Transcription
National Health Screening Guideline onNoncommunicable Diseases (NCDs)Ministry of HealthBrunei DarussalamNovember 2019 EditionNoncommunicable Diseases (NCDs) Prevention Unit, Ministry of HealthPage 1 of 36
Table of ContentsBackground Information . 3Existing Health Screening Programmes in Brunei Darussalam . 4Levels of Recommendation on Health Screening . 5Levels of Evidence . 6Selected Conditions for Population-based Screening . 7Breast cancer . 9Cervical cancer . 10Colorectal cancer . 11Liver cancer (Hepatocellular Carcinoma) . 12Nasopharyngeal cancer (NPC) . 13Prostate cancer. 14Diabetes Mellitus . 16Hyperlipidaemia . 18Hypertension . 19Obesity . 20Vascular Conditions: Atherosclerotic Cardiovascular Disease (ASCVD) . 21Abdominal Aortic Aneurysm . 24Anaemia (Iron Deficiency) . 25Dementia . 26Depression (Children & Adults) . 27Renal Impairment / Chronic Kidney Disease . 28Appendix 1: Body Mass Index (BMI) Classification . 29Acknowledgement . 30Literature Review on Established Policies of Health Screening . 30References . 31Page 2 of 36
Background InformationHealth Screening“Screening is defined as the presumptive identification of unrecognized disease in anapparently healthy, asymptomatic population by means of tests, examinations or otherprocedures that can be applied rapidly and easily to the target population” (WHO)Criteria for an effective screening test as according to The Wilson & Jungner ClassicScreening Criteria:1.2.3.4.5.6.7.The condition sought should be an important health problemThere should be an accepted treatment for patients with recognized diseaseFacilities for diagnosis and treatment should be availableThere should be a recognizable latent or early symptomatic stage.There should be a suitable test or examination.The test should be acceptable to the population.The natural history of the condition, including development from latent todeclared disease, should be adequately understood.8. There should be an agreed policy on whom to treat as patients.9. The cost of case-finding (including diagnosis and treatment of patientsdiagnosed) should be economically balanced in relation to possibleexpenditure on medical care as a whole.10. Case-finding should be continuing process and not a “once and for all” projectScreening expectationsWhen screening for a disease or condition, depending on the sensitivity and specificityof the screening tools used, may result in false positive or false negative results: False positive – wrongly reported as having the conditionFalse negative – wrongly reported as not having the conditionScreening can: Save lives or improve quality of life through early identification of a conditionReduce the chance of developing a serious condition or its complicationsScreening does not guarantee protection. Receiving a low chance results does notprevent the person from developing the condition at a later date.Page 3 of 36
As part of the Government of His Majesty The Sultan and Yang Di-Pertuan of BruneiDarussalam’s continuous effort to strengthen the planning, enhance quality and developthe country’s health care system, and in alignment to the Wawasan Brunei 2035 and theMinistry of Health’s vision ‘Together Towards a Healthy Nation’, several key strategiesand initiatives have been identified, development and implementation of populationbased health screening for key noncommunicable diseases (NCDs) were one of the keyinitiatives that have been identified.As part of the Health Screening initiative, a technical workgroup on development ofNCDs screening guideline was formed, it was represented by experts and specialistsfrom various departments in the RIPAS Hospital, Primary Health Care, Public Healthand Laboratory Services, chaired by Deputy Permanent Secretary (Professional). Theobjectives were to review the current health screening programmes and guidelines, toidentify any update need to be made in light of latest evidence-based literature and localdisease prevalence, and to develop a comprehensive NCDs screening guideline forBrunei Darussalam. This document will serve as a recommendation guideline forclinicians to refer to when considering NCD screening methods and also to guide policymakers in implementing national screening programmes based on latest evidences.The committee had several meetings and consultations to review local diseaseprevalence and incidences, current screening practices in Brunei and overseas in orderto develop health screening policy framework, and matrix of the health screeningrecommendation.Existing Health Screening Programmes in Brunei DarussalamChildren: Neonatal health screeningSchool health screeningAdults: Antenatal health screeningOccupational health screeningCervical cancer screening (Well Women clinics)Opportunistic health screening (Hospitals and private clinics)Page 4 of 36
