Transcription
SEER Program Coding and Staging Manual 2007Coding GuidelinesBreastC500 -C509Primary SiteC500 Nipple (areolar)Paget disease without underlying tumorC501Central portion of breast (subareolar) area extending 1 cm around areolar complexRetroareolarInfraareolarNext to areola, NOSBehind, beneath, under, underneath, next to, above, cephalad to, or below nipplePaget disease with underlying tumorC502Upper inner quadrant (UIQ) of breastSuperior medialUpper medialSuperior innerC503Lower inner quadrant (LIQ) of breastInferior medialLower medialInferior innerC504Upper outer quadrant (UOQ) of breastSuperior lateralSuperior outerUpper lateralC505Lower outer quadrant (LOQ) of breastInferior lateralInferior outerLower lateralC506Axillary tail of breastTail of breast, NOSTail of SpenceC508Overlapping lesion of breastInferior breast, NOSInner breast, NOSLateral breast, NOSLower breast, NOSMedial breast, NOSMidline breast NOSOuter breast NOSSuperior breast, NOSUpper breast, NOS3:00, 6:00, 9:00, 12:00 o’clockAppendix CSite-Specific Coding ModulesC-605
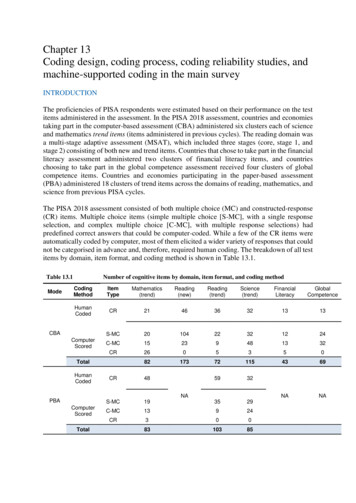
SEER Program Coding and Staging Manual 2007C509Breast, NOSEntire breastMultiple tumors in different subsites within breastInflammatory without palpable mass¾ or more of breast involved with tumorDiffuse (tumor size 998)Additional Subsite DescriptorsThe position of the tumor in the breast may be described as the positions on a clockO'Clock Positions and CodesQuadrants of 50.1465LIQC50.3RIGHT BREAST121C50.42938C50.21110UOQ3847LIQC50.365LEFT BREASTLOQC50.5Priority Order for Coding SubsitesUse the information from reports in the following priority order to code a subsite contains conflictinginformation:1.2.3.4.Pathology reportOperative reportPhysical examinationMammogram, ultrasoundIf the pathology proves invasive tumor in one subsite and insitu tumor in all other involved subsites, codeto the subsite involved with invasive tumorC-606Site-Specific Coding ModulesAppendix C
SEER Program Coding and Staging Manual 2007When to Use Subsites 8 and 91. Code the primary site to C508 when there is a single tumor that overlaps two or more subsites,and the subsite in which the tumor originated is unknown2. Code the primary site to C508 when there is a single tumor located at the 12, 3, 6, or 9 o’clockposition on the breast3. Code the primary site to C509 when there are multiple tumors (two or more) in at least twoquadrants of the breastGradeConvert BR Score/Grade to SEER CodeUse the table below to convert BR score, grade or terminology to SEER code.BRScores3-56, 78, 9---BR GradeLowIntermediateHigh---NuclearGrade1/3; 1/22/32/2; 3/34/4TerminologyHistologic GradeWell differentiatedModerately differentiatedPoorly differentiatedUndifferentiated/anaplasticI, I/III, 1/3II, II/III; 2/3III, III/III, 3/3IV, IV/IV, 4/4SEERCode1234Priority Rules for Grading Breast CancerCode the tumor grade using the following priority order:1.2.3.4.5.6.7.8.Bloom-Richardson (Nottingham) scores 3-9 converted to grade (see conversion table below)Bloom Richardson grade (low, intermediate, high)Nuclear grade onlyTerminologyDifferentiation (well differentiated, moderately differentiated, etc)Histologic gradeGrade i, grade ii, grade iii, grade ivBloom-Richardson (BR)BR may also be called: modified Bloom-Richardson, Scarff-Bloom-Richardson, SBR grading, BRgrading, Elston-Ellis modification of Bloom Richardson score, the Nottingham modification of BloomRichardson score, Nottingham-Tenovus, or Nottingham gradeBR may be expressed in scores (range 3-9)The score is based on three morphologic features of “invasive no-special-type” breast cancers (degree oftubule formation/histologic grade, mitotic activity, nuclear pleomorphism of tumor cells)Use the following table to convert the score into SEER codeBR may be expressed as a grade (low, intermediate, high)BR grade is derived from the BR scoreFor cases diagnosed 1996 and later, use the following table to convert the BR grade into SEER code(Note that the conversion of low, intermediate, and high is different from the conversion used for all othertumors).LateralityLaterality must be coded for all subsites.Appendix CSite-Specific Coding ModulesC-607
