Transcription
Schema Therapy for EatingDisorders: Working withentrenched patterns & complexityANZAED WebinarDr. Susan Simpson, Clinical PsychologistAdvanced Schema Therapy TrainerSchema Therapy ScotlandE: info@schematherapyscotland.com1Schema Therapy for Eating Disorders Routledge,20192Programme Current treatment gaps for eating disorders Factors affecting outcome Rationale: Schema Therapy for Eating Disorders Evidence to date Schema Therapy model for Eating Disorders Case example - Karen31
Why schema therapy for eatingdisorders? Current treatment gaps for eating disorders: CBT for BN – 25% drop out, & of those who do not drop out50% recover (Agras, et al., 2007). CBT-E –transdiagnostic model (Fairburn, 2009; Byrne et al, 2011) Reduction in ED symptoms: 56% of completers in fullremission Attrition rates: 50% (AN); 35% (BN); 37.3% EDNOS Need to consider treatment models that can address morecomplex needs of those who do not respond to standardtreatments (Jones, Leung, & Harris, 2007).4Why schema therapy for eatingdisorders? Eating disorders (ED) are severe psychiatric illnesses Co-morbidity of ED: Up to 69% meet DSM criteria for PD Up to 93% have concurrent Axis I disorder (Blinder et al., 2006) Individuals with ED commonly experience complex & difficultto-treat symptomatology including dissociation, perfectionism,compulsive pathology, rigid thinking patterns & high levels ofshame (Leung et al., 2000; Waller, et al., 2007; Fairburn, 2008).5Eating Disorder Personality DisorderComorbidity OutcomesANPDHigherAttrition PoorerOutcomesBEDCluster CPoorerOutcomesBNPDless likelyto impactED SpecificOutcomes62
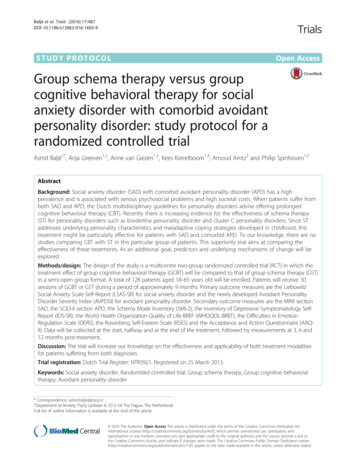
Trait Comorbidity & ED SeverityIm pulsivityPersistenceNoveltySeekingCom stabilityNeuroticismPerfectionism7Multiple Pathways to Eating DisordersTemperament&Body FactorsCulture*Emotionallyinhibited, ‘manup’ cultureTem peram ent:Em path,Sensitive,Perfectionistic,Com pulsivity/im pulsivityBody Factors:Body interoceptiveawareness*Emphasis onappearance,achievement &material success,autonomy, atexpense of‘presence’ &connection*Fat phobia, dietcultureChildhoodExperience*Emotionally absent,cold, misattunement,invalidatiion*Parenting: GuiltInducing, Enmeshed*Demanding, * Critical,*Overcontrolling*Abusive* Sibling difficulties requiringdisproportionate parental attention (e.g.disabilities, ADHD,)*Peer attitudes/bullying*Body-sexualobjectification*Fam ily attitudes toeating/weight/shape8Parental Bonding in EDsThe role ofAttachment& ParentalBonding(systematicreviews): Lower parental care; Higher paternalprotectiveness (O’Kearney, 1996; Tetley et al,2014; Ward et al., 2000) Insecure attachment style & separationanxiety (Ward et al, 2000) Higher parental control; Lower affection(affectionless control) (Ward et al, 2000) Mediating factors – Low self efficacy; EMS(defectiveness, abandonment & vulnerabilityto harm); avoidant coping (Tetley et al, 2014)Attachment in EDs (O'Shaughnessy & Dallos, 2009; Ward etal., 2000; Zachrisson & Skarderud, 2010) AN has strongest association with AvoidantAttachment BN has strongest association withPreoccupied attachment style93
