Transcription
A Comparison of RN-to-BSN CompletionGraduates to Generic BSN Graduates: IsThere a Difference?Nancy L. Chornick, PhD, RNABSTRACTThis study compares RN-to-BSN completion graduatesand generic BSN graduates in frequency of critical nursingactivities performed when caring for patients and indegree of commitment to the profession. Results indicatethat RN-to-BSN completion . graduates perform in amanner similar to generic BSN graduates; however,RN-to-BSN graduates more frequently demonstrated professional commitment such as attending continuing education programs, and furthering their education. Thesefindings support not only the current RN-to-BSN completion education program's but also the value of this .c ohort tothe nursing profession.IntroductionAlthough the largest portion of practicing nurses in theUnited States do not have a baccalaureate degree, many ofthese nurses are returning to school to continue theireducation. In order to accommodate those nurses interested in completing a baccalaureate degree, many schoolshave developed modified RN-to-BSN completion programs(Creasia, 1989; Green, 1987; Roudonis, 1987). In mostinstances, RN-to-BSN completion programs are designedto take advantage of past learning experiences. Placementis determined through testing, with nurses often beingDr. Chornick is Assistant Professor, Department of AdministrativeStudies in Nursing, College of Nursing, University of Illinois atChicago.Address reprint requests to Nancy Chornick, PhD, RN, Department of Administrative Studies in Nursing (M/C 802), College ofNursing, University of Illinois at Chicago, 845 S. Damen Ave.,Chicago, IL 60612.May 1992, Vol. 31, No.5required to take only those courses with content whichthey have not had.Although the need to provide a way for nurses toadvance' educationally has been recognized, concernsabout the quality ofRN-to-BSN completion graduates hasbeen a long-standing issue (Boyar, Senturia, & Palisin,1989; Lynn, McCain, & Boss, 1989). Are nurses whocomplete these programs adequately socialized to theprofession? Do they function in a similar manner as RNswhose basic nursing edu.c ation is a baccalaureate degree?A basic underlying assumption of this s.tudy is thatdifferences do exist between baccalaureate-prepared nurses(BSN) and nurses without a baccalaureate degree. A reviewofthe literature indicates that, depending on which variableis being meaSUred, differences mayor may not be evident.For instance, in three studies looking at professionalism,two found BSN students more professional than associatedegree in nursing (ADN) students (Jones & Jones, 1977;Murray & Morris, 1982; Richards, 1972). In three studies ondecision-making, only partial support existed for the premise that the decision-making of BSN nurses is moreprofessional (Gray, Murray, Roy, & Sawyer, 1977; Jacobs,1980; Johnston, 1982). Before performing the analysis forthe current study, data were analyzed to determine ifdifferences did exist in the baccalaureate-prepared nurse inthe variables to be considered.An analysis of the Illinois Department of ProfessionalRegulation's 1990 Biennial Survey of Registered Nursesdata set, comparing ADN nurses and diploma nurses withBSN nurses, demonstrated significant differences with theBSN nurse more frequently performing critical nursingactivities such as completing psychosocial exams, usingnursing diagnosis, etc. The BSN nurse also reportedsignificantly more professional commitment behaviorssuch as increased incidence of participation in continuingeducation, enrollment in academic programs, and certification in a specialty area (Chornick, 1990).203