SEER Program Coding and Staging Manual 2007This page left blankC-608Site-Specific Coding ModulesAppendix C
Appendix CBreast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)Equivalent or Equal TermsSite-Specific Coding ModulesSynonyms for “in situ”Behavior code ninvasiveDefinitionsCarcinoma with osteoclast-like giant cells (8035): This is a specific type of duct carcinoma. The carcinomatous part of the lesion is mostcommonly an infiltrating duct carcinoma.Ductular carcinoma (8521): A malignancy that is infrequently found in the breast and may be found with greater frequency in other organs suchas pancreas or prostate. Code 8521 is seldom, if ever, applied to the breast. Although the ICD-O-3 suggests that 8521 is a site-associated code; theaddition of (C50. ) after this code may be misleading. The WHO Histological Classification of Tumours of the Breast does not list 8521, ductularcarcinoma.Duct carcinoma, NOS (8500): The largest group of breast cancers. Duct carcinoma, NOS is not a specific histologic type because it lacksspecific features that can be used to better classify the tumor. See Table 1 and Table 2 for intraductal and duct types.C-609Breast Terms and DefinitionsSEER Program Coding and Staging Manual 2007And, with (used in histology rules, i.e. duct and lobular is equivalent to duct with lobular)Duct, ductalMammary, breastMucinous, colloidNOS, NSTTumor, mass, lesion, neoplasm
Breast Terms and DefinitionsC-610Breast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)Inflammatory breast carcinoma (IBC): A breast cancer with a distinctive clinical presentation believed to be due to lymphatic obstruction froman underlying invasive adenocarcinoma. The vast majority of cases have a prominent dermal lymphatic infiltration by tumor. Dermal lymphaticinfiltration without the characteristic clinical picture is insufficient to qualify as inflammatory carcinoma.In Situ: A tumor that is confined to the duct system (ductular or lobular) and does not invade surrounding stroma.Site-Specific Coding ModulesInvasive: A tumor that penetrates beyond the ductal basement membrane into the adjacent stroma of the breast parenchyma.Lobular Carcinoma: Lobular carcinoma includes solid and alveolar patterns. About 5 to 10% of breast cancers are lobular. There is about a20% chance that the opposite breast will also be involved, and many of them arise multicentrically in the same breast.Paget Disease: Paget disease of the nipple is a condition where the epidermis of the nipple is infiltrated with neoplastic cells. ICD-O-3 classifiesall mammary Paget disease as a malignant process with a malignant behavior (/3). Under the matrix system, only if the Paget disease is explicitlyspecified as in situ or non-invasive by the pathologist, code the behavior in situ (/2).Phyllodes tumor (cystosarcoma phyllodes): A rare tumor with incidence ranging from 0.3% to 0.9% of all breast cancers. These tumors have anatural history and clinical behavior different from carcinoma of the breast. Criteria to classify benign, borderline and malignant cystosarcomaphyllodes utilize histologic parameters such as cellular atypia, mitotic activity and tumor margins. The reported incidence of malignantcystosarcoma phyllodes is approximately 25% of all phyllodes tumors.Pleomorphic carcinoma (8022): This is a specific duct carcinoma type; A rare variant of high grade ductal carcinoma, NOS.Sarcoma of breast: Primary sarcomas of the breast are rare accounting for less than 0.1% of all malignant tumors of the breast.Diagnoses may include fibrosarcoma, angiosarcoma, pleomorphic sarcoma, leiomyosarcoma, myxofibrosarcoma, hemangiopericytoma, and osteosarcoma (extra-osseous osteosarcoma of breast).Appendix CScirrhous Carcinoma: An adenocarcinoma with a firm-hard nodule associated with a dense connective tissue in the stroma.Scirrhous carcinoma is descriptive term, not a specific type of ductal carcinoma.SEER Program Coding and Staging Manual 2007Intracystic carcinoma/Intracystic papillary carcinoma: Variant of intraductal carcinoma used to describe encysted forms of papillarycarcinoma. Code intracystic carcinoma as in situ /2 unless the histology is described as invasive intracystic carcinoma.
