Transcription
AnnualReport2014/15Report & Consolidated Financial Statements
Providing vital careto patients and familiesliving with terminal illnessacross Birminghamand Sandwell2
ContentsCHAIRMAN’S STATEMENT5VISION AND VALUES9REPORT OF THE TRUSTEES11WHAT OUR SUPPORTERS SAY ABOUT US33INDEPENDENT AUDITOR’S REPORT41CONSOLIDATED STATEMENT OF FINANCIAL ACTIVITIES42COMPANY STATEMENT OF FINANCIAL ACTIVITIES45CONSOLIDATED BALANCE SHEET48COMPANY BALANCE SHEET49CONSOLIDATED CASHFLOW STATEMENT50NOTES TO THE FINANCIAL STATEMENTS51LEGAL AND ADMINISTRATIVE INFORMATION67ANNUAL REPORT 2014 / 2015Birmingham St. Mary’s Hospice Limited3
statementfrom the Chiefexecutive andchairman4
Annual Report of the Trusteesof Birmingham St Mary’sHospice for the year ended 31March 2015The calibre and compassion of our staff andvolunteers is central to the quality of the serviceswe provide and to the Hospice’s reputation. Puttingpatients and families first is right at the top of ourvalues; our Annual Report sets out the many tangibleachievements that demonstrate this commitment.We are incredibly proud of everyone’s efforts towardsmaking significant improvements within a changingand challenging economic climate.Care at homeBirmingham St Mary’s Hospice is more than abuilding; we offer many services in a wide numberof settings including our inpatient provision withinthe hospice; delivering care in our patients’ ownhomes; and through our Education programmes.As well as our bespoke courses, our Educationprogramme includes the building of expertise in otherorganisations as an integral part of the Hospice’sservice delivery, working alongside other health andsocial care professionals including prison, care homes,hospitals and mental health services across the NHSand the community.Growing demands on Hospice careThese include the opening of our Family Centre on theInpatient Unit in May 2014, with a grant from HelpHarry Help Others and NHS England; the upgradingof our oxygen supply facilities on our Inpatient Unit;producing a child bereavement leaflet “The GroundFeels Wobbly” to help families support childrenthrough the loss; and an increase in volunteer roles,including recruitment of more Volunteer BereavementWorkers and Volunteer Ward Assistants.Recent projections forecast that the local populationaged 85 and over is likely to grow by 30% in the next10 years, with a growing range of physical, social andmental health conditions. Studies also show thatthe majority of people would prefer to die at home.Research by the Aston Research Centre for HealthyAgeing shows that risks associated with isolation aresignificantly greater across parts of Birmingham. Thiswill all increase demand for Hospice care.A grant from the Connie Taylor Trust Fund hasallowed us to establish a Research partnership withthe University of Birmingham. This has enabled usto participate in national research to remain at theforefront of symptom management and care ofpatients, families and carers.Over the past year we have had an increase inreferrals of 6.5% across all Hospice services, inparticular to our Hospice at Home and CommunityPalliative Care Teams. We also recognise the growingneeds of younger people living longer with terminalillness. This affirms our ongoing priorities to makeit easier for people to reach us and for the Hospiceto provide more care at home as we plan ahead to2020.Partnership, volunteering and new communityinitiatives have also extended our reach throughawareness raising and continuing to build capabilitiesin other settings.ANNUAL REPORT 2014 / 20155
FundingGovernanceThe growth in demand comes at a time when weface greater constraints and competition for funding.In the Five-Year Forward View for the NHS, ChiefExecutive, Simon Stevens, identifies three options toreduce and even close the 30 billion gap betweenNHS funding available and what patients will needby 2020/21. This creates a range of new scenariosfor hospice care nationally and locally. Whilst ourlocal NHS funding has reduced year on year, we weredelighted to secure confirmed funding for our Hospiceat Home service which is invaluable in supportingpatients safely at home in the last weeks of life anddemonstrates the value of integration with