Childhood Trauma & Eating Disorders(EDs) Childhood sexual, physical & emotional abuse operate as risk factors andsignificant predictors or ED psychopathology (Caslini et al, 2016; Kong et al, 2009; Racine & W ildes, 2015;Sanci et al., 2008). Emotional abuse & invalidation are strongest predictors of ED severity ( CSA and physicalabuse) (Kent, W aller & Dagnan, 2007; Leung et al, 2009; Turner et al, 2004; W aller, Corstorphine, & M ountford, 2007)10Why talk about developmental issues? Clients need to understand that “they didn’t comeup with this on their own” & the role of experiencein developing beliefs. Helps generate insight to core problems Helps make problems ego dystonic, so they can“fight against the belief” Helps to differentiate “vulnerable states” fromcoping states and Inner Critic (‘old’ core belief)states1111Schema Therapy: ResearchEvidenceEffective with: Borderline Personality Disorder (Giesen-Bloo et al., 2013) Cluster C Personality Disorders (Bamelis et al., 2014) Chronic Depression (Carter et al., 2013) Substance Abuse (Ball, 1998) Agoraphobia (Bamber, 2004) PTSD (Young, 2005)124
Schema Therapy is effective forBorderline & Cluster C PersonalityDisorders Giesen-Bloo et al.(2006). Outpatient psychotherapy for borderline personalitydisorder. Randomized trial of Schema-Focused Therapy versus Transference-FocusedPsychotherapy. Archives of General Psychiatry,63, 649-658. Nadort et al. (2008, 2009). Implementation of outpatient schema therapy forborderline personality disorder: study design. BMC Psychiatry, 9:64. Farrell, Shaw & Webber (2009). A schema-focused approach to group psychotherapyfor outpatients with borderline personality disorder: a randomized controlled trial.40(2): 317-28. Carter, J. et al. (2013). Psychotherapy for depression: a randomized clinical trialcomparing schema therapy and cognitive behavior therapy. Journal of AffectiveDisorders, 151, 500-505. Bamelis et al. (2014). Results of a multicenter randomized controlled trial of theclinical effectiveness of schema therapy for personality disorders. Am J Psychiatry.1;171(3):305-22.13Preliminary treatment studies:Schema Therapy for EDs McIntosh, V. et al. (2016) Psychotherapy for transdiagnostic bingeeating: A randomized controlled trial of cognitive-behaviouraltherapy, appetite-focused cognitive-behavioural therapy, and schematherapy. Psychiatry Research, 240, 412-420. Simpson et al (2010) Group Schema Therapy for Eating Disorders:A pilot study. Frontiers in Psychology, 1, 182. Calvert, F., Smith, E., Brockman, R., & Simpson, S. (2018). Groupschema therapy for eating disorders: study protocol. Journal ofEating Disorders 6, 1-7. Simpson & Slowey (2011). Video Therapy for Atypical EatingDisorder and Obesity: A Case Study. Clinical Practice andEpidemiology in Mental Health 7(1):38-4314What is Schema Therapy? An integrative, unifying theory & treatment Designed for clients with complex, chronic, entrencheddifficulties, including PDs With significant origins in childhood & adolescentdevelopment Use when clients describe the problem as “this is the way Iam/ have always been” When CBT gets ‘stuck’155
Schema Therapy expands on traditional CBT byplacing more emphasis on: The therapeutic relationship Longer term treatment focus More emphasis on affect (e.g., through imagery, roleplaying) and mood states More discussion of childhood origins anddevelopmental processes More emphasis on lifelong coping styles (e.g.avoidance and overcompensation More emphasis on entrenched core themes (i.e.,schemas & modes)16Schema Therapy- 2 Models1) Schema Model- 18 maladaptive schemas Working with individual schemas/beliefs & coping styles More high functioning, less complex problems2) Schema Mode Model Collapsing schemas/ coping styles into modes/ sides of self. Used for Personality Disorders & more “dug in”, complex presentations17Five Core Emotional Childhood Needs Secure attachments to others (includes safety,stability, nurturance and acceptance) Autonomy, competence and sense of identity Freedom to express valid needs and emotions Spontaneity and play Realistic limits and self-control18186