Appendix CBreast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)Table 1 – Intraductal(8500/2) and Specific Intraductal CarcinomasNote: These are the most common specific intraductal carcinomas. This is not intended to be a complete list of all possible intraductal types. If a histologyappears only on table 1, it does not mean that it is impossible for that histology to occur with a malignant behavior (/3).Column 1:CodeCribriformSolidApocrineIntraductal, NOSComedoPapillaryIntracystic carcinomaMicropapillary/ClingingTable 2 – Duct (8500/3) and Specific Duct CarcinomasNote: These are the most common specific duct carcinomas. This is not intended to be a complete list of all possible duct types. If a histology appears only ontable 2, it does not mean that it is impossible for that histology to occur with an in situ behavior (/2).Column 1: Column 2:CodeType8022803585008501850285038508Pleomorphic carcinomaCarcinoma with osteoclast-like giant cellsDuct, NOSComedocarcinomaSecretory carcinoma of breastIntraductal papillary adenocarcinoma with invasionCystic hypersecretory carcinomaC-611Breast Terms and DefinitionsSEER Program Coding and Staging Manual 2007Site-Specific Coding Modules82018230840185008501850385048507Column 2:Type
Breast Terms and DefinitionsC-612Breast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)Table 3 – Combination Codes for Breast CancersUse this two-page table with rules H5, H6, H7, H8, H16, H17, H18, H19, H24, H25, H26 and H28 to select combination histologycodes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the case using the ICD-O-3histology code in column 4. Use the combination codes listed in this table only when the histologies in the tumor match the histologieslisted below.Column 2:Combined with HistologyOther than ductal and lobularColumn 3:Combination TermAdenocarcinoma with mixed subtypes*Column 4:Code8255/3*Lobular carcinoma in situ8522/2Infiltrating duct andIntraductal and two or more of thehistologies in Column 2 ORtwo or more of the histologies inColumn 2Infiltrating lobular llaryClingingTubularApocrineMucinousSecretory carcinomaIntraductal papillary adenocarcinoma withinvasionIntracystic carcinoma, NOSMedullaryIntraductal carcinoma and lobular carcinoma insituInfiltrating duct and lobular carcinomaIntraductal mixed with other types of carcinomaInfiltrating duct mixed with other types ofcarcinoma8523/3Infiltrating duct and one or moreof the histologies in Column 2Appendix CTable 3 continues on the next page8522/38523/2SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesColumn 1:Required HistologyAny combination excludinglobular and duct histologies fromTables 1 and 2Intraductal carcinoma and
Appendix CBreast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)Column 1:Required HistologyTable 3 continuedInfiltrating lobular carcinoma andPaget disease and*Rarely used for breast cancerC-613Breast Terms and DefinitionsColumn 3:Combination TermColumn 4:CodeTubularApocrineMucinousSecretory carcinomaIntraductal papillary adenocarcinoma withinvasionIntracystic carcinoma, NOSMedullaryPaget disease (NOS and invasive)Infiltrating duct carcinoma (includes anyspecific duct type listed in Table 2Intraductal carcinoma (includes any specificintraductal type in Table 1)Infiltrating lobular mixed with other types ofcarcinomaNote: Invasive carcinomas only. Do not use thiscode for in situ8524/3Paget disease and infiltrating duct carcinoma8541/3Paget disease and intraductal carcinoma8543/3SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesPaget disease andColumn 2:Combined with Histology
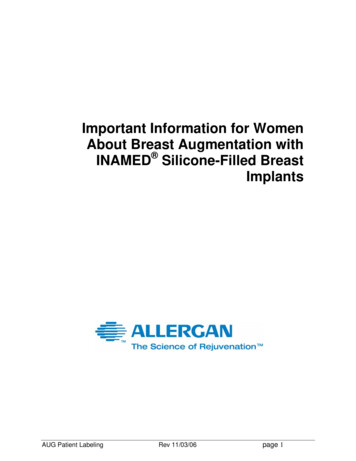
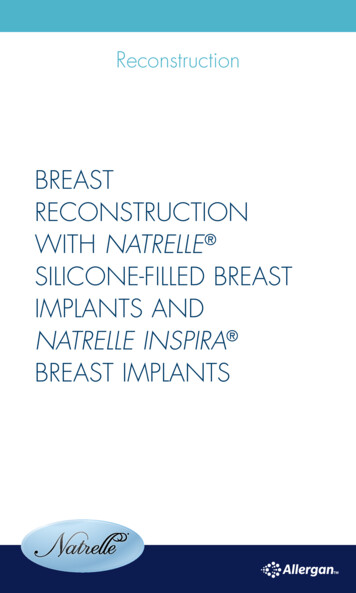
Breast Terms and DefinitionsC-614Breast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesAppendix CNetter illustration used with permission of Elsevier Inc. All rights reserved