primarycare and community services. Most of our funding isthrough voluntary giving; legacies remain a valuableand important income stream, yet trends suggestthey will become less predictable in the future and weare already experiencing that impact.Building on the success and efforts of Judi Millward,who stepped down after 10 years as Chairmanthis year, we continue to strengthen our Boardthrough new appointments and are pleased towelcome Denise McLellan and Sarah Mitchell asnew Trustees. This year we have also taken a freshlook at Governance to ensure we remain fit for thefuture, continuing to create a Board environmentthat supports our duty of candour, with transparentassurance on the safety and standards of care,financial reporting and organisational performance.In response to these challenges, and to protectservices against uncertainties, we have implementeda new change programme. This aims to create theright balance and blend of affordable services andinnovations in income generation, to meet the growingneeds of our population, and to put the hospice in astronger financial position for the future. We haveadopted a set of principles to guide the process ofinnovation and change: safe, compassionate care topatients, families and carers; wellbeing of staff andvolunteers; job security and highest standards.Thank you to our supportersWe thank our whole community and all the individuals,trusts and foundations, companies and groups thatsupport us. Birmingham is an incredible, diverse,international city; the generosity and enthusiasm of allour supporters has been instrumental in BirminghamSt Mary’s Hospice continuing to deliver high qualitycare.It is a privilege to work with our dedicated andinspirational team of staff and volunteers; we thankyou for all your ongoing commitment and the manyachievements set out in this report.Mr Vij Randeniya OBEChairman of the TrusteesMs Tina Swani MBA, MCIMChief Executive6
ANNUAL REPORT 2014 / 20157
VisionandValues8
VisionOur vision is for a future where the best experience of living is available toeveryone leading up to and at the end of life.We continually strive to achieve this through the specialist and practical rangeof services we offer to individuals, families and carers; through education andpartnerships; and through working with professionals and communities to share ourexpertise and learn from others.Our shared valuesAt Birmingham St Mary’s Hospiceour patients and their familiescome firstWhat we do—— Listen & learn—— Make a difference—— Build trust & confidence—— Open minds & challenge myths—— Work together to achieve moreWhat we are— Honest & accountable— Open minded & flexible— Safe, specialist & sensitive— Person focused & positive— Innovative & forward thinking— Collaborative & inclusive— Empowering & enablingANNUAL REPORT 2014 / 20159
10
IntroductionThe Trustees, who are also Directors of the Companyfor the purposes of the Companies Act, submit theirAnnual Report and audited Financial Statementsfor the year ended 31 March 2015. The Trusteeshave adopted the provisions of the Statement ofRecommended Practice (SORP) “Accounting andreporting by Charities” (Revised) in preparing theAnnual Report and Financial Statements of theCharity. Birmingham St Mary’s Hospice is the brandname of St Mary’s Hospice Limited.Aims of the CharityThe Memorandum of Association sets out the aimsof the Hospice as the relief of suffering for those inneed of palliative care through serious illness, withoutintention to shorten life.The Trustees have considered the CharityCommission’s guidance on public benefit. TheTrustees believe this charity provides a public benefitby offering palliative care to adults who are residentwithin and around its catchment area of the cityof Birmingham and the neighbouring borough ofSandwell, and who are living with a terminal illness.Individuals, their carers and families, access ourservices by means of referral by their GP, DistrictNurse, hospital consultant or Clinical Nurse Specialist.Our services are developed with local communitiesto respond to the individual and diverse needs of ourpopulation. The Hospice’s services are free of chargeto patients and their families.ANNUAL REPORT 2014 / 2015We aim to