrition, speech languagepathology, social work, physicaland occupational therapy, symptommanagement, and neuropsychology.Trying to organize and capitalize on allour strengths in those areas has been abig part of my job as well.What are your areas of research?My research has been focused on themolecular biology of head and neckcancer and most specifically salivarygland cancers. One particular type ofcancer, adenoid cystic carcinoma, iswhere I have dedicated most of myeffort. It is rare – there are only about1,000 cases in the U.S. per year – butit’s a very good tumor model to studyin many ways. One problem is thatthe prognosis is very uncertain. Somepatients do really well and other patientsdo not. It’s frustrating because wedon’t have a good way of telling whichpatients are going to do well. Abouthalf the patients will develop metastases,but we can’t tell which patients. Ourcurrent treatment methods have notchanged much in the past 20 years. It iscoincidental that my DistinguishedProfessorship is named after Dr. IrwinJacobs, who happened to have beentreated for adenoid cystic carcinoma.He generously endowed this position,so I have even more inspiration tocontinue my research in this area.“The most important thingto me is to build a team.that works seamlessly, thatprovides the best patientcare possible, in the bestway possible.”– Patrick Ha, MDTell us your goalsThe most important thing to me is tobuild a team that encompasses all of thecore values that we hold every day – ateam that works seamlessly, thatprovides the best patient care possible,in the best way possible. It’s a matter ofengaging that team and facilitating thatcare so when a patient comes, ourcommunication lines are open and ourexperts in all of the disciplines are readyto surround the patient and provide thebest care possible.From a research standpoint, I alsowant to build upon our current team ofhead and neck cancer researchers andengage the brilliant research communityat UCSF to further our work. Ultimately,our goal is to develop novel therapiesthat will change the way head and neckcancer is treated. nHeadsUp! Spring 20163
Clinical TeamIntegrated Health Care PractitionerTeam Benefits PatientsThe UCSF Otolaryngology – Headand Neck Surgery department’sdiverse clinician team comprisesPhysician Assistants (PAs) andNurse Practitioners (NPs), who workcollaboratively with departmentfaculty physicians to provide excellentpatient care.“We are fortunate to have recruitedand trained a group of knowledgeableand compassionate providers whoevaluate and treat patients acrossthe diversity of subspecialties in ourdepartment, including performingin-office diagnostic and therapeuticprocedures,” says team leader,Laura Kirk, PA-C.“Our collaborative approach ensuresthat both our new and establishedpatients receive timely access to carefor their concerns, with faculty otolaryngologists readily available for assumingcare of more complex patients or thosewho require surgery,” she adds.Both PAs and NPs are licensed healthcare professionals with extensive postgraduate training. PAs are nationallyboard-certified health care providerswho have completed two to three yearsof postgraduate medical training. NPsare nationally board-certified advancedpractice nurses who have completedtwo to three years of master’s degreenursing training. Both PAs and NPs arewidely accepted by patients and maybe more accessible to patients thanphysicians, often spending more timewith each patient.In the UCSF Department ofOtolaryngology – Head and NeckSurgery, both PAs and NPs see patientswith general otolaryngology, pediatricotolaryngology, and head and necksurgery conditions.“We utilize the most up to datetechnology and evidence-basedmedicine to care for our patients inpreventive care, diagnosis, andtreatment. This includes prescribingmedications, performing outpatientprocedures, and assisting in surgery,”notes Ms. Kirk.