Appendix CBreast Equivalent Terms, Definitions, Tables and IllustrationsC500-C509(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesNetter illustration used with permission of Elsevier Inc. All rights reservedC-615Breast Terms and Definitions
Breast Terms and DefinitionsC-616This page left blankSEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesAppendix C
Appendix CBreast Multiple Primary Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)questionDecisionNoteFlow Direction* Prepare one abstract. Use the histology coding rules to assign the appropriate histology code.** Prepare two or more abstracts. Use the histology coding rules to assign the appropriate histology code to each case abstracted.UNKNOWN IF SINGLE ORMULTIPLE TUMORSSite-Specific Coding ModulesIs it impossible to determine ifthere is a single tumor or multipletumors?NOTESTumor(s) not described as a metastasis.YESNOSINGLEPrimary*Use this rule only after all information sourceshave been exhausted.End of instructionsfor Unknown if Singleor Multiple TumorsGo to Single Tumoror Multiple TumorsSINGLE TUMORDECISIONNOTES1. Tumor not described as metastasis.2. Includes combinations of in situ and invasiveM2Is there inflammatory carcinomain one or both breasts?YESSINGLEPrimary*NOM3Is there a single tumor?NOC-617Go to MultipleTumors.Breast MPYESThe tumor may overlap onto or extend intoadjacent/contiguous site or subsite.End of instructionsfor Single Tumor.SEER Program Coding and Staging Manual 2007M1DECISION
Breast MPC-618Breast Multiple Primary Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)questionDecisionNoteFlow Direction* Prepare one abstract. Use the histology coding rules to assign the appropriate histology code.** Prepare two or more abstracts. Use the histology coding rules to assign the appropriate histology code to each case abstracted.MULTIPLE TUMORSDECISION1. Tumors not described as metastasis.2. Includes combinations of in situ and invasive.Multiple tumors may be a singleprimary or multiple primaries.YESSEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesM4Are there tumors in sites with ICD-O-3topography codes that are differentat the second (Cxxx) and/or thirdcharacter (Cxxx)?NOTESMULTIPLEPrimaries**NOM5Are there tumors diagnosed morethan five (5) years apart?YESMULTIPLEPrimaries**NOM6Is there inflammatorycarcinoma in one or both breasts?YESSINGLEPrimary*NOM7Is there a tumor(s) in each breast?Appendix CNONextPageYESMULTIPLEPrimaries**Lobular carcinoma in both breasts ("mirrorimage") is a multiple primary.
Appendix CBreast Multiple Primary Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)questionDecisionNoteFlow Direction* Prepare one abstract. Use the histology coding rules to assign the appropriate histology code.** Prepare two or more abstracts. Use the histology coding rules to assign the appropriate histology code to each case abstracted.DECISIONMULTIPLE TUMORS, continuedNOTES1. Includes combinations of in situ and invasive.2. Tumors are not described as a metastasis.Site-Specific Coding ModulesIs there an invasive tumor followingan in situ tumor more than 60 days afterdiagnosis?YESMULTIPLEPrimaries**2. Abstract as multiple primaries even if themedical record/physician states it is recurrenceor progression of disease.NOM9Are the tumors intraductal or ductand Paget Disease?YESNOM10Are the tumors lobular (8520) andintraductal or duct?YESNOM11Are there multiple intraductal and/orduct carcinomas?NOC-619NextPageBreast MPYESSINGLEPrimary*Use Table 1 and Table 2 to identify intraductal andduct carcinomasSEER Program Coding and Staging Manual 2007M81. The purpose of this rule is to ensure that thecase is counted as an incident (invasive) casewhen incidence data are analyzed.