Levels of Recommendation on Health ScreeningThe following levels of recommendation are used in this health screening guideline forNCDs (Table 1). This is to serve as a guideline for clinicians when considering varioushealth screening options for their patients and to take into consideration of individualrisk factors and other clinical assessment. The health screening recommendations areto updated when new evidence or disease information emerges.Table 1: Three Levels of Recommendation on Health ScreeningLevelDefinitionSuitable for populationbased screeningGood evidence that the screening test is both clinicallyeffective and cost-effective for use in screening thepopulationNet benefit does not always outweigh the risk in generalpopulations, but screening may be useful for high-riskpopulationsSuitable for individuallevel decision or high risk ORscreeningEvidence suggests that the screening test is effective butits cost-effectiveness has not yet been evaluated or itsoutcome is unfavourableThere is lack of evidence to make a decision regardingthe usefulness of the testNot recommended forscreeningORGood evidence suggests that the screening test isineffective, or that the net harm outweighs the benefitsPage 5 of 36
Levels of EvidenceIEvidence from meta-analyses, systematic reviews of randomised controlledtrials (RCTs), or RCTsIIEvidence from systematic reviews of case control or cohort studies or any casecontrol or cohort studiesIIIEvidence from non-analytic studies, e.g. case reports, case seriesIVExpert opinion, formal consensusAdapted from The National Institute for Health and Care Excellence (NICE) levels of evidencePage 6 of 36
Selected Conditions for Population-based ScreeningThis guideline contains recommendation for population-based screening for thefollowing group of conditions.1. Cancers2. Cardiovascular Diseases (CVD) and Risks3. Other Noncommunicable Diseases (NCDs)Page 7 of 36
CancerPage 8 of 36
Breast cancerPopulationRecommendation andrationale(if rval ortimingFemales aged 70 years old andaboveCurrent evidence insufficientBreast awareness for normalto assess the balance ofNormal risk and asymptomatic,risk and asymptomaticbenefits and harms of screeningscreen with mammographymammography.Screening start at aged 25-30 every three yearsSubject to clinical assessmentsyears for BRCA mutationof patient’s conditions and riskcarriersfactorsRisk factors associated with breast cancer include early menarche, late menopause, later age at firstpregnancy, nulliparity or low parity, not breastfeeding, high body mass index at postmenopausal age, tallstature, low physical activity levels, alcohol consumption, certain exogenous hormone therapies, historyof proliferative benign breast conditions, advancing age, having a parent, sibling, or child with history ofbreast cancer, known underlying genetic mutation (BRCA1 or BRCA 2 genetic mutation or other familialbreast cancer syndrome) and history of chest radiation therapy at a young ageFemales under 40 years oldCBE, Ultrasound,Mammography, MRICBE – every 6 – 12 monthMammography – annuallyMRI – annually (in addition tomammography)Females aged 40 - 69 years oldMammographyMammographyEvery three yearsSubject to clinical assessmentEvidenceIVIstrengthAbbreviations: CBE, clinical breast exam; MRI, magnetic resonance imagingIVPage 9 of 36