“The UCSF OHNS team’scollaborative approach is designedto directly benefit our patients byimproving access to and coordination ofcare at all levels,” points out DepartmentChairman Andrew H. Murr, MD.PAs and NPs are subject to periodicpeer review and clinical outcomeevaluations, just like the physicianfaculty. In addition to providing directpatient care, UCSF Otolaryngology –Head and Neck Surgery PAs andNPs are also involved in clinicaleducation, clinical research, andquality improvement initiatives; andthey may have supervisory duties.From left: Roseanne Krauter, Regina Gould, Trina Sheedy, Laura Kirk, Brittany McGinnisOkimura, Shauna Brodie, Suzanne Petersen, Cosette Audirac4HeadsUp! Spring 2016Meet the OHNSPA and NP TeamLaura Kirk, MSPAS, PA-C(General Otolaryngology Practiceand PA/NP Team Supervisor)joined the UCSF team in 2008 asthe first PA or NP in the OHNSdepartment. She sees patients ofall ages and otolaryngologyconcerns, teaches nationally ondizziness and various pediatricotolaryngology topics, and alsoteaches in the UCSF MedicalSchool and UCSF Pediatric NursePractitioner Program. Her clinicalinterests include infant feedingdisorders, dizziness, tinnitus,and sudden hearing loss.Trina Sheedy, MMS, PA-C(Head and Neck SurgicalOncology) joined the team in2013. She sees adult patients withhead and neck surgery concernsincluding benign and malignanttumors, thyroid and parathyroiddisorders, and salivary glanddisorders and has a clinicalinterest in diagnostic andtherapeutic use of ultrasoundfor these conditions.Brittany McGinnis Okimura,MMS, PA-C (PediatricOtolaryngology) joined the teamin 2014. She sees pediatricpatients at both the San Franciscoand Oakland locations of UCSFBenioff Children’s Hospital.Ms. Okimura’s clinical interests
are obstructive sleep apnea,pediatric ear disorders, epistaxis,and newborn feeding difficulties.Roseanne Krauter, MSN,FNP-C (General Otolaryngology,Otology) joined our team in 2015.She sees adult patients with allotolaryngology concerns, and hasinterests in unilateral sensoryhearing loss, cochlear implantationimplementation for single-sideddeafness, and vestibular disorders.Shauna Brodie, MS, FNP-C(General Otolaryngology) joinedthe OHNS team at San FranciscoGeneral Hospital in 2015. Ms.Brodie’s clinical interests includeaddressing disparities in healthcare by improving accessibility andcultural competence, both locallyand internationally.Regina Gould, MMSC, MPH,PA-C (General Otolaryngology)joined the team in 2016. She seesadult patients at the Parnassuscampus, assisting in the operatingroom and providing inpatientcontinuity of care within UCSF’sunique hospitalist-model ofotolaryngology. She also seesadult outpatients at the MountZion clinic location. Her interestsinclude sinus disease, airwayemergencies, and cross culturalbarriers to delivery of health care.Suzanne Petersen, MSPAS,PA-C (Pediatric Otolaryngology)joined the team in 2016 and seespatients at the Oakland campus ofUCSF Benioff Children’s Hospital.Ms. Petersen’s clinical interestsinclude pediatric hearing loss,craniofacial anomalies, andnewborn feeding difficulties.Cosette Audirac, MSPAS, MPH,PA-C (Pediatric Otolaryngology)joined our team in 2016.Focused on providing care toSpanish-speaking patients andfamilies and other underservedpopulations, she sees pediatricotolaryngology patients at both theSan Francisco and Oaklandlocations of UCSF BenioffChildren’s Hospital. Ms. Audirac’sclinical interests are congenitalhearing loss, sleep disorderedbreathing, and naturopathic andalternative medical therapy. nResearch Profile: Aaron Tward, PhD, MDEngineering Mutations toDefeat Squamous Cell CancerAaron Tward, PhD, MD, has studiedmany things during a diverse career,but his current interest is cancerbiology and how normal tissue goes awry inbecoming cancer, with specific work insquamous cell carcinoma. To get to thatsubject he took a circuitous route, whichincluded cancer research with formerUCSF chancellor and Nobel laureate J.Michael Bishop, MD; work in Dr. ElizabethBlackburn’s lab, which was focused ontelomeres; and investigative activities at theBroad Institute, which he describes asthe “center of the bioinformatics universethat had great sequencing expertise.”During his residency at The HarvardCombined Program in Otolaryngologystarting in 2007, he met Todd Golub, MD,of the Broad Institute. Dr. Tward tookadvantage of research blocks in his residency to investigate the genetic underpinnings of cancer in the Golub laboratory.As Dr. Tward describes it, “in themid-2000s sequencing technology –that is the ability to determine DNAsequences – got much better. Basically itbecame feasible then, in an unbiasedfashion, to say ‘okay I am going to, withina sample of tissue, determine thesequence of an entire genome.’”At the time, one of the wealthiest menin the world, Carlos Slim Helú, donatedenough money to the Broad Institute to fundthe sequencing of many tumors, includingbreast cancer and head and neck cancer.As a PhD-trained cancer biologist whoalso knew about head and neck cancer,Dr. Tward was paired with Nico Stransky,a good friend of his, to sequence headand neck squamous cell carcinoma.