Transcription
Adverse Event Analysis: A Staff TrainingExercise9/6/2016September 8, 2016Adverse Event Analysis:A Staff Training Exercise 2016 EC RI I N S TI TU TEOur Office Team Office managerElectronic health record (EHR) liaisonClinic nurse (Julie Williams)Clinic medical director (Dr. Mary Downs)2Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE1
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Learning Objectives To understand the steps of event analysis:1.2.3.4.5.Identify eventConduct investigationAnalyze dataIdentify root cause and contributing factorsDevelop action plan 2016 EC RI I N S TI TU TE33Key DefinitionsAdverse event: An undesired outcome or occurrence, notexpected within the normal course of care or treatment,disease process, condition of the patient, or delivery ofservices Near miss: An event or situation that could have resultedin an accident, injury, or illness but did not, either bychance or through timely intervention Root cause analysis*: A structured method used toanalyze adverse events or near misses to identifyproblems and decrease the risk of future errors *Agency for Healthcare Research and Quality. Root cause analysis. PSNet July -cause-analysis.4Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE2
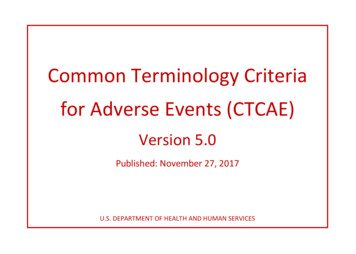
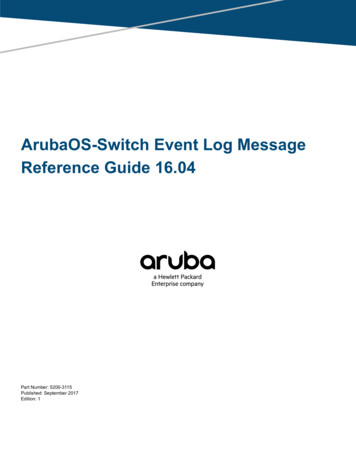
Adverse Event Analysis: A Staff n5 2016 EC RI I N S TI TU TE5PhasesEvent Investigation and Analysis MethodologyI. Notification/Immediate/Interim ActionII. InvestigationIII. AnalysisIV. ActionPlanningV. MonitoringSTARTNotification ofeventYesRCA?YesInitiateInvestigationAnalyze dataIdentify n PlanMonitor andmeasurepreventativeactionsImmediate/Interim actionsfor PatientSafetyNoActionseffective?NoEnter event into database fortracking and trending of:-Chronic events-Event characteristics-Root CausesYesReport findingsRCA Process StepEnd6Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE63
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Identification of Event The immediate response to an adverse event is to ensurethe patient is safe and to alleviate any untoward effectsof the event 2016 EC RI I N S TI TU TE7Identification of Event All adverse events and near misses should be reportedimmediatelyAll adverse events and near misses should be reportedusing a uniform procedure Who is supposed to report the event/near miss? What form should be used? When should the report be completed? Who is supposed to get the incident report?Timely and accurate reporting is the basis of effectiveresponses8Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE4
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Systems ThinkingRoot cause analysis seeks to identify systemic orindividual problems that contribute to an event These causes go deep enough to reveal the systemissues underneath Once root causes are identified, they point tovulnerabilities and fixes at a systems level The fixes at systems level can prevent recurrences 2016 EC RI I N S TI TU TE9Common Pitfalls Investigation not thoroughly done beforeanalysis is attempted Analysis stops short of actual rootcauses Root cause is often identified as “theperson” or human error Root causes not tied to corrective actionplans that were identified Action plans focus on education of theperson or persons Action plans not measured foreffectiveness10Copyright ECRI Institute, 2016If we don’tget to therootcauses Then ouractionplans won’tfix thesystemicproblem 2016 EC RI I N S TI TU TE105
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Case Scenario Dr. Smith sees a female patient with complaints of nasalcongestion and watery eyes. Dr. Smith prescribes Flonasenasal spray and orders a sinus CT scanWhen ordering the prescription in the EHR, she types“FLO” in the medication order screen and the EHRautomatches Flomax, a medication for an enlargedprostate that is not approved by the Food and DrugAdministration for womenWithout noticing the error, Dr. Smith selects the incorrectmedication 2016 EC RI I N S TI TU TE11Case Scenario (cont.) The patient fills the prescription and takes it as directedFlomax also has a side effect of hypotension. Severaldays after beginning the medication, the patient presentsto the emergency room (ER) with dizziness and the erroris discovered12Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE6