LzaqRN-TO-BSN VS. GENERIC BSN GRADUATESFew studies have compared those nurses who enterednursing with a BSN to those nurses with less educationwho subsequently completed a BSN. Several studies havereported differences between RN-to-BSN completion student nurses and their generic BSN counterparts. Forinstance, Thomas (1979) found that RN-to-BSN completion students were less oriented toward traditional viewsof nursing than other students. Lynn et a1. (1989) reporteda lack of overall change in the measurement of professional development in RN-to-BSN completion students.King (1986) determined that significant differences existed between RN-to-BSN completion and generic BSNstudents on the variables of ego development and lifestages.Only two studies differentiated between the two types ofbaccalaureate-prepared nurse. McCloskey (1983) reportedthat ADN nurses who completed a BSN were more highlyrated in nursing practice than generic BSN nurses or ADNnurses. In the second study, ADN nurses who hadcompleted a BSN were compared with generic BSN andADN nurses in terms of professionalism. Results indicatedthat the ADN nurse13 who completed a BSN were moreprofessional than either the ADN or generic BSN nurses(Lawler & Rose, 1987).Purpose of the StudyThis study compared the behaviors of RN-to-BSNcompletion graduates with generic BSN graduates todetermine if differences existed between the groups'behaviors performed when caring for patients and in theirdegree of corhmitment to the profession. Specific questionsthat this study attempted to answer were:1. Do RN-to-BSN completion graduates perform criticalnursing activities as frequently as generic BSN graduateswhen caring for patients?2. Do RN-to-BSN completion graduates demonstrate acomparable degree of commitment to the nursing profession as generic BSN graduates?DefinitionsThe following definitions were used: The basic level ofnursing education was that level which initially preparedone to be a nurse, e.g., licensed practical nursing (LPN),diploma, ADN, and BSN. An RN-to-BSN completiongraduate is a nurse whose basic level of nursing educationwas something less than a BSN, i.e., LPN, ADN, ordiploma, who had returned to school for a BSN. A genericBSN graduate is a nurse whose basic level of nursingeducation was a BSN. Critical nursing activities are thoseessential activities performed by a professional nursewhen caring for patients. They are measured by thefrequency of obtaining health histories, performing physical examinations, performing psychosocial examinations,developing nursing diagnoses and therapeutic plans,instructing patients in prevention or management ofillness and health maintenance, and evaluating patientoutcomes.204MethodsData were obtained from the 1990 Illinois Nurses Survey.The state of Illinois was selected because the population isrepresentative of the nation in terms of urban/ruraldistribution and income. In