“We worked our tails off, and ultimatelyfound all kinds of mutations that were ofinterest,” he says. They published a paperin Science in 2011, which was one of thevery first reports of genome-wide mutationsthat are present in any tumor type.In 2014, Dr. Tward accepted an appointment as an assistant professor at UCSF tostart a lab that is currently engineeringauthentic models of the human disease.“We engineer in the same mutations, inorder to recapitulate the diversity of humandisease and have authentic models so thatwe can figure out what those genes doand how those genes interact,” he says.To recapitulatethe disease, thelab is usingprimary humantissue. They arerecreating theorgan structure inculture and thenputting in thesame mutationsthat cause the human disease.The hope is to create squamous cellcarcinoma that faithfully recapitulatesaspects of the disease. He and histeam hope to create unbiased screenswhere they can alter the model and notethe results.“Squamous epithilium is tissue thathas barrier function,” he explains. “Thecells in the basal layer are the ones thatmake more cells. Ultimately the cells thatreach the top layer lose their nuclei andslough off. Cancer of your skin looks like itharbors pretty much the same mutationsthat cancer of the squamous epithilium inyour mouth does, which is the same aslung squamous cell cancer, which lookspretty much the same as bladder orcervical or the subset of cervical cancer.That means that if we find ways to targetthese mutations, it is probably applicableto many different types of cancer.”“This will reform the entire threedimensional structure in vitro,” says theresearcher. “And even better, if you nowengineer mutations into these, you will startseeing mutations that look like cancer.Squamous cell cancer in general is definedby when these cells pass through thisbasement membrane, and once theyinvade that, they are, by definition, cancer.You can see this in vitro also.”The significance of Dr. Tward’s workrests on global best estimates that 1.5percent of the world’s population will die ofsquamous cell cancer.“That’s a lot of people,” he says. “Itbasically means that if a given mutation isreally important and present in 20 to 30percent of tumors, then if you reverse themutation, at the very least you will extendsomebody’s life a lot. This means that adrug could be applied to cancer that one totwo percent of people in the world have –that’s a big impact.” nHeadsUp! Spring 20165
Sialendoscopy CenterContinued from front pageSialendoscopy is a huge aid in diagnosing the salivary duct blockage problems,and it is used to guide minimally-invasive surgical techniques to treat the problems.“In addition to giving us visualization, sialendoscopes also have side ports throughwhich basket snares or graspers or even plasticballoons can be delivered to the duct to removethe stones or widen the ducts when they arenarrowed from scarring,” Dr. Ryan explains. “Thesialendoscopes also let us see if the work that wehave done is effective. So, if we have rerouted orbypassed a duct or created a new opening into aduct, we can use the sialendoscope to determineSalivary duct stonethat the duct reconstruction was successful.”Sparing the gland“An overall goal for these minimally invasive techniques is to preserve the salivarygland.” says Dr. Chang. “To avoid the need to surgically remove the entire gland –the traditional recommendation – we aim to treat the source of obstruction within theduct. We have found that removing the stone or treating a stenosis directly hasproduced excellent results and high rates of patient satisfaction.”Dr. Ryan adds that “after sialendoscopy there is just a small surgical wound thatneeds to heal. The patient wakes up and can eat and go home right away. They willnotice a fairly dramatic change, and the change seems to be durable for mostpatients. For salivary stones, sialendoscopic assisted techniques work very well.”Pioneers in the fieldUCSF has a rich history in pioneering sialendoscopy and minimally invasive salivaryduct surgery. David Eisele, MD, was one of the first American surgeons to bring theequipment and techniques to the United States from Europe when he was the chairof UCSF’s Department of Otolaryngology – Head and Neck Surgery.