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Case Scenario (cont.) The patient returns to the health center as directed bythe emergency roomDr. Smith examines the patientResults of sinus CT scan are not availableDr. Smith leaves for vacation 2016 EC RI I N S TI TU TE13Case Scenario (cont.) Radiology calls the health center with abnormal CTresultsReceptionist writes the telephone report down and placesit in Dr. Smith’s inboxResults of abnormal sinus CT scan are also emailed to Dr.Smith’s portal. Assigned covering provider for Dr. Smith isunaware CT results are pending for the patientDelayed follow-up to the CT scan report for a sinus mass;rule out squamous cell carcinoma14Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE7
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Investigation 2016 EC RI I N S TI TU TE15Gather Information Physical evidence—locate, separate, investigateInterview—involved parties, witnesses, others withinformation16Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE8
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Physical Evidence Office medical record, ER medical record Orders Diagnostic tests Lab results Visit summary Prescriptions Equipment, instructions, error codesStaff schedulesTelephone recordsPhotos, videos 2016 EC RI I N S TI TU TE17Interviews Interviews are one of the primary ways wegather evidence about an accident/incident They can be structured, semistructured, orunstructured They often involve a person (witness) tellinghis or her story18Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE9
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Interview TipsBe an active listener Be courteous andopen-minded Show limited emotion Don’t embarrass;reassure nervousinterviewees Look for bias, but do notinterrupt or criticize Keep interviewees onpointEncourage intervieweesto continue talking if theystate they “don’t knowanything” prematurelyEnsure interviews areprivate and conductedone on one 2016 EC RI I N S TI TU TE19IntervieweesOffice manager Dr. Smith (involved in the event) Dr. Miller (another physician in the practice) Dr. Downs (medical director) Nurse Adams (another nurse in the practice) EHR liaison 20Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE10
Adverse Event Analysis: A Staff TrainingExercise9/6/2016“The point of a human error investigationis to understand why actions and assessmentsthat are now controversial,made sense to people at the time.”— Sidney Dekker**Human factors and safety expert 2016 EC RI I N S TI TU TE21Sample Interview QuestionsCan you explain to me in your words what happened? Have you ever been in this situation before? Did you do anything different in this situation than youhave done before? Was there anything unusual about this visit or situation? Do you feel that when things don’t go right, you are ableto speak about it freely? Can you describe your decision-making process? Do you feel like you had adequate training in the EHR? 22Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE11
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Walk through the Event Good to elicit important detailsHelps probe staff perceptions (situational awareness) ofthe environmentHelps interviewee to sketch out a diagram/flowchart ofhow things happenedHelps remind the interviewees of event details they mighthave forgotten 2016 EC RI I N S TI TU TE23Look at Safeguards/Barriers Safeguards/barriers are things that have been set inplace to protect from harm, damage, or lossWhen investigating events/near misses/unsafeconditions, you must ask and seek to answer theseimportant questions: Was a safeguard present? How did each defense/safeguard fail? Why did they fail?24Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE12
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Are There Any Safeguards/Barriers?What shouldhaveoccurred: Physicianselects“FLONASE”Were any safeguards present ordid they fail? Is the drug highlighted or boldedin the list of choices to help theprovider know which drug isbeing selected? Is there a follow-up dosingscreen? Is there any alert fordiagnosis/drug matches ormale/female drug matches? Is there a pop-up screen toconfirm the medication beingprescribed? 2016 EC RI I N S TI TU TE25Are There Any Safeguards/Barriers? (cont.)What should have occurred: CT scan results shouldhave been forwarded toassigned coveringprovider when physicianwas absent 26Copyright ECRI Institute, 2016Were any safeguardspresent or did they fail?Is there a way to verifythat results are forwardedin cases of absences?What is the processregarding coverage whena provider is on vacation?Was there an errormessage after the lastupgrade? 2016 EC RI I N S TI TU TE13
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Putting the Investigation Together 2016 EC RI I N S TI TU TE27Develop a Timeline Based on data gathered and interviewsBe as specific and detailed as possibleBe sure to include precursor events28Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE14