addition, Illinois reports nursingdemographics similar to national surveys, such as educational distribution and minority representation. The 1990Illinois Nurses Survey was mailed along with registrationmaterials to all persons who are licensed as RNs in the stateof Illinois. Information was collected on 66,005 nurses froma sample of 117,796 nurses who applied for licensure (56%response rate) and consisted of employment, work functions,and continuing educational activities. To assure anonymity,renewal materials were separa ted at the state regulatoryagency before being forwarded to the investigators. Surveyswere electronically scanned and uploaded to an IBMmainframe computer. Data analysis was performed usingthe SPSS-X Statistical Package to obtain frequ.encies andcross-tabulations. The acceptable level of significance wasset at .05.SampleThe sample consisted of those nurses who had obtaineda BSN degree and was divided into four groups. Threegroups consisted of individuals who had entered nursingat one of the various levels-LPN, ADN, or diploma-andhad subsequently returned to school to complete a baccalaureate degree. The fourth group consisted of those whohad entered nursing with a BSN degree. A preliminarydata analysis indicated that there was an uneven distribution of types of positions held by the four groups.Therefore, in order to compare the four groups moreclosely, only those nurses who reported spending at least50% of their usual work eek in direct patient care wereincluded in the sample.InstrumentThe 1990 Illinois Nurses Survey is a four-page , 55-itemscannable survey. Included are questions on years andtype of employment, work setting, position, functions 'performed at work, and educational activities, along withdemographic information.Questions pertaining to this study asked how frequentlyrespondents performed critical nursing activities whengiving patient care. Critical nursing activities weremeasured by frequency with responses categorized as: (1)neuer, (2) for less than 10 of my patients, (3) for 10 to 50 ofmy patients, and (4) for ouer 50 of my patients. Othercomparisons determined degree of commitment to nursingand were measured by enrollment in a formal educationalprogram, certification in a specialty area, and number ofcontinuing education hours earned in the past year.Continuing education hours were determined by fourcategories ranging from none to more than 40 hours.Data analysisThe sample (n 11,884) consisted of four groups of BSNnurses with either an LPN (n 471), ADN (n 1,019),Journal of Nursing Education
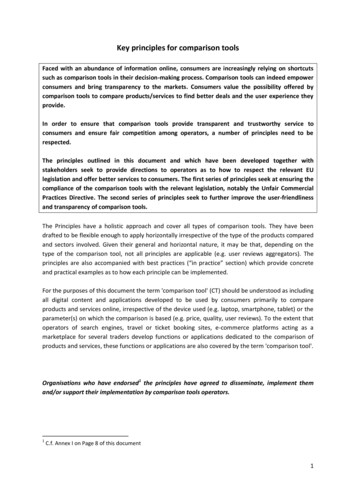
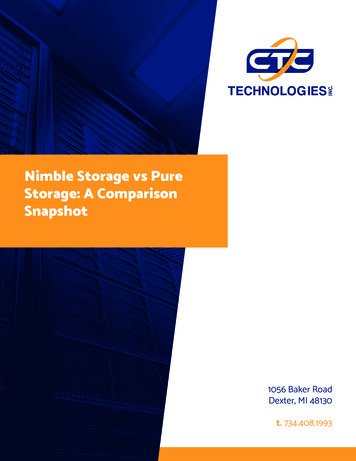
CHORNICKTABLE 1Demographic VariablesLPN (N 491)Diploma (N 2,716)ADN (N 1,037)Generic BSN (N 8,588)Gender (%)*MaleFemale5.189.43.091.66.688.22.991.9Mean age (SO)38.30 (8.37)44.50 (10.19)38.82 (8.38)34.64 (9.14)Race (%)HispanicsBlacksAsianWhiteAmerican .31.23.211 .284.30.164.91.611.62.019.368.63.011 .10.716.669.71.98.92.117.569.40.84.30.824.7Marital Status (%)MarriedWidowedDivorcedSeparatedNever MarriedMean number of children (50)Gross household income (%) 21,000 21,000- 29,999 30,000- 39 ,999 40,000- 49,999 50,000- 59,999 60,000 Mean years worked as RN (50)Principal position (%)Staff nurseNurse clinicianNurse