provide relief to individuals living withterminal illness by:—— Developing and maintaining hospice basedservices and providing support in people’s ownhomes—— Promoting, encouraging or assisting researchinto the care and treatment of palliative care andrelated conditions—— Promoting, encouraging or assisting in theeducation and training of doctors, nurses,physiotherapists and other health and social careprofessionals—— Providing or assisting in the provision of spiritualsupport and guidance—— Providing support for carers and families of ourpatients.The Trustees believe that the quality of the caredepends on having a skilled and resourced workforceof paid and voluntary workers with access toappropriate training and development.The Hospice aims to ensure that it is recognisednot only as a leading provider of high qualitycompassionate care at end of life, but also as acentre of excellence for the provision and promotionof education, training and research for health andsocial care professionals in palliative care.11
What We DoSignificant activitiesDay HospiceThe Charity’s services are delivered through theInpatient Unit, the Day Hospice, Community PalliativeCare Team (CPCT), Hospice at Home Team, Familyand Carer Support Team (FACST) and the EducationDepartment. These are supported by the Finance,Income Generation and Marketing, Facilities,Information Technology Services, Governanceand Human Resource Departments. We also runcommunity engagement initiatives that influence thewider healthcare economy including our PalliativeCare Futures Forum and Compassionate CommunitiesProgramme.The Day Hospice is staffed by a Lead Nurse,Registered Nurses, a Therapeutic Activities Coordinator and nursing assistants, supported by ateam of four to six hospitality volunteers and cohort ofvolunteer drivers each Thursday. The Day Hospice alsohas input from physiotherapy, occupational therapy,the medical team and Family and Carer SupportTeam.Inpatient UnitThe Inpatient Unit has 25 beds in a mixture of multibedded wards and single rooms. There is also theHarry Moseley Family Centre which enables partnersor family members to stay at the Hospice.The Unit is staffed by a Lead Nurse, full and parttime registered nurses and nursing assistants, anAdmission/Discharge Nurse, a medical team andadministrative support. The medical team is led bya Consultant in Palliative Medicine, (who is also theHospice’s Medical Director), and includes a furthertwo part time Consultants in Palliative Medicine,supported by a ward based Speciality Doctor. Thereare up to four junior doctors working with the team atany one time in both General Practice and PalliativeMedicine training posts.Patients have access to physiotherapy, occupationaltherapy and pharmacy advice supplied under aService Level Agreement with University HospitalBirmingham NHS Foundation Trust. They are also ableto enjoy massage treatments given by the Hospice’steam of voluntary Complementary Therapists.12Day Hospice supports up to 20 patients a day andoffers supportive symptom management by way ofgroup education activities, exercise and relaxation.There are diversional, therapeutic activitiesthroughout the day. Patients are able to receivetransfusions of blood products and intravenous drugtherapies in Day Hospice.Patients who attend the Day Hospice have beenassessed by the Community Palliative Care Team andare living at home and referred into Day Hospice for12 attendances.Community Palliative Care Team (CPCT)The CPCT consists of a Team Leader and ClinicalNurse Specialists (CNS) with extensive clinicalexperience in specialist palliative care-working in thelocal community. A 24-hour service is offered by theteam, with one of the Clinical Nurse Specialists oncall during the out of normal working hours period,at weekends and bank holidays to provide holisticspecialist advice and support to patients, families andother health care professionals.Each CNS has a complex patient caseload andprovides specialist input to allocated GP practices andDistrict Nursing teams in Birmingham and Sandwell.They visit patients in their homes offering advice andsupport, and work closely with the patient’s GP andother members of the multidisciplinary communityteam.
