Transcription
Management of Radiotherapy Patients withCardiac Implantable Electronic DevicesDaniel Bailey, PhD, DABRNorthside Hospital Cancer InstituteSeptember 2016
Quiz Question #1What is the safe radiation dose limit forimplanted cardiac pacemakers?1. 0.5 Gy2. 2 Gy3. 10 Gy4. No safe dose threshold2
Quiz Question #2Compared to pacemakers, implanted cardiacdefibrillators are:1. Less sensitive to radiation-induced malfunction2. More sensitive to radiation-induced malfunction3. Equally sensitive to radiation-induced malfunction4. Harder to spell3
Quiz Question #3Compared to older pacemaker models (e.g.discreet uni- or bi-polar transistors) modern CMOSpacemakers are:1. Less sensitive to radiation-induced malfunction but moresensitive to EMF interference2. More sensitive to radiation-induced malfunction but lesssensitive to EMF interference3. Equally sensitive to radiation-induced malfunction and EMFinterference4. Far less susceptible to the Vulcan Death Grip4
Quiz Question #4When treating a CIED patient with high-energyphotons (e.g., 18 MV), how is proximity oftreatment fields to the CIED related to risk ofradiation-induced malfunction?1. Linearly related2. Related by the inverse-square law3. Unrelated4. The same as the ratio of unicorns to leprechauns5
A series of CIED-related conundrums:where it all began
CIED literature is scattered and conflicting Number of CIED patients receiving radiationtherapy is steadily increasing7
CIED literature is scattered and conflicting8
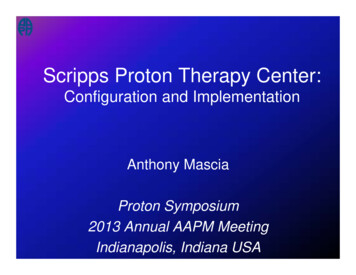
CIED issues motivating this study Number of CIED patients receiving radiationtherapy is steadily increasing Vendor literature concerning “safe” radiation doselimits for these devices is tedious and scattered9
Summary of doselimit recommendations from fourmajor CIEDmanufacturers10
CIED issues motivating this study Number of CIED patients receiving radiationtherapy is steadily increasing Vendor literature concerning “safe” radiation doselimits for these devices is tedious and scattered AAPM TG-34 (published in 1994) is outdated interms of current CMOS technology and doesn’tinclude tachycardia devices (i.e. implantable cardiacdefibrillators)11
12
CIED issues motivating this study Number of CIED patients receiving radiationtherapy is steadily increasing Vendor literature concerning “safe” radiation doselimits for these devices is tedious and scattered AAPM TG-34 (published in 1994) is outdated interms of current CMOS technology and doesn’tinclude tachycardia devices (i.e. implantable cardiacdefibrillators) Sometimes historical policies and/or physician’sinstructions have little to no basis in actual data13
Brief overview of CIED issues inexternal beam radiation therapy
CIED issues in EBRT Data on older, transistor-type CIEDs is basicallyuseless today Modern CMOS (complimentary metal-oxidesemiconductor) devices are less susceptible to EMFinterference but exponentially more sensitive toradiation-induced malfunction1– ICP/ICD: accumulation of positive charge carriers in siliconlayers leads to aberrant electrical pathways– ICD: RAM memory chip sensitive to radiation damage,especially in the presence of neutron dose15
CIED issues in EBRT Reports of CIED-malfunction in radiation therapy showpotential errors from doses as low as 0.15 Gy– Some of the exact same models showed no errors at all in directirradiation of up to 150 Gy Almost no reports of error for CIEDs exposed toirradiation of 2 Gy by 10 MV photons Multiple reports of errors due to 18 MV photon beamsand 1 Gy delivered at isocenter (regardless of proximityto CIED) Defibrillators are more sensitive to radiation damagethan pacemakers: in one report, every single ICD exposedto direct irradiation malfunctioned in some way16