Breast MPC-620Breast Multiple Primary Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)questionDecisionNoteFlow Direction* Prepare one abstract. Use the histology coding rules to assign the appropriate histology code.** Prepare two or more abstracts. Use the histology coding rules to assign the appropriate histology code to each case abstracted.DECISIONMULTIPLE TUMORS, continuedNOTES1. Includes combinations of in situ and invasive.2. Tumors are not described as a metastasis.Site-Specific Coding ModulesDo the tumors have ICD-O-3 histologyYESMULTIPLEPrimaries**codes that are different at the first (xxxx),second (xxxx), or third (xxxx) number?NOM13Does not meet any of theabove criteria(M1 through M12).NOYESSINGLEPrimary*1. When an invasive tumor follows an in situtumor within 60 days, abstract as a single primary.2. All cases covered by Rule M13 have the samefirst 3 numbers in ICD-O-3 histology code.End of instructionsfor Multiple Tumors.ERROR: Recheck rules.Stop when a match is found.Appendix CRule M13 Examples: The following are examples of cases that use Rule M13.This is NOT intended to be an exhaustive set of examples; there are other cases that may be classified as a single primary.Warning: Using only these case examples to determine the number of primaries can result in major errors.Example 1. Invasive duct and intraductal carcinoma in the same breastExample 2. Multicentric lobular carcinoma, left breastSEER Program Coding and Staging Manual 2007M12
Appendix CBreast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: IN SITU CARCINOMA ONLY(Single Tumor; all parts are in situ)ActionRuleH1Code thehistologydocumentedby thephysicianNOH2Is only one histologic typeidentified?NOC-621NextPageBreast HistoYESCode thehistology.1. Priority for using documents to code the histologyDocumentation in the medical record that refers topathologic or cytologic findingsPhysician's reference to type of cancer (histology)in the medical record2. Code the specific histology when documented.SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesYESIs the pathology/cytologyreport unavailable?Notes and Examples
Breast HistoC-622Breast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: IN SITU CARCINOMA ONLY(Single Tumor; all parts are in situ)RuleH3ActionYESNOSite-Specific Coding ModulesIs there adenocarcinoma in situ,NOS (8140) and a specificadenocarcinoma in situ?YESCode themorespecifichistologicterm.The specific histology may be identified as type, subtype,predominantly, with features of, major, or withdifferentiation, architecture or pattern.The terms architecture and pattern are subtypes only forin situ cancer.NOIs there intraductal NOS (8500)and a specific intraductalcarcinoma (Table1)?YESNOH4Does the tumor have non-infiltratingcomedocarcinoma and any otherintraductal carcinoma (Table 1)?YESCode 8501/2(comedocarcinoma, noninfiltrating).NOH5Does the tumor have a combinationof in situ lobular (8520) andintraductal carcinoma (Table 1)?Appendix CNONextPageYESCode 8522/2(intraductaland lobularcarcinomain situ) (Table 3).Example: Pathology report reads intraductalcarcinoma with comedo and solid features. Codecomedocarcinoma (8501/2).SEER Program Coding and Staging Manual 2007Is there carcinoma in situ, NOS (8010)and a specific carcinoma in situ?Notes and Examples
Appendix CBreast Histology Coding Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: IN SITU CARCINOMA ONLY(Single Tumor; all parts are in situ)RuleActionNotes and ExamplesSite-Specific Coding ModulesIs there a combination of intraductal carcinomaand two or more specific intraductal types ORare there two or more specificintraductal carcinomas?YESCode 8523/2(intraductalcarcinoma mixedwith other typesof in situcarcinoma)(Table 3).2. Change the behavior to 2 (in situ) inaccordance with the ICD-O-3 matrix principle(ICD-O-3 Rule F).NOH7Is there in situ lobular (8520) and any insitu carcinoma other than intraductalcarcinoma (Table 1)?YESCode 8524/2(in situ lobularmixed with othertypes of in situcarcinoma)(Table 3).Change