Schema Mode Model Child modes – Refers to our innate vulnerability, or Inner Child self basic emotions & vulnerability (happiness, anger sadness, anxiety) Coping modes: Dissociated parts of self developed to survive/cope with mismatchbetween temperament & environment in childhood Survival strategies: fight – flight – freeze Inner Critic modes: Internalised messages from childhood (family, culture & unmetemotional needs)Punitive – demanding – guilt inducing Healthy adult19Phase 1: Assessment: SchemaModesADULTCHILDCOPING20Child Modes – Adapted for EDsShamed/Deprived Child Rejected, hurt, shamed, unwanted, anxious, lost, unattractive, inferior Desperate for nurturance, protection & attentionImpulsive/Rebellious Child Can never get enough of what they need. Impulsive binge eating, DSH Rebels against control, acts on impulsesAngry Child Intensely angry because emotional needs not being met Anger usually suppressed. Expressed through passive-aggressive meansHappy Child Body as a positive part of ‘self’ Uses body appropriately for play, express feelings, pleasurable activities217
Internalised Inner Critic nerableChild22Inner Critic Mode Messages: Try harder that’s not good enough Where is the extra 10%? You should have done more Cant you see how your being ill is hurting everyone? You’re too selfish/self-indulgent/greedy. You’re too needy. You’re undeserving You are a monster, barely human. You are disgusting, horrible, completely unlovable. You are pathetic.23Coping Modes – Adapted for EDsCompliantSurrendererSurrenderer d248
Coping Modes – Adapted for her25Coping Modes – Adapted for ionisticOver-controller279
Hypothesised developmental originsof schemas/ core beliefsEnvironmentTemperament Culture, body objectification Media, Parenting style, family beliefs aroundfood/weight/shape Availability of emotional support offamily & wider system Peer pressures Messages from teachers, wider family Experiences of abuse, trauma, neglect Sensitive/Anxious High empathy Low tolerance foruncertaintyNeedsmet/unmetSchemas Maladaptive Modes28Coping ModesChild ModesVulnerable“Child” modeCore feelings- pain,anxiety, empty,sad,shame lonely etcDetaching/ emotionalavoidanceDetached, emotionallyavoidant, “rational”,“out of touch”Parent Modes1) Punitive Parent“internal “you’reBad mode”2)Demanding ParentCompliant Surrender, pressure!!“Happy/ smiling”, goesdemandingalong with, doesn’t standupHealthy AdultOvercompensationmodes-Aggrandising-A Perfectionistovercompensation-Bully/ attack2929Inner Criticshamesthe InnerVulnerableChild3010
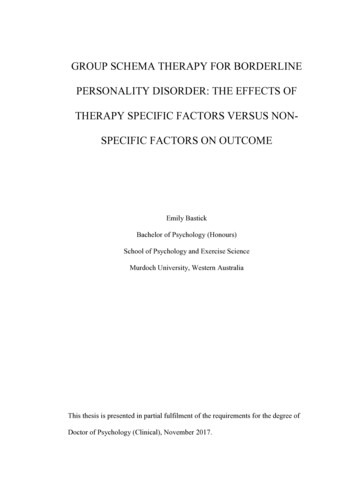
Karen: Presenting Issues Anorexia Nervosa (restricting) Compulsive over-exercise OCD – handwashing, counting, checking rituals Chronic dysthymia Self-harm – cutting Avoidant Personality Disorder31Childhood ExperiencesMum anxious, depressed; Dad critical, controllingTemperament: Lack of closeness/attachment difficulties;Parents preoccupied with their conflicts/problems – separated whenShy, anxiousKaren was 9 years oldMum absent, working long hours, extra-marital affairDad angry, ‘exasperated’, negative, ‘shouty’Mum disapproving; Father