practitionerClinical nurse .specialistCertified nurse anesthetistCertified nurse midwifeCharge nurseHead/assistant head nurseInservice educational instructorAdministrative nursing serviceHome careConsultantPrivate nurseOffice nurseSchool nurseOther1.15 (1.31)4.717.423.915.112.725.29.06 .71.15 (1.25)1.15 .618.72 (9.43)11.24 71.16 (1 .27)4.217.420.515.115.627.29.64 (6.82)73.42.12.21.51.00.64.52.40.22.94.21.82.6'% 100 due to missing data.diploma (n 2,676 ) or BSN (n 7,718 ) as a basic level ofpreparation. Many of the descriptive data were similar forall four groups (Table 1). The majority of respondents ineach group consisted of married white females with one ortwo children. More than 50% of each group reported a meangross household income between 30,000 and 60,000.Differences did exist between the groups in terms of age,May 1992, Vol. 31, No.5years worked as an RN, and types of positions held, with themajor differences existing between generic BSNs andremaining groups. The generic BSN tended to be younger(mean age of 34 years), and most frequently reported beinga staff nurse (76.8%). The other three groups of nursesreported a wider range of positions, including home care,private duty, and office nursing despite the inclusion criteria205
2QRN-TO-BSN VS GENERIC BSN GRADUATE TABLE 2Significant Comparisons of Frequency of Performance of Critical Nursing ActivitiesFrequency of Performance (% of time)Critical Nursing ActivityPerformance of physical examination1 to 5 yearsBSNDiplomaADNLPN6 to 10 years11 to 15 years16 to 20 yearsNever N (%) 10% N(%)419 (1 7.0)44 (28.8)21 (17.2)20 (18.7)NSNSNS253 (10.3)18 (11.8)10 (8.2)9 (8.4)Performance of psychosocial examination1 to 5 yearsBSN472 (19.2)Diploma48 (31.0)ADN25 (20.3)LPN19 (17.1)6 to 10 yearsNS11 to 15 yearsNS16 to 20 yearsBSN211 (30.5)Diploma191 (42. 1)ADN43 (30.9)LPN20 (45.5)10%t050% N(%)357202122(14.5)(13.1)(17.2)(20.6)1429 (58.1)71 (46.4)70 (57.4)56 )(22.8)(27.0)932523941158 (22.8)74 (16.3)24 (17.3)2 (4.5)12177287(17.5)(17.0)(20.1)(15.9)202 (29.2)112 (24.7)44 (31.7)15 (34.1)1890 (75.5)97 (63.0)92 (73.0)79 (68.7)483273121Performance of nursing diagnoses1 to 5 yearsBSNDiplomaADNLPN6 to 10 years11 to 15 yearsBSNDiplomaADNLPN16 to 20 years153 (6.1)13 (8.4)11 (8.7)5 (4.3)NS154 (6.2)13 (8.4)9 (7.1)11 (9.6)307 (12.3)31 (20.1)14 (11.1)20 (17.4)100 (7.1)59 (12.3)30 (10.2)12 (16.0)NS1014125722861436Develop therapeutic plans1 to 5 years11 to 15 yearsBSNDiplomaADNLPN16 to 20 yearsNSNS212 (8.0)56 (11 .8)41 (13.8)5 (6.5)NSInstruct patient In prevention of Illness1 to 5 years6 to 10 years11 to 15 years16 to 20 yearsBSNDiplomaADNLPN 50% N (%)(7.2)(8.6)(8.5)(9.3)140 (10.1)53 (11 .2)26 (8.8)12 (15.6)(16.3)(12.8)(14.6)(8.0)246 (17.7)71 (15.0)44 (14.8)13 (16.9)(37.9)(33.5)(31 .7)(36.9)972 (69.4)317 (66.3)196 (66.7)50 (66.7)894 (64.2)294 (62.P)186 (62.6)47 (61 .0)NSNSNS41 (5.4)29 (6.1)16 (11.0)7 (15.6)Instruct patient in management of Illness1 to 5 yearsNS6 to 10 yearsNS11 to 15 yearsBSN82 (5.7)Diploma28 (5.8)ADN20 (6.6)LPN3 (4.1)16 to 20 918.0810.619"99996.2212.253.78120 (15.7)102 (21.5)19 (13.0)3 (6.7)130 (9.1)48 (10.0)28 (9.2)11 (14.9)164 (24 .1)113 (23.8)30 (20.5)8 (17.8)32475668(22.6)(15.6)(21 .7)(10.8)4172318127(54.7)(48.6)(55.5)(60.0)896 (62.6)329 (68.5)190 (62.5)52 (70.3)26.189t9.3610.079918.1612.589t9Evaluate patient outcome1 to 5 years6 to 10 years11 to 15 years16 to 20 yearsNSNSNSNS14.296.225.2215.539999Instruct patients In health maintenance1 to 5 years6 to 10 years11 to 15 years16 to 20 yearsNSNSNSNS13.617.275.949.329999"P . 01tp .Ol:j:p .OOl206Journal of Nursing Education