Members of the CPCT also have an educational roleand frequently have medical and nursing students onplacement with them. The CNS role includes deliveryof training programmes at the Hospice, at localuniversities and within the acute setting alongsideparticipation in audit and research.Hospice at Home TeamHospice at Home started in January 2013, and is nowin its third year, the team continues to reach morepatients. Hospice at Home aims to care for peoplewho are at the end stage of their illness and haveexpressed a wish to die at home.Post-bereavement support is part of the Familyand Carer Support Team, and continues to beprovided by the Bereavement Services Coordinator and a specially trained team of VoluntaryBereavement Workers. This model is proving to beextremely effective and training and recruitmentare undertaken regularly. Support is also offered topeople in their homes.The team also has a part-time chaplain, who is partof a wider multi-faith chaplaincy team.The Hospice at Home Team consists of a Lead Nurse,three Registered Nurses and three HealthcareAssistants experienced in palliative care as well as ateam of bank nurses.The Hospice at Home Team provide a completepackage of care in peoples own homes in partnershipwith Birmingham Community Healthcare NHS Trustand Sandwell, working alongside GP’s, District Nursesand other care providers. The service also helpspeople avoid crisis that could lead to unwantedhospital admissions and aims to ensure a timelydischarge of patients in hospital who are nearing theend of their lives and wish to be cared for at home.Family and Carer Support Team (FACST)The Hospice Family and Carer Support Team providea variety of services to meet the social, emotional andspiritual care needs of patients and relatives. Theteam consists of qualified social workers who providea range of services from financial and practicalsupport, assistance with housing and grants, andliaison with other statutory and voluntary agencies.It also provides much needed emotional supportto families and children. The team runs projectssuch as carers’ education groups, compassionatecommunities and diversity work across Birmingham,reaching minority groups to enable them to accessHospice services more effectively.ANNUAL REPORT 2014 / 201513
Medical TeamPalliative Care Futures ForumThe Medical Team supports the four key Hospiceservices providing 24 hour cover for all clinical areas.There are reciprocal working arrangements in placewith the Consultant at the Queen Elizabeth Hospital,meaning that Hospice Consultants offer one clinicalsession a week at the Hospital to support the hospitalmultidisciplinary team meeting. These professionalsalso work collaboratively to provide an out-of-hoursadvice service to University Hospitals Birminghamand the community. As with all other clinical teams italso supports the Hospice education programme. Inaddition, the team organises and hosts BirminghamUniversity Medical Student academic study days andHospice placements.This cross sector Forum was established by theHospice in order to address inequalities at the endof life and to ensure that local advancements arelinked to regional and national policy development inpalliative care. The Forum held 2 key events over theyear, setting the agenda for collaboration betweenthird sector, NHS, local government and commercialhealth and social care providers. Task and finishgroups have been created to address specific issuesand opportunities and translate national policy inorder to influence better local outcomes.EducationThe Hospice’s Strategic Plan reiterates a commitmentto education, not only for its own staff and volunteersbut extending to other health and social careprofessionals and service providers. The ultimateaim is to support the enhancement and continuingdevelopment of end of life care throughout the widercommunity and have a positive effect on patientoutcomes.For Hospice staff and volunteers’ education andpersonal development initiatives will continue to besupported by a performance review system. TheHospice’s training and development policy aims toensure all staff and volunteers have fair and equal‘access to development opportunities.Developing a Strategy for a Research ActiveHospiceA palliative care consultant has been designatedas ‘Research Champion’ to provide two protectedresearch sessions a week for two years. In additiona senior lecturer has been supported by the localUniversity to work with the hospice to developresearch. Together they have devised a researchstrategy to guide the development of researchactivity in the Hospice.14As part of this initiative the Hospice celebratedWorld Hospice Care Day and World Mental HealthDay with a workshop in October 2014. Mental healthservice users, supporters, and organisations metwith palliative care service providers and communitygroup representatives to explore ways of workingtogether to make the end of life journey for peoplewith pre-existing mental health diagnoses moresupported.Compassionate CommunitiesCompassionate Communities is a Public Healthapproach to end of life care. It encouragescommunities to support people and their families whoare living with a terminal illness or living with loss andit aims to enable all to live well within communitiesto the very end of life. Compassionate Communitiesrepresentatives’ support wider initiatives such as thePalliative Care Futures Forum.