CIED issues in EBRT “ there does not appear to be any consistent wayto to predict how a device will fail or at what dosefailure will occur.”1– Current literature – such as the 2012 comprehensivereport of the Dutch Society of Radiotherapy – separatesCIED patients into risk categories2– Upcoming TG-203 from the AAPM will supersede theoutdated TG-34 report, and from previews given atmultiple AAPM meetings it appears that this document willtake a similar approach to the study from The Netherlands17
Risk categories and recommendations
Definition and quantification of “risks” Virtually impossible to quantitatively approximatethe risk of radiation-induced CIED malfunction– Though generally proportional to accumulated dose, thereis no clear linear relationship to radiation dose– Similar devices (in fact, exact same models) may behavecompletely differently, suggesting overall stochastic effects– Proximity to the treatment fields is irrelevant in thepresence of neutron dose– Level of device-dependence (also difficult to quantify) is aprimary concerning when assessing relative risk19
Types of malfunctions reported in the contextof radiotherapy Transient fluttering effectsReset to factory programmingDecrease in battery life or total loss of electric functionDecrease in pacing amplitudeDecrease in shock energy (ICD)Erroneous ventricular fibrillation or ventriculartachycardia detection Runaway pacemaker or defibrillator Shock coil failure (ICD) Total , catastrophic defect20
“Risk” for CIED-dependent patients PalpitationsShortness of breathVertigoSyncope (pass out due to loss in blood pressure)Even in the transient malfunction setting, the patient’scondition can deteriorate to life-threatening cardiac eventCatastrophic decrease in heart rate and blood pressureVentricular tachycardiaVentricular fibrillationCardiopulmonary resuscitation may be required, followedby temporary external pacingProhibition of life-saving intervention from ICD21
Risk of serious complications in context ofCIED malfunction Majority of CIED malfunctions are transient,requiring at most reprogramming FDA reports risk of CIED malfunction as 1 in 75,000for pacemakers and 1 in 13,500 for defibrillators1– Risk of mortality due to CIED malfunction within thesame population was 1 in 300 for ICP and 1 in 275 for ICD1 0.7% risk of preventing a life-saving shock by deactivatingan ICD for a 6-week course of radiotherapy2 0.5%-6% risk of serious surgical complications (e.g.pneumothorax, infection) if CIED must be replaced222
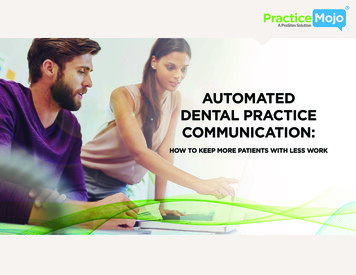
Risk Categories Low Risk– Pacing-independent AND 10 MV photons AND CIEDreceives 2 Gy (and 1 Gy for ICD) Medium Risk– Pacing-independent AND 10 MV photons AND CIEDreceives 2-5 Gy– Pacing-dependent AND 10 MV photons AND CIEDreceives 5 Gy High Risk– 10 MV photons AND CIED receives less 5 Gy– 10 MV photon in any scenario23
This chart4 willbe adopted byTG-203 but isONLY VALID fortreatmentswith 10 MVphotons ( 60%of EBRTpatients)24
Risk Categories Notes concerning physical (i.e., hard) wedges:– Scatter from a physical wedge significantly increases doseoutside the treatment field6-9– Treatment planning systems do not estimate dose outsidethe field well, and especially not in the presence of aphysical beam modifier1-10– For an 18 MV beam, neutron dose is 6.5 times higher (onaverage) for a hard-wedged beam compared to an openbeam10 For EBRT plans in which physical wedges cannot beavoided, RISK LEVEL must be individually assesed25
Current CIED-management process atNHCI (Atlanta GA)
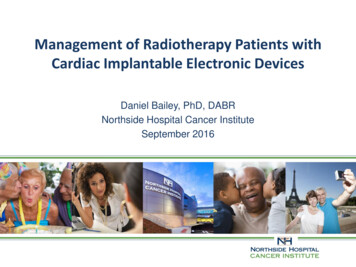
Current CIED-management process1. Nursing evaluation and notification of department2. CT simulation includes pacemaker if within 20 cm of treatmentfields3. Physician and dosimetrist plan and approximate CIED dose4. Physician and physicist come up with preliminary managementplan based upon risk level5. Physician or physicist contact patient’s cardiologist and/orelectrophysiologist6. Pacemaker interrogation services (internal or vendor-provided) isarranged7. Nursing cardiac monitoring and AED availability arranged ifnecessary8. Discharge instructions include a follow-up with cardiologist orelectrophysicologist within 1 month (typically two weeks)27