distant, rigid, self-focused.Bullied & ostracized at schoolsKarenUnmet needs: Lack of close attachment, attunement, emotional availability &warmth, empathy, praise, help with managing anxiety & fears .Core Beliefs/SchemasSocial Isolation: I am weird; I’m different from othersSubjugation: I must submit to the control of others or I will be punishedAbandonment: Others will leave me. In the end I’ll be all aloneEmotional Deprivation: No-one will ever meet my emotional needsUnrelenting Standards: Nothing I do is good enough; I must avoid mistakes at all costsDefectiveness: I am disgusting, unlovable, worthless, evil, undeserving. I’m wrong tomy core. I’m bad – an imposter in my own body.Mistrust/Abuse: Others will judge/hurt me.32Karen Mode MapPerfectionisticOvercontrollerInner Critic (Punishing)ModeYou’re so weak & pathetic.You’ve eaten too much.You’re bad, dirty, aNo you’re wrongYou’re a problemYour needs/feelings are aburdenYou’re undeservingYou’re too needyYou’re differentRestriction of eatingPerfectionistic,productive, busy,achievement-focused.Rituals, exercise,Self-HarmSelf-punishment – asatonement, selfflagellation.Annihilation of ownneeds/feelings to makeself ‘invisible’Compliant SurrendererPassive, compliant, selfsacrificingLittle Karen Anxious, guilty,sad, lonely,dependent,stressed, rejectedtrapped, aburden, hopeless,powerless, guilty.Angry ChildInternalisedtoward bodyHealthyAdult3311
Treatment with Schema TherapyThe overall goal is to help patients find adaptive waysto meet their core emotional needs and engage inschema healing via: Experiential techniques: chair work, imagery re-scripting.Interpersonal Work: attunement, connecting withvulnerability underneath ‘rational’ & ‘detached’ copingmodesCognitive work with Core BeliefsStrong behavioural component34Schema Therapy: Broad Goals Help clients get their core needs met In an adaptive Manner; By cultivating the Healthy Adult; Through changing Maladaptive Schemas (EMS) Coping styles/responses Modes35Phase 2: Change ProcessesEnhance adaptive coping by cultivating the Healthy AdultLimited Re-parentingImagery RescriptingChair/Mode WorkCognitive TechniquesBehavioural Pattern Breaking3612
Goals: Working with ED modesPunishing InnerCriticEmpathically confrontDetachedSelf SootherConfront,set limitsOvercontrollerVulnerable,Impulsive &Angry, childNurture,validate,heal, setlimitsHealthyAdultStrengthen,EmpowerHappy Child37Summary:How is Schema Therapy different? Integrative Active focus on mentalising deeper level thoughts/feelings Structured, utilises broad range of strategies Developmental model: Focus on attachment & childhoodneeds Emphasis on evoking affect rather than rationalisingemotions – goes beyond intellectual change ‘Reparenting’ meeting some of patients’ needs asantidote to EMS whilst avoiding gratifyication of copingmodes Builds Healthy Individuated Self from ‘inside out’38Common Pitfalls Questions?3913
Relevant references Brown, et al. (2016). Do dysfunctional coping modes mediate therelationship between perceived parenting style and disordered eatingbehaviours? Journal of Eating Disorders, 4(27):1-10. Calvert, et al. (2017). Group schema therapy for eating disorders: Studyprotocol. Journal of Eating Disorders, 6(1):1. Edwards, D. (2017a). An Interpretative Phenomenological Analysis ofSchema Modes in a Single Case of Anorexia Nervosa: Part 1 –Background, Method, and Child and Parent Modes. Indo-PacificJournal of Phenomenology, 17(1) Edwards, D. (2017b). An