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Simple TimelineMondayDr. Smith sees femalepatient with nasalcongestion and wateryeyesDr. Smith tells patient shewill prescribe FLONASEnasal sprayDr. Smith ordersprescription in the EHRfor FLOMAXPharmacy order sentelectronically to patient sretail pharmacyDr. Smith orders sinusCT scanPatient picks upprescription at retailpharmacyPatient goes to outpatientRadiology for CT scanPatient takes FLOMAX forseveral daysPatient returns toHealth CenterPatient seen by Dr. SmithCT scan report notavailableDr. Smith leaves forvacationReport placed in Dr.Smith s inboxCT report mass identifiedrule out squamous cellcarcinoma sent to Dr.Smith s e-patient listCT report not seen bycovering providerSundayPatient presents to ERwith complaints ofdizzinessWednesdayRadiology calls HealthCenter withabnormal CT report 2016 EC RI I N S TI TU TE29Analysis30Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE15
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Identify the Problem: The Problem StatementWhat happened? Who was involved? When did it happen? Where did it happen? Who was affected? How did it happen? 2016 EC RI I N S TI TU TE31Develop a Problem StatementThe problem statement does not contain the “Why?”“Why” will be discovered in the investigation32Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE16
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Problem Statement1.Incorrect medication was prescribed for the patient2.Recognition of abnormal sinus CT scan report wasdelayed 2016 EC RI I N S TI TU TE33Analysis Steps1.Identify and gather your root-cause analysis (RCA) team2.Analyze the data for causal factors3.Drill down to determine root causes4.Prioritize the root causes34Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE17
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Multiple Tools and Thorough AnalysisCan Help Identify Root CausesSwarm analysis 2016 EC RI I N S TI TU TE3535AnalysisBrainstormingBased on the idea that collective thinking is better thanindividual thinking alone No idea is out of the question; some ideas will trigger others Ideas generated will not be discussed or analyzed at thistime Ensure equal participation Document identified issues that are not related to the eventbut warrant attention at another time 36Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE3618
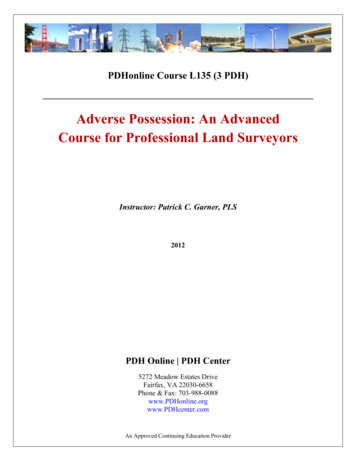
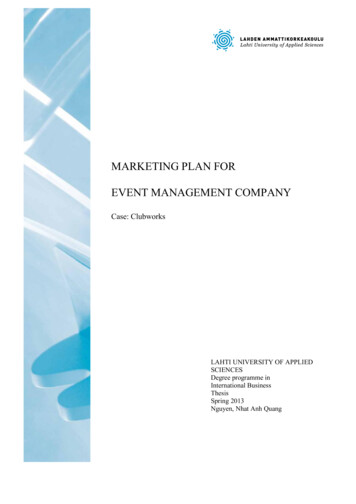
Adverse Event Analysis: A Staff TrainingExercise9/6/20165 Why’s Steps to Answering the 5 “Why’s”: Ask, “Why is this a cause of the originalproblem?” For each new answer to the question,ask “why” again. You will usually need to ask “why” 5times (it may be more or less, but it’susually 5). How do you know when to stop? Whenyou can no longer answer “why.” 2016 EC RI I N S TI TU TE375 Why’s Worksheet5 Whys Worksheet12Problem from worksheetIncorrect medication was prescribed for the patientWhy is that happeningProvider did not review the drop down listof all medications that started with “FLO”3Why is that?Provider assumed that the correctmedication was being prescribed4Why is that?Providers not cautioned about medicationautomatch in the EHR5Why is that?Root CauseProtocols or systems were not developed to requireverification of prescriptions to intended medicationsbefore sending prescription to the pharmacyAction38Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE19
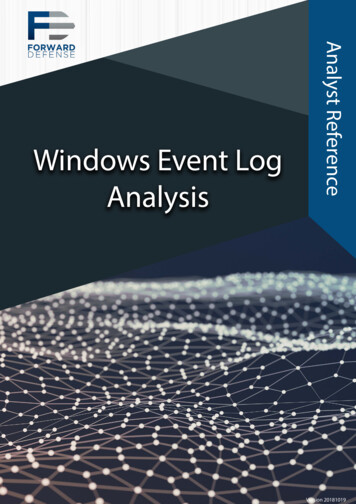
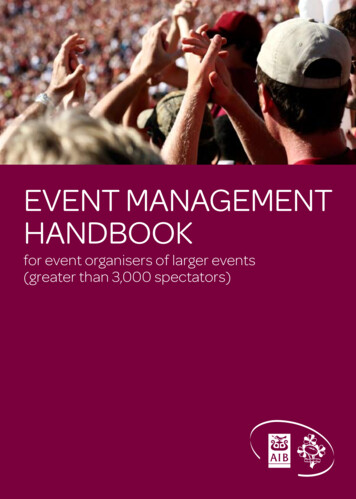
Adverse Event Analysis: A Staff TrainingExercise9/6/20165 Why’s Worksheet5 Whys Worksheet1Problem from worksheetRecognition of abnormal sinus CT scan report delayed2Why is that happeningRadiology report sent to ordering physician’sinbox but she was on vacationWhy is that?Dr. trained that in her absence test resultswould automatically default to assignedcovering provider for follow up34Why is that?Sinus CT scan did not automatically defaultto assigned covering provider5Why is that?Root CauseFollowing the last upgrade, automatic defaultmalfunctioned and was not reportedAction 2016 EC RI I N S TI TU TE39Identify Root Cause40Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE20
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Why Take Time to Identify Root Causes?If you don’t have time to find the root causes now,do you have time to reinvestigate similar eventsbecause the root causes were not identified and fixed thefirst time? 2016 EC RI I N S TI TU TE41Causal Factor ChainDr. Smith ordersprescription in the EHRfor FLOMAX42Copyright ECRI Institute, 2016Causal FactorCausal FactorRoot CauseRoot Cause 2016 EC RI I N S TI TU TE21