,CHORNICKTABLE 3Significant Comparison of CommitmentProfessional VariablesCertified in a specialty area1 to 5 yearsBSNDiplomaADNLPN6to10yearsBSNDiplomaADNLPN11 to 15 yearsBSNDiplomaADNLPN16 to 20 yearsBSNDiplomaADNLPNEnrolled in a formal education program1 to 5 yearsBSNDiplomaADNLPN6 to 10 yearsBSNDiplomaADNLPN11 to 15 yearsBSNDiplomaADNLPNYes N (%)No N (%)294362018(11 1)(85.5)(85 .7)14.283'117935822159(78.9)(71 .9)(69.5)(72 .0)19.683'(21 .1)(28.1)(30.5)(28.0)117935822159(78.9)(71 .9)(69.5)(72 .0)19.673'177 (22.5)151 (29.6)49 (31 .6)17(31 .5)61135910637(77.5)(70.4)(68.4)(68.5)11.90 -3'FUll-timePart-time64 (2.4)9 (5.0)9 (6.5)3 (2.4)239 (8.9).31 (17.1)28 (20.1)15(11 9208183555719(7.3)(13.4)(15.6)(10.0)2292 (91.0)326 (79.5)288 (78.9)163 (85.8)89.136'84 (5.5)60(11 .8)50 (15.8)17(21.3)1409 (92.8)436 (85.8)256 (80.8)63 (78.8)68.116'29.676'Chi-square10.18df9(1 .8)(7.1)(5.5)(4.2)26 (1 .7)12 (2.4)11 (3.5)16 to 20 yearsBSNDiplomaADNLPN51332(.6)(2.5)(1 .9)(3.7)Not enrolled43 (5.3)60 (11 .7)16(10.3)6 (11 n in continuing education1 to 5 years6to10yearsBSNDiplomaADNLPNNoneNS 20 hrs20-40 hrs 40 hrs397 (16.0)61 (15.2)44 (12.1)22(11.6)1257 (50.5)173 (43.0)159 (43.6)l'l9 (46.8)653 (26.3)114 (28.4)113 (31.0)51 (26.8)180 (7.2)54 (13.4)49 (13.4)2804.7)46.499'11 to 15 yearsBSNDiplomaADNLPN1915735516 to 20 yearsBSNDiplomaADNLPN(12.8)(11 .4)(11 1936(29.2)(25.9)(37.5)(43.9)130 (8.7)56 (11 .2)37 (11 .7)8 (9.8)29.099'87 (10.8)40 (7.8)17 (10.9)5 31 .2)(33.2)(42.9)(27.8)77 (9.6)61 (11 .9)17 (10.9)5 (9.3)19.399t' p .OO1.tp .01May 1992, Vol. 31, No.5207
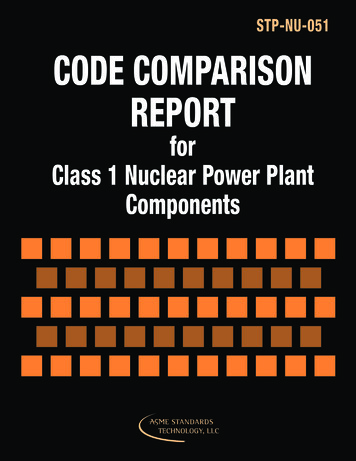
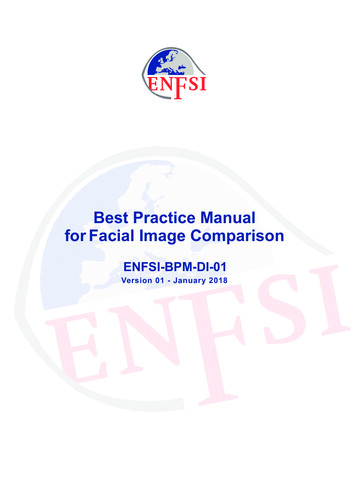
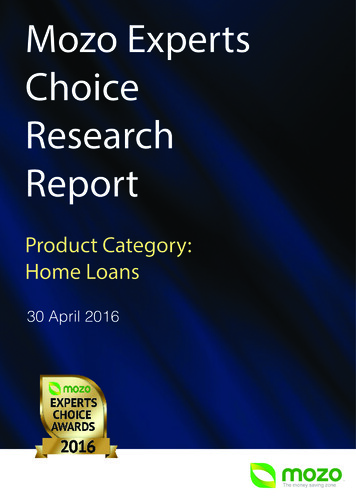
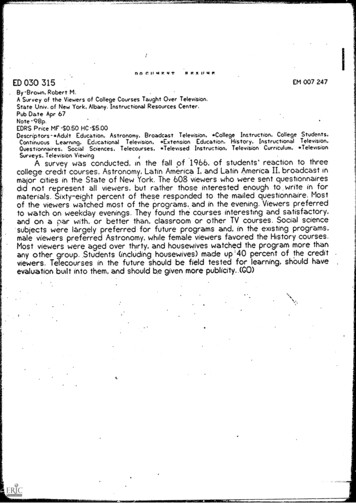
.ZSQRN-TO-BSN VS. GENERIC BSN GRADUATESof reporting at least 50% of time in direct patient contact.Diploma nurses reported the highest mean total number ofyears worked as an RN (9.92 years). This result is notunexpected because the declining number of diplomaschools decreases the possibility of recent graduation from .this type of program. Licensed practical nurses reported amean of 2.36 years worked as an RN. Due to the wording ofthe question, the number of years that the LPN workedbefore becoming a RN was not taken into account.Table 2 shows the significant results of the question thatasks nurses to indicate how frequently they performedcritical nursing activities when caring for their patients.Because total years in nursing was a variable determined toaffect nurses' behaviors, it was controlled by analyzing thedata using five-year cohorts. When years in nursing andtime spent in direct patient contact were controlled, fewsignificant differences existed among all groups whenviewing critical nursing activities. Frequency of criticalnursing activities that were not significant among any of thefive-year cohorts were: obtaining a health history, instructing patients in health maintenance, assisting patients inplanning health care, ' instructing