Interpretative Phenomenological Analysis ofSchema Modes in a Single Case of Anorexia Nervosa: Part 2 – CopingModes, Healthy Adult Mode, Superordinate Themes, and Implicationsfor Research and Practice. Indo-Pacific Journal of Phenomenology,17(1). George et al. (2004). Motivational enhancement and schema-focusedcognitive behaviour therapy in the treatment of chronic eating disorders.Clinical Psychologist, 8(2), 81-85. Hodge & Simpson (2016). Speaking the Unspeakable: Artistic Expression inEating Disorder Research and Schema Therapy. The Arts in Psychotherapy,50, 1-8.40References McIntosh, V. et al. (2016) Psychotherapy for transdiagnostic binge eating: Arandomized controlled trial of cognitive-behavioural therapy, appetite-focusedcognitive-behavioural therapy, and schema therapy. Psychiatry Research, 240,412-420. Pugh. M. (2015). A narrative review of schemas and schema therapyoutcomes in the eating disorders. Clinical Psychology Review, 39:30-41. Simpson, S. (2012) Schema Therapy for Eating Disorders: A case studyillustration of the mode approach. In M. van Vreeswijk, J. Broersen & M.Nadort (Eds.) The Wiley-Blackwell Handbook of Schema Therapy: Theory,Research and Practice. Simpson et al (2010) Group Schema Therapy for Eating Disorders: A pilotstudy. Frontiers in Psychology in Clinical Settings, Vol 1, Article 182. Simpson, S. & Slowey, L. (2011). Video Therapy for Atypical Eating Disorder &Obesity: A Case Study. CPEMH, 7, 38-43. Simpson et al. (2018) Factorial Structure and Preliminary Validation of theSchema Mode Inventory for Eating Disorders (SMI-ED). Front. Psychol., 9,DOI:10.3389/fpsyg.2018.00600 Waller, G., Kennerley, H., & Ohanian, V. (2007). Schema-focused cognitivebehavioural therapy for eating disorders. In J. Rodin, P. L. du Toit, D. J. Stein, &J. E. Young (Eds.), Cognitive Schemas and Core Beliefs in PsychologicalProblems: A Scientist-Practitioner Guide (pp. 139-175). Washington, DC: APA.41Reviews:Evidence Base for Schema Therapy Bakos, D.S., Gallo, A.E. & Wainer, R. (2015). Systematic review of the clinicaleffectiveness of schema therapy. Contemp Behav Health Care, 1. Hopwood, C. & Thomas, K. (2014). Schema therapy is an effective treatment foravoidant, dependent and obsessive-compulsive personality disorders. Evid BasedMent Health;17(3):90-1 Jacob, G., Arntz, A. (2013) Schema Therapy for Personality Disorders – A Review.International Journal of Cognitive Therapy 6(2), 171-185. Masley, S., Gillanders, D., Simpson, S., Taylor, M. (2011). A systematic review ofthe evidence base for schema therapy. Cognitive Behaviour Therapy. 31, 185-202 Pugh. M. (2015). A narrative review of schemas and schema therapy outcomes inthe eating disorders. Clinical Psychology Review, 39:30-41. Sempertegui, G.A., Karreman, A., Arntz, A. & Bekker, M. (2012). Schema therapyfor borderline personality disorder: a comprehensive review of its empiricalfoundations, effectiveness and implementation possibilities. Clinical PsychologyReview, 33(3), 426-447.4214
For online workshop details on SchemaTherapy for Eating achable.com/*www.schematherapyscotland.comComing 15
Nadortet al. (2008, 2009). Implementation of outpatient schema therapy for borderline personality disorder: study design. BMC Psychiatry, 9:64. Farrell, Shaw & Webber (2009). A schema-focused approach to group psychotherapy for outpatients with borderline personality disorder: a randomized controlled trial. 40(2): 317-28. Carter, J. et al. (2013).