Current CIED-management issues1. Is the patient CIED-dependent?– This information is ideally determined at the first consult– Often, the patient’s knowledge is not dependable– Often, the cardiologist listed on the patient’s ID card iseither unreachable or no longer managing the patient– If not certain, patient must have an initial EP evaluationto verify device dependence2. What is the planned dose to the CIED?– Within the approximations of the TPS, but so is all currentliterature– Physician/dosimetrist/physicist select risk category28
Current CIED-management issues3. Contact patient’s cardiologist or electrophysiologist todiscuss management plan– Typically do not wish to complete or sign any paperwork,but it is always offered as a courtesy4. Contact either hospital pacemaker services ormanufacturer support if at a remote location– Pacemaker services requires a physician’s order, but notnecessarily a cardiologist– While vendor support is usual easy to secure, dailymonitoring is not supported by any vendor29
Current CIED-management issuesWe are making great effort to assimilate currentnational and international guidelines into ourroutine management of CIED patients but this isan ongoing and laborious process.This process requires a multi-disciplinary team ofprofessionals and continual re-evaluation of themanagement plan, basically for every individualpatient.30
Selected works cited1.2.3.4.5.Marbach, J. R., et al. "Management of radiation oncology patients withimplanted cardiac pacemakers: Report of AAPM Task Group No. 34." Medicalphysics 21.1 (1994): 85-90.Prisciandaro, J. “An Institutional Experience Managing the Care of Patients withCIEDs.” AAPM 2014. http://www.aapm.org/education/VL/vl.asp?id 3224. Lastaccessed 24 July 2015.Makkar, Akash, et al. "Effect of radiation therapy on permanent pacemaker andimplantable cardioverter-defibrillator function." Heart Rhythm 9.12 (2012):1964-1968.Hurkmans, Coen W., et al. "Management of radiation oncology patients with apacemaker or ICD: a new comprehensive practical guideline in TheNetherlands." Radiat Oncol 7.1 (2012): 198-198.Mihailidis, D. “New Comprehensive and Practical Guidelines for ManagingRadiotherapy Patients with Cardiac Devices: TG-203.” AAPM 2014.http://www.aapm.org/education/VL/vl.asp?id 3225. Last accessed 24 July2015.31
Selected works cited6.7.8.9.10.Li, Zuofeng, and Eric E. Klein. "Surface and peripheral doses of dynamic andphysical wedges." International Journal of Radiation Oncology* Biology* Physics37.4 (1997): 921-925.Stovall, Marilyn, et al. "Fetal dose from radiotherapy with photon beams:report of AAPM Radiation Therapy Committee Task Group No. 36." Medicalphysics 22.1 (1995): 63-82.Varatharaj, C., et al. "Variation of beam characteristics between three differentwedges from a dual-energy accelerator." Journal of medical physics/Associationof Medical Physicists of India 36.3 (2011): 133.Kim, Yeon Sil, et al. "Comparison of Virtual Wedge versus Physical WedgeAffecting on Dose Distribution of Treated Breast and Adjacent Normal Tissue forTangential Breast Irradiation." The Journal of the Korean Society for TherapeuticRadiology and Oncology 22.3 (2004): 225-233.Mesbahi, Asghar, et al. "Effect of wedge filter and field size on photoneutrondose equivalent for an 18MV photon beam of a medical linear accelerator."Applied Radiation and Isotopes 68.1 (2010): 84-89.32
1. Nursing evaluation and notification of department 2. CT simulation includes pacemaker if within 20 cm of treatment fields 3. Physician and dosimetrist plan and approximate CIED dose 4. Physician and physicist come up with preliminary management plan based upon risk level 5. Physician or physicist contact patient's cardiologist and/or