Structure, Governance & ManagementThe Articles of AssociationThe Articles of Association is the governing documentthat sets out rules and requirements relating to votesof Association Members; terms of office and electionof Trustees and Honorary Officers; disqualification ofTrustees; and proceedings of the Board.The membership of the Association is currently 63,with provision for up to 100 members. All Trusteesand Non-Executive Directors of the Hospice, itsCharitable Trust Fund and Trading Company,are required to be members of the Association.Association Members are appointed following openrecruitment or open evenings, followed by interviewwith an appointments panel of Trustees, AssociationMembers and Executive Directors. This will include theChairman and Chief Executive.Board of TrusteesThe Board of Trustees (the Board) is the governingbody of the Hospice. The purpose of the Board is toensure the Hospice is able to fulfil the objectives in thegoverning documents, that the organisation complieswith charitable and company law and that the values,philosophies and reputation of the Hospice areupheld. The approach of the Board is also to supportthe Executive Team in carrying out their executiveresponsibilities. There is a clear understanding of thedistinction between Governance and Management.There may be up to 15 Trustees on the Board (with aminimum quorum of five). The Board is the employerof all Hospice staff. The Board meets once everytwo months and is the final decision-making bodyfor new policy, strategic planning and approval offinancial budgets. The Board is also responsible formonitoring the implementation of the strategy andfinancial activity. The Hospice Chief Executive andExecutive Directors attend Board meetings but do nothave voting rights. Trustee and Director Indemnityinsurance was provided for the year at an annual costto the Hospice of 617 with a limit of indemnity of 1million.ANNUAL REPORT 2014 / 2015A maximum of two staff or volunteer observers mayattend each Board meeting by prior arrangement.Appointment of TrusteesAppointment of Hospice Trustees may either be byelection by the Association at the Annual GeneralMeeting or co-opted by the Board. There is a termof office of 3 years following which there may bere-election by the Association. The number of reelections is not limited although this is currently beingreviewed.Trustees are appointed following a recruitmentprocess which may include advertisement followedby an introductory open evening. An expression ofinterest form and Curriculum Vitae is requestedfollowed by interview with an Appointments Panelof Trustees, Association Members and ExecutiveDirectors. The panel will include the Chairmanand Chief Executive. References are taken andappropriate suitability checks are made prior toappointment, as Trustees may be given power ofinspection.Through active recruitment the Hospice has recentlyappointed a new Chairman and two new Trustees.Induction and training of Trustees andAssociation MembersTrustees and Association Members have a coreinduction programme supported by bespokeinduction activities depending upon their role. AllTrustees now have Information Governance trainingas they are encouraged to participate in providervisits. There are brief trustee training sessions prior toat least 2 Board Meetings a year and an annual AwayDay of Trustees and Executive Directors. In May 2015this focused on the development of the Hospice’sEducation and Research Strategy.15
Strategic Leadership & Governance FrameworkThe Chief Executive is responsible for the leadershipof the Hospice, which involves assisting the Boardin determining the strategic vision and plans for theHospice, and for ensuring effective achievement ofthose plans. The Chief Executive and Executive Teamalso ensure that Trustees are actively engaged inexercising their accountabilities and assure effectiveand transparent governance across the wholeorganisation. This is provided through a leadershipand governance framework of which there is a corestructure:LeadershipExecutive TeamThe Executive Director Team comprises:—— Chief Executive—— Medical Director & Consultant in Palliative Medicine—— Director of Nursing—— Finance Director—— Commercial DirectorMeeting fortnightly this team is engaged at looking atthe wider strategic implications of changes that affectthe charity sector and the operational environment.Executive Directors have powers to make decisionswithin the approved budget, operational plan andhospice policies and procedures, including StandingFinancial Instructions which set out delegatedauthority for financial decisions. Finance Committee(within given limits) or Board Authority is requiredfor investment or service changes outside theseparameters.The Executive Directors have specific responsibilitieswithin the Grievance and Disciplinary procedures.16Business Development TeamThe Business Development Team comprises the ChiefExecutive, Executive Directors, and key managersacross Hospice departments. The purpose of theBusiness Development Team is to develop anddeliver strategic and operational plans as well asimplement and manage change. This includes takingforward the Hospice’s Equality and Diversity priorities.Leadership development takes place at the 6-weeklymeetings to develop consistency and confidence ofleadership practice. This is augmented by a largervirtual Leaders’ Communication Forum to ensure allstaff in key and supervisory positions receive timelyinformation.Open ForumEvery 6 months, an Open Forum is held for staffand volunteers to receive updates and to engagein discussion about plans and ideas. Where thereare more significant changes being plannedor implemented, the Open Forum is held morefrequently.GovernanceFinance CommitteeThe Finance Committee is a sub-committee of theBoard, Chaired by the Honorary Treasurer. ExecutiveDirectors are members of the Finance Committee.The Committee meets bi-monthly between BoardMeetings and has delegated decision makingauthority from the Board.The purpose of the Committee is to monitor thestrategic, financial and operational planning of theHospice and for decisions on Executive Director andChief Executive remuneration.