the behavior to 2 (in situ) in accordancewith the ICD-O-3 matrix principle (ICD-O-3 Rule F).NOH8Is there a combination of insitu/non-invasive histologies that does notinclude either intraductal carcinoma(Table 1) or in situ lobular (8520)?YESC-623This is the end of instructions for Single Tumor: In Situ Carcinoma Only.Code the histology according to the rule that fits the case.Breast HistoCode 8255/2(adenocarcinomain situ with mixedsubtypes(Table 3).Change the behavior to 2 (in situ) in accordancewith the ICD-O-3 matrix principle (ICD-O-3 Rule F).SEER Program Coding and Staging Manual 20071. Use Table 1 to identify the histologies.H6
Breast HistoC-624Breast Histology Coding Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: INVASIVE AND IN SITU CARCINOMA(Single Tumor; in situ and invasive components)RuleActionNotes and ExamplesSite-Specific Coding ModulesH9Does the tumor have invasive andin situ components?YESCode theinvasivehistology.NOERROR: Confirm Multiple PrimaryRule application and then go toH1 - H8 or H10 - H29Appendix CThis is the end of instructions for Single Tumor: Invasive and In Situ Carcinoma.Code the histology according to the rule that fits the case.2. This is a change from the previous histologycoding rules and is different from ICD-O-3 rules. Thischange was made in collaboration with the ICD-O-3editors. The consensus was the invasive componentof the tumor better explains the likely disease courseand survival category. Using these new rules,combinations of invasive duct and in situ lobular arecoded to invasive duct (8500/3) rather than thecombination code for duct and lobular carcinoma(8522/3)SEER Program Coding and Staging Manual 20071. Ignore the in situ terms.
Appendix CBreast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: INVASIVE CARCINOMA ONLY(Single Tumor; all parts are invasive)ActionRuleSite-Specific Coding ModulesIs there no pathology/cytologyspecimen or is thepathology/cytology reportunavailable?YESCode thehistologydocumentedby thephysician.1. Priority for using documents to code the histologyDocumentation in the medical record that refers topathologic or cytologic findingsPhysician's reference to type of cancer (histology) inthe medical recordMammogramPET scanUltrasound2. Code the specific histology when documented.3. Code the histology to 8000 (cancer/malignantneoplasm, NOS) or 8010 (carcinoma, NOS) as stated bythe physician when nothing more specific is documented.NOH11Is the only specimen from ametastatic site?(there is no pathology/cytologyspecimen from the primary site)NOC-625NextPageBreast HistoYESCode thehistologyfrom themetastaticsite.Code the behavior /3.SEER Program Coding and Staging Manual 2007H10Notes and Examples
Breast HistoC-626Breast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: INVASIVE CARCINOMA ONLY(Single Tumor; all parts are invasive)RuleIs there carcinoma, NOS (8010) and amore specific carcinoma?Notes and ExamplesYESNOYESSite-Specific Coding ModulesIs there adenocarcinoma, NOS (8140)and a more specific adenocarcinoma?NOIs there duct carcinoma, NOS (8500) anda more specific duct carcinoma (8022,8035, 8501-8508)?YESCode themostspecifichistologicterm.The specific histology may be identified as type,subtype, predominantly, with features of, major, orwith differentiation. The terms architectureand pattern are subtypes only for in situ cancer.NOYESIs there sarcoma NOS (8800) and amore specific sarcoma ?NOH13Does the final diagnosis of thepathology report specifically stateinflammatory carcinoma?Appendix CNONextPageYESCode 8530(inflammatorycarcinoma).Record dermal lymphatic invasion in CollaborativeStaging.SEER Program Coding and Staging Manual 2007H12Action
Appendix CBreast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: INVASIVE CARCINOMA ONLY(Single Tumor; all parts are invasive)RuleActionNotes and ExamplesIs only one histologic typeidentified?YESCode thehistology.Site-Specific Coding ModulesNOH15YESAre there two or more specific ductcarcinomas?Code thenumericallyhigherICD-O-3histology code.Use Table 2 to identify duct carcinomasNOH16Use Table 2 to identify duct carcinomasIs there a combination of lobular (8520)and duct carcinoma (Table 3)?NONextPageC-627Breast HistoYESCode 8522(ductand lobular).SEER Program Coding and Staging Manual 2007H14