patients in prevention ofillness, and evaluating patient outcomes.Significant differences existed in the one- to five-yearcohort for performing physical examinations, performanceof psychosocial examinations, and developing nursingdiagnoses with generic BSN nurses tending to report thesebehaviors more frequently. No significant differencesexisted in the 6- to 10-year cohort. In the 11- to l5-yearcohort, differences were noted in performing nursingdiagnoses, developing therapeutic plans, and instructingpatients in management of illness, with generic BSNsmore frequently reporting these activities.Generic BSNs also reported performing more psychosocial examinations and instructing patients in prevention ofillness in the 16- to 20-year cohort. The four differencesnoted in performance of critical nursing activities betweenthe generic BSN group and remaining groups may be due, inpart, to the multiple positions held by the RN-to-BSNcompletion graduates. Several of these critical nursingactivities, such as developing nursing diagnoses, couldpossibly occur more frequently when .working in a staffnurse position than in other positions such as office nurse orschool nurse.Areas pertaining to commitment that were consideredfor this study included certification, continuing education,and additional formal education. Table 3 indicates thatgeneric BSNs reported significantly fewer continuingeducation hours, were not certified in specialty aJ:eas asfrequently, and were less inclined to continue with theirformal education than those nurses who had less thanBSN. Only in the one- to five-year cohort for participationin continuing education did no differences exist.ConclusionThe results of this study suggest that RN-to-BSNcompletion graduates not only perform critical nursing208activities as frequently as generic BSN nurses, butdemonstrate significantly more behaviors indicating commitment. The fact that RN-to-BSN completion graduatesperform critical nursing activities as frequently as genericBSN graduaLes suggesLs LhaL Lhe wrrenL educationalprograms offered for these students are adequate. Concerns so frequently expressed regarding the quality of theRN-to-BSN completion graduate appear to be unfounded.Considering the large number of nurses without a BSNand the comparable product produced, increased efforts byeducators to recruit this pool of nurses seem worthwhile.RN-to-BSN completion graduates are more likely thangeneric BSN graduates to continue with their education,to be certified in a specialty area, and to attend continuingeducation programs, i.e., behaviors often attributed toprofessional commitment. Possibly the nurse returning fora BSN differs from the generic BSN nurse in terms ofambition and self-direction. They have chosen to continueto improve their position through education. Also, RN-toBSN completion graduates are individuals who haveworked in the profession and have decided to make anadditional investment in their chosen field. A selectionprocess appears to be in progress. By virtue of continuingtheir education to achieve a BSN, these nurses havealready demonstrated a commitment to their professioncompared to RNs whose first contact with nursing placesthem in the role of the BSN nurse. In addition, thiscommitment appears to