Governance CommitteesThe Executive Team is responsible for managingquality and risk through four Governance Committeesensuring that courses of action are taken to minimiseand remedy identified risk and poor performance,and that systems are in place to share good practiceand continually improve the quality of care, clinicaleffectiveness and leadership across the Hospice.Each committee has authority to approve policies,which are then ratified by the Board. The committeesmake recommendations to the Board. Eachcommittee meets at least once a quarter.The Governance Committees are:—— C ompliance Committee (Health, Safety,Environment, Risk, Information Governance)—— Clinical Governance Committee—— HR Committee—— Premises Committee.St Mary’s Hospice (Trading) Ltd(“the Trading Company”)The Trading Company is a wholly owned subsidiaryof the Hospice. There are seven directors who haveaccountability for retail and other trading andcommercial activities. The Hospice Chief Executivehas ultimate responsibility for the management of theHospice and Trading Company. Four of the currentdirectors are Hospice Trustees. The Finance Director,the Commercial Director and the Head of Retailattend the Board meetings, which are held once everythree months.The Trading Company owns a one third share of theequity of TLC Lotteries Ltd (TLC). This company is ajoint venture between the Hospice, Acorns Children’sHospice and Birmingham Focus on Blindness. TLC ismanaged by a Lottery Manager. The TLC Board ofDirectors comprises two representatives from eachof the three charities. The Hospice representativesare a Trading Company Director and the CommercialDirector. TLC is a decision-making organisation unlessTrustee approval is required from any of the ownercharities.The committees are chaired by an Executive Directorand attended by at least one Trustee or AssociationMember with relevant expertise.Associated Trust Fund& SubsidiaryThe St Mary’s Hospice Charitable Trust FundThe Charitable Trust Fund is a registered charitywhich has the purpose of managing the investmentfund for the Hospice. During the year ended 31 March2015 there were five Trustees, three of whom arecurrently Hospice Trustees. Meetings are held once aquarter, with a quorum of two Trustees. The HospiceChief Executive and Finance Director attend withthe Investment Manager from Quilter Cheviot, in anadvisory capacity.ANNUAL REPORT 2014 / 201517
StrategicReport18
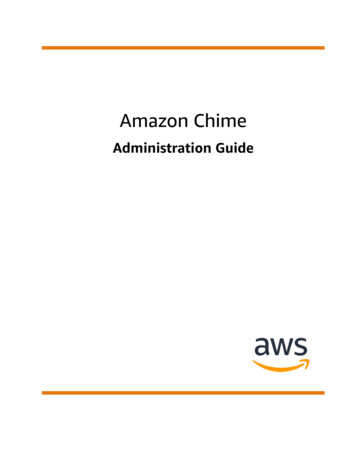
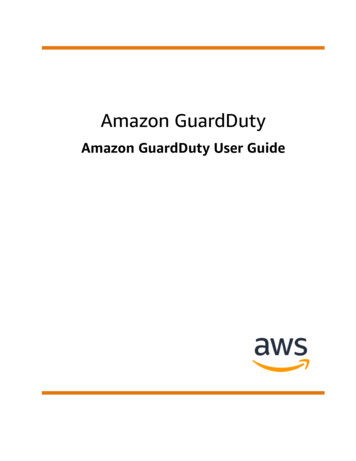
Overview of Financial Performance for the YearThere was a consolidated deficit before investment gains of 788,000 for the year.A deficit of 116,000 on restricted funds further added to the deficit of 672,000 onunrestricted funds. Expenditure increased by 332,000 (4%), but incoming resourcesdecreased by 634,000 (9%) compared with the previous year, due to a significantreduction in legacy income.Realised and unrealised investment gains totalling 172,000 reduced the deficit resulting in a net‘decrease in funds of 616,000Charitable