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Causal Factor ChainFrom problem toCausal factors toRoot cause 2016 EC RI I N S TI TU TE43Recognition of abnormalAbnormalsinusCTsinus CT scanreportscan reportdelayeddelayed44Copyright ECRI Institute, 2016Causal FactorCausal FactorCausalCausal FactorFactorRoot CauseRoot CauseRoot CauseRoot Cause 2016 EC RI I N S TI TU TE22
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Causal Factor ChainFrom problem toCausal factors toRecognition of abnormal sinus CTscan report delayedRadiology report sent to orderingphysician s inbox but she was onvacationDr. trained that in her absence test resultswould automatically default to assigned.covering provider s inbox to follow upSinus CT scan did notautomatically default to assigned.covering providerRoot causeFollowing the last EHR upgrade, theautomatic default malfunctioned and wasnot reported. 2016 EC RI I N S TI TU TE45What Have We Learned from this Process?Before TrainingAfter TrainingFocused only on the individualsinvolved?Look at the systems or workflow tohelp the individual (not blame theindividual).Decided that the pharmacy shouldhave caught the error?We can control and fix some of theprocesses or workflow. It is ourresponsibility to create safeguards inour office.Jumped into coming up with solutionsbefore thorough analysis?We need to take the time toinvestigate and analyze—even if ittakes multiple meetings.Analysis may not have gotten to theroot cause because we didn’t askenough “why’s”?Getting to the root cause will identifythe systematic issues to help preventfuture events.46Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE23
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Developing an Action Plan 2016 EC RI I N S TI TU TE47Actions Should Be Tied Directly to CausalFactors and Underlying (Root) CauseAdverse EventCausal FactorCausal FactorRootCauseActionActionCausal FactorCausal seAdapted from Vanden Heuvel et al. Root cause analysis handbook. 3rd ed.Houston (TX): ABS Consulting; 2008.48Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE24
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Sample Action ChainAdverse EventCausal FactorCausal FactorCausal FactorRecognition of abnormalsinus CTscan delayedRootCauseActionActionRootRootRadiology report sentCauseto orderingCausephysician’s inbox but she was onvacationActionDr. trained that in herActionabsence testresults would default to coveringprovider’s inbox to follow upCausal ActionActionCauseCauseSinus CT scan report did notautomatically default to assignedcovering providerFollowing the last EHR upgrade,the automatic defaultmalfunctioned and was notreported 2016 EC RI I N S TI TU TE49Root Cause and Action Plans Root Cause: Protocols or systems were not developed torequire verification of prescription to intended medicationbefore sending prescription to the pharmacy Hardwired pop-up in EHR requires the physician toverify that the prescription has been matched againstthe intended medications before sending theprescription to the pharmacy Updated protocol requires the provider to verify anddocument that the prescribed medications are correct Office-wide education on updated protocols50Copyright ECRI Institute, 2016 2016 EC RI I N S TI TU TE25
Adverse Event Analysis: A Staff TrainingExercise9/6/2016Root Cause and Action Plans (cont.) Root Cause: Following the last EHR upgrade, automaticdefault malfunctioned and was not reported Schedule IT to make the necessary changes in theEHR to ensure that the malfunction is fixed Investigate EHR tracking system to address issue Change the process for front desk and clinical staff onhow to handle diagnostic results and who to contactwhen provider is not in the building Educate providers and staff to “hand off” to coveringproviders 2016 EC RI I N S TI TU TE51Take-awayIdentifyEvent52Copyright ECRI Institute, ion Plan 2016 EC RI I N S TI TU TE5226
Adverse Event Analysis: A Staff TrainingExercise9/6/2016ECRI Institute Clinical Risk ManagementResources Event report ges/PSRM5.aspxEvent reporting /EventReportToolkit.aspxEvent response /EventResponseToolkit.aspx 2016 EC RI I N S TI TU TE53Questions?Clinical RM Program@ecri.org(610) 825-6000, x5200Thank You 2016 EC RI I N S TI TU TECopyright ECRI Institute, 201627
Enter event into database for tracking and trending of :-Chronic events-Event characteristics-Root Causes Monitor and measure preventative actions Report findings No Yes Yes Immediate / Interim actions for Patient Safety