continue for the RN-to-BSNcompletion graduate after the BSN is achieved. TheRN-to-BSN graduate appears to be a highly motivatedindividual and a valuable part of the nursing profession.ReferencesBoyar, D., Senturia, B., & Palisin, H . (1989). Accelerated LPN-RNnursing education: Is role socialization lost along the way?Journal of Nursing Education, 28, 361-365.Chornick, N . (1990). A comparison of graduates of BSN, associatedegree, and diploma nursing programs. Unpublished manu- .script.Creasia, J. (1989). Reducing the barriers to RN educationalmobility. Nurse Educator, 14(4),29-33.Gray, J., Murray, B., Roy, J., & Sawyer, J. (1977). Do graduates oftechnical and professional nursing programs differ in practice?Nursing Research, 26, 368-373 . .Green, C. (1987). Multiple role women: The real world of themature RN learning. Journal of Nursing Education, 26,266-27l.Jacobs, A. (1980). Clinical competencies of baccalaureate, AD anddiploma nurses-Are they different? Issues, 1, 1-3 . .Johnston, S. (1982 ). The use ofthe rines model in differentiatingprofessional and technical nursing practice. Nursing ' HealthCare, 2, 374-379.Jones, S., & Jones, P. (1977). Nursing student definitions of thereal nurse. Journal of Nursing Education, 16, 15-2l.King, J. (1986). A comparative study of adult developmentalpatterns of RN and generic students in a baccalaureatenursing program. Journal of Nursing Education, 25, 366-371.Lawler, T., & Rose, M. (1987). Professionalization: A comparisonamong generic baccalaureate ADN and RNIBSN nurses. NurseJournal of Nursing Education
,CHORNICKEducator, 12(3), 19-22.Lynn, M., McCain, N., & Boss, B. (1989). Socialization of RN toBSN. Image: The Journal ofNursing Scholarship, 24, 232-237.McCloskey, J. (1983). Nursing education and job effectiveness.Nursing Research, 32, 53-58.Murray, L., & Morris, D. (1982). Professional autonomy amongsenior nursing students in diploma, associate degree andbaccalaureate nursing programs. Nursing Research, 31, 311313.Richards, M. (1972). A study of differences in psychologicalcharacteristics of students graduating from three types ofbasis nursing progr s . Nursing Research, 21, 258-26l.Roudonis, B. (1987). Adult education: Its implications for baccalaureate nur.sing education. Journal ofNursing Education, 26,164-166.Thomas, J. (1979). Professional socialization of students in fourtypes of nursing education programs (Doctoral dissertation,University of Florida). Dissertation Abstracts International,39,5966A.Help as muchas you can. AmericanRed CrossTogether, we can change things.A Public ServIce 0 1Th is Newspaper & The Advtrtl'.nO Councl'May 1992, Vol. 31, No.5 209
Copyright of Journal of Nursing Education is the property of SLACK Incorporated and its contentmay not be copied or emailed to multiple sites or posted to a listserv without the copyrightholder's express written permission. However. users may print. download. or email articles forindividual use.
diploma, ADN, and BSN. An RN-to-BSN completion graduate is a nurse whose basic level of nursing education was something less than a BSN, i.e., LPN, ADN, or diploma, who had returned to school for a BSN. A generic BSN graduate is a nurse whose basic level of nursing education was a BSN. Critical nursing activities are those