activities consisting of Inpatient Services,Community Palliative Care, Day Hospice, Hospice atHome service and Education accounted for 74% ofexpenditure for the year.Only 47% of total incoming resources were generateddirectly by these charitable activities, and thereforethe Hospice continues to rely on fundraising andtrading activities to help sustain its core services forpatients and their families.Income ,0001,500,0001,000,000500,0000Donations& GiftsANNUAL REPORT 2014 / 2015LegaciesNationalHealthServiceFundraisingEvents &AppealsTLCLotteriesFundingTradingActivities &EducationInvestmentIncome19
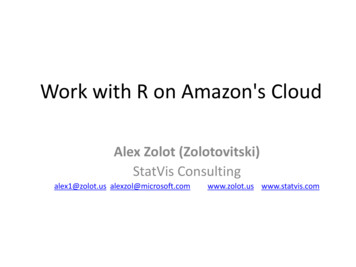
1%5%16%15%2%Principle sourcesof funding14%47%KEY20Fundraising Events & AppealsDonations & GiftsTl c Lotteries Fund ingLegaciesTrading Activities & EducationNational Health Service GrantsInvestment Income
Principle Sources of Funding 15%-42% 2%Donations and giftsLegaciesNational Health Service grantsThe Hospice was pleased toreceive donations and gifts of 358,000 during the year, anincrease of 15% over theprevious year.Income of over 1,022,000 wasreceived from gifts generously leftby supporters in their wills. Whilstthis was a decrease of 752,000(42%) year on year, it represents14% of the Hospice’s total funding.Bequests remain vital to theHospice’s continued financialviability, and sincere thanks aredue to all those people who haveremembered the Hospice in thisway during the year.Income received from the NHSincreased by 64,000 (2%) to 3.2 million, representing 45% oftotal group income. This is dueto funding being received for theHospice at Home service for thefull year, whilst the remaining coreNHS funding was subject to afurther 1.9% deflator.ANNUAL REPORT 2014 / 2015The costs of the clinical servicesthat the NHS grants help to fundincreased by 106,000 (2%) overthe last year.21
-8%Fundraising events & appealsFundraising events and appealsgenerated income of 912,000,including 295,000 restrictedfunding. This was 83,000 (8%)lower than the previous year,which had included 214,000of restricted funding. The costof generating voluntary incomewas 111,000 (12%) more than inthe previous year as the Hospicecontinued to invest in fundraisingplans to increase publicawareness of its services andgenerate voluntary income fromnew sources.A variety of successful eventswere held including the Light upA Life appeal which generatedalmost 65,000 for the Hospice,the Moonlight Memories Walk( 24,000) and the GreatBirmingham Run. Other challengeevents, collections and supporterled activities that provide essentialrecurring funding for Hospiceservices were also undertaken
St Mary's Hospice continuing to deliver high quality care. It is a privilege to work with our dedicated and inspirational team of staff and volunteers; we thank . Chairman of the Trustees Ms Tina Swani MBA, MCIM Chief Executive. ANNUAL REPORT 2014 / 2015 7. 8 Vision and Values. ANNUAL REPORT 2014 / 2015 9 Vision Our vision is for a future .

![Index [beckassets.blob.core.windows ]](/img/66/30639857-1119689333-14.jpg)