“Thanks to David Eisele, UCSF pioneered one of the first U.S. sialendoscopycenters in 2004. At UCSF, we are dedicated to advancing the field with our researchand by teaching physicians around the country how to incorporate these techniquesinto their practices,” says Dr. Chang, who notes that “we started a sialendoscopyand salivary duct surgery instructional course in 2014 and have been offering itannually due to interest from otolaryngologists around the country.”“The mentorship that I received at UCSF as a fellow has been a springboard todevelop this part of my career,” comments Dr. Ryan. “Dr. Eisele really developedsialendoscopy at UCSF to the point where he had a robust practice. Jolie Changand I both learned from him. We currently collaborate with a group of U.S. experts insialendoscopy and have developed our own training course.”“As a newer technique, I have found it interesting to define how sialendoscopycan be used to help our patients, and we continually strive to find ways to improvehow surgery is performed – how to reduce morbidity, how to be less invasive, howto be better at diagnosing and choosing effective therapies,” Dr. Chang adds.Tracking outcomes“Will Ryan and I have developed the first specific clinical questionnaire for patientswith obstructive salivary disease to help understand how patients improve aftersurgery” notes Dr. Chang. “We aim to use it as a clinical tool to characterize diseaseseverity and understand patient outcomes.”The two surgeons are collecting feedback from patients with obstructed salivaryflow both before treatment and at intervals after treatment. “The questionnairescores not only symptoms, but it has an aggregate score, and the scores haveshown what procedures work” notes Dr. Ryan. “We are really interested in thesubtleties of the treatments we give and what works best so that we can counselpatients and predict real outcomes of the procedures for patients.” n6HeadsUp! Spring 2016New Facesin the DepartmentContinued from page 2In June 2016JordanVirbalas, MD,will join thedepartmentas a ClinicalAssistantProfessor andwill be situated atUCSF Benioff Children’s Hospital inOakland as a member of the pediatricotolaryngology team. Dr. Virbalasearned his masters in the Science ofTeaching from Pace University inNew York and attended the HarvardExtension in Health Careers.Dr. Virbalas received his MD in 2010from Weill Cornell Medical Collegein New York. His residency inotolaryngology – head and necksurgery was completed in 2015 atAlbert Einstein College of Medicinein New York, followed by a fellowshipin pediatric otolaryngology – headand neck surgery at the Children’sHospital Colorado in Aurora.Gretchen M.Oakley, MD,will join thedepartment inAugust 2016 as aClinical AssistantProfessor.Dr. Oakleyreceived her MDfrom Saint Louis University Schoolof Medicine in Missouri in 2010,followed by a five-year otolaryngology– head and neck surgery residencyat the University of Utah Hospitalsand Clinics in Salt Lake City. Shewas the 2014 recipient of theSteven D. Gray Memorial ResearchAward from the University of Utah’sOtolaryngology – Head and NeckSurgery Department and is firstauthor on five scientific publications.Dr. Oakley’s fellowship, in rhinologyand skull base surgery, will becompleted at St. Vincent’s Hospital inSydney, Australia, in June 2016. n
Resident Education FundOHNS Runs theRagnar RaceThe Ragnar Relay Series (namedfor Ragnar, a king and hero ofearly 9th Century Scandinavia)has grown from a single 188 milerelay from Logan to Park City,Utah in 2004 to the largestovernight running relay series inthe nation. On October 23-24,2015, a 12-person OHNS team rana grueling but gorgeous 197-mileRagnar Race in NorthernCalifornia. Molly Naunheim, MD,a PGY-3 OHNS resident, ledthe team and describes herexperience:All of our 12 participants committed toup to 36 hours for the race. We ranFriday day and through the night, andthen through the next day. Each runnercompleted three legs of between threeand 13 miles each, so after runners#1 through #12 completed their firstlegs of the race, runner #1 would startagain and the sequence was repeatedthree times.The route took us from San Francisco,up into the Marin Headlands, and endedin Calistoga, in California wine country.We ran among beautiful vineyards; wehad incredible views; and the scenerywas just magnificent.In a Ragnar Race, the team of 12is split into groups of six, who traveltogether in a van. Each group is incharge of dropping a runner off andmaking sure that that they pick up therunner who is just completing their leg.At that checkpoint the first runner transfersa slap bracelet to the new runner.Each group also provides “vansupport,” where the van pulls to theside of the road at an unexpected placealong the route to cheer for their runnerduring their leg and then drives on tothe next checkpoint. At night, becauseyou are running in near darkness,it’s important to wear reflective vestsand LED lights. It can really feel lonelyout there – in wine country, prettymuch by yourself, in the dark. Butseeing your van ahead on the side ofthe road and hearing your teammatescheering (despite the fact that it is4:00 a.m.) really pushes you forward.Organizing the OHNS teamIt takes a lot of time and logisticalcoordination to allow for six OHNSresidents to be away from the hospitaland make sure that there is still sufficientcoverage. But I figured 2015 was theyear, and everybody signed up and hada great time. In addition to myself, oursix residents included Drs. Dan Faden,Conor McLaughlin, Sean Alemi, PhilPerez, and Eric Formeister. Roundingout our team of 12 were facultymembers Drs. Steven Pletcher andChase Heaton; nurse practitionerShauna Brodie; graduate medicaleducation administrator Joanna Times;and friends of the department, RachelBaum and Sam Rowen.A unique eventThe race was a great opportunity tobuild department camaraderie in a newway. Part of me was worried becausewhen you aren’t running you arespending 36 hours, sweaty, in acramped van. Although the residentsall knew each other well, some of theother team members don’t know eachother that well. Luckily, everyone reallyenjoyed themselves as there is plentyto do between runs. All the teamsdecorate their vans, for example. Wehad markers listing everyone’s name andnickname, along with three boxes sothat after each runner completed a legof the race, a box got checked off.When the race was over, all boxes werefilled and the vans were covered inwriting. It turns out, when you are notrunning, you are certainly occupied bycheering on team members and rushingto the next checkpoint. Everyone wasenthused, sleeping when we could, butdedicated to getting up and cheering onthe next runner.Raising fundsMany of us residents would like to go onglobal missions – for example to fix cleftlips and cleft palates or perform chronicear surgery. Because those trips areoften paid for out of the residents’ ownfunds, we wanted to create a residenteducation fund. So, any money raisedfrom the Ragnar Race was to bedesignated for resident education in thefuture. Dr. Pletcher helped me arrangefor pledges of 1.00 per mile fromOHNS alumni and current departmentmembers.I’m happy to report that our officialfinish time was 28 hours and 24 minutes.Thanks to everyone who supportedthe team, we raised 4,158 for theeducation fund! nHeadsUp! Spring 20167
Nonprofit Org.U.S. PostagePA I DSan Francisco, CAPermit No. 8285Otolaryngology Head and Neck Surgery2233 Post Street, UCSF Box 1225San Francisco, CA 94115A D D R ES S S ER V I C E R E Q U EST EDUpcoming EventsThe Annual Francis A. Sooy, MD LectureshipJune 18, 2016, 7:30 am–NoonMission Bay Hospitals, William & Susan Oberndorf AuditoriumSpeaker: Kathleen Sie, MD, FACS, University of WashingtonThe Roger Boles, MD LectureshipSeptember 15, 2016, 5:00 – 6:45pmLocation to be determinedSpeaker: Bevan Yueh, MD, MPH, University of MinnesotaSooy Society Alumni Reception at the AAO/HNS Academy MeetingSeptember 18, 2016, 6:00-8:00 pmSan Diego Yacht Club, 1011 Anchorage Lane, San Diego, CASialendoscopy / Salivary Duct Surgery Cou
Integrated Health Care Practitioner Team Benefits Patients T he UCSF Otolaryngology - Head and Neck Surgery department's diverse clinician team comprises Physician Assistants (PAs) and Nurse Practitioners (NPs), who work collaboratively with department faculty physicians to provide excellent patient care. "We are fortunate to have recruited