Breast HistoC-628Breast Histology Coding Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionSINGLE TUMOR: INVASIVE CARCINOMA ONLY(Single Tumor; all parts are invasive)RuleAction1. Use Table 2 to identify duct carcinomas.Site-Specific Coding ModulesIs there a combination of duct and anyother carcinoma (Table 3)?YESCode 8523(duct mixedwith othertypes ofcarcinoma).2. Other carcinomas exclude lobular and any ductcarcinoma listed on Table 1 or Table 2.NOH18Does the tumor have lobular (8520) andany other carcinoma (Table 3)?YESCode 8524(lobular mixedwith othertypes ofcarcinoma).Other carcinomas exclude lobular and any ductcarcinoma listed on Table 1 or Table 2.NOH19Are there multiple histologies that donot include duct or lobular (8520)?YESCode 8255(adenocarcinoma withmixedsubtypes)(Table 3).Appendix CThis is the end of instructions for Single Tumor: Invasive Carcinoma Only.Code the histology according to the rule that fits the case.Use Table 2 to identify duct carcinomasSEER Program Coding and Staging Manual 2007H17Notes and Examples
Appendix CBreast Histology Coding Rules - Flow chartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionMULTIPLE TUMORS ABSTRACTED AS A SINGLE PRIMARYRuleActionH20YESCode thehistologydocumentedby thephysician.1. Priority for using documents to code the histologyDocumentation in the medical record that refers topathologic or cytologic findingsPhysician's reference to type of cancer (histology) inthe medical recordMammogramPET ScanUltrasound2. Code the specific histology when documented.3. Code the histology to 8000 (cancer/malignantneoplasm, NOS) or 8010 (carcinoma, NOS) as stated bythe physician when nothing more specific is documented.NOH21Is the only specimen from ametastatic site?(there is no pathology/cytologyspecimen from the primary siteYESCode thehistologyfrom ametastaticsite.Code the behavior /3.NOH22Does the final diagnosis of thepathology report specifically stateinflammatory carcinoma?NOC-629NextPageBreast HistoYESCode 8530(inflammatorycarcinoma).Record dermal lymphatic invasion in CollaborativeStaging.SEER Program Coding and Staging Manual 2007Site-Specific Coding ModulesIs there no pathology/cytologyspecimen or is thepathology/cytology reportunavailable?Notes and Examples
Breast HistoC-630Breast Histology Coding Rules - FlowchartFlowchart Key(C500-C509)(Excludes lymphoma and leukemia M9590-9989 and Kaposi sarcoma M9140)RuleActionNotes andExamplesFlow DirectionMULTIPLE TUMORS ABSTRACTED AS A SINGLE PRIMARYRuleH23ActionYESCode thehistology.NOH24Site-Specific Coding ModulesDoes the pathology report specifically state thatthe Paget disease is in situ and the underlyingtumor is intraductal carcinoma (Table 1)?YESCode 8543/2(in situ Pagetdisease andintraductalcarcinoma(Table 3).Change the behavior to 2 (in situ) in accordance withthe ICD-O-3 matrix principle (ICD-O-3 Rule F).NOH25YESIs there Paget disease andintraductal carcinoma (Table 3)?Code 8543/3(Paget diseaseand intraductalcarcinoma).1. ICD-O-3 classifies all mammary Paget disease as amalignant process with a malignant behavior (/3).2. Includes both invasive Paget disease and Pagetdisease with behavior not stated.3. Use Table 1 to identify intraductal carcinomas.NOH26YESIs there Paget disease and invasiveduct carcinoma (Table 3)?Appendix CNONextPageCode 8541/3(Paget diseaseand infiltratingductcarcinoma).1. ICD-O-3 classifies all mammary Paget disease as amalignant process with a malignant behavior (/3).2. Includes both invasive Paget disease and Pagetdisease with behavior not
Table 3 - Combination Codes for Breast Cancers . Use this two-page table with rules H5, H6, H7, H8, H16, H17, H18, H19, H24, H25, H26 and H28 to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the case using the ICD-O-3 histology code in column 4.