Cervical cancerPopulationRecommendation andrationale(if rval ortimingEvidencestrengthAge 19 years old oryoungerScreening notrecommendedAge 20 - 65 years oldAge above 65 years old & havehad prior screening & not highriskFor those aged 20 to 29 years:Screen with Pap Test alone every 3yearsScreening not recommendedFor those aged 30 to 65 years:Screen with Pap Test every 3 yearsOR; with high-risk HPV testing aloneevery 5 years OR; co-testing (Pap Test& HPV testing) every 5 yearsRisk factors include having human papillomavirus (HPV) infection, multiple sexual partners, earlysexual intercourse ( 17 years old), prolonged use of oral contraceptive, multiparous, young pregnancy(before 17 years old), smoking, history of a compromised immune system, in-utero exposure todiethylstilbestrol, and previous treatment of a high-grade precancerous lesion or cervical cancer.--Pap Test /- hrHPV testing-Every 3 years or 5 years (see above)-III & IIIVPage 10 of 36
Colorectal cancerPopulationBelow 50 years oldAge 50 - 75 years oldAge 76 - 85 years old86 years andaboveDo not automaticallyscreenRecommendation andrationale(if any)Individuals with riskfactors may needscreening before age50 yearsFor those at normal risk andasymptomatic, screeningrecommendedScreening is appropriate forNotadults that are healthyenough to undergo treatment recommendedshould colorectal cancer befound; if they do not havecomorbid conditions.RiskAssessmentAssociated risk factors include older age, male gender, history of adenoma or serrated polyps orcolorectal cancer, history of inflammatory bowel disease and family history for colorectal cancer oradvanced adenoma (high grade dysplasia, 1cm, villous or tubulovillous histology) and family historyof known genetic disorders that predispose to a high lifetime risk of colorectal cancer (such as Lynchsyndrome or familial adenomatous nterval ortimingEvery 3 or 5 yearsdepending onindividual risk factorsEvidencestrengthIVFIT, ColonoscopyColonoscopy, FITFIT every 2 years ifnegativeColonoscopy if fit for scope,scope every 10 years ifnegativeColonoscopy for those withpositive FIT or those optedfor scope, scope every 10years if negativeFIT if unfit for scope, every 2years if FIT negativeII--IVPage 11 of 36
Liver cancer (Hepatocellular Carcinoma)PopulationHigh Risk Groups (refer to risk assessment)Recommendationand rationale(if any)Screening recommended for high risk groups onlyRisk AssessmentScreening tool/test:Screening intervalor timingEvidence strengthPatients with chronic hepatitis B infection or liver cirrhosis from other aetiologies (such ashepatitis C, alcohol, non-alcoholic steatohepatitis and other chronic liver diseases) are atincreased risk of developing hepatocellular carcinomaAlpha-FetoProtein (AFP) and Ultrasound Hepatobiliary System (US HBS)Every 6 monthsIIPage 12 of 36
Nasopharyngeal cancer (NPC)PopulationRecommendation andrationale(if any)Risk AssessmentScreening tool/test:Screening interval ortimingEvidence strengthHigh Risk Groups:Family members of NPC patients starting age 30 – 70 years olda) Individuals with a first degree relative (parent, sibling) with NPCb) Individuals with 2 or more relatives with NPCScreening recommended for high risk groups onlyRisk factors include Epstein‐Barr Virus (EBV) infection, specific HLA-antigen haplotypesLifestyle risk factors include smoking and consuming preserved vegetablesTumour marker for NPC , Serology EBV VCA IgA & EBV Ea IgA and NasoendoscopyAnnually for EBV seropositive individuals and triennial for EBV seronegative individualsIIPage 13 of 36
Prostate cancerPopulationHigh risk populationRecommendation &rationale (if any)Screening recommended for high risk groups only based on individual informedchoice/decision makingMay offer early PSA testing in men at elevated risk of having prostate cancer with individualinformed choice and decision making:Risk AssessmentScreening tool/test:Screening interval ortimingEvidence Strength men 50 years of agemen 45 years of age and a family history of prostate cancermen with a PSA level of 1 ng/mL at 40 years of agemen with a PSA level of 2 ng/mL at 60 years of age In consideration of the low sensitivity and specificity of PSA test, patients and cliniciansshould consider the balance of benefits and harms (risk of overdiagnosis and overtreatment)of screening. Clinicians should not screen men who do not express a preference forscreening.PSA testOffer a risk-adapted strategy (based on initial PSA level), with follow-up intervals of 2 years forthose initially at risk: men with a PSA level of 1 ng/mL at 40 years of agemen with a PSA level of 2 ng/mL at 60 years of ageIPage 14 of 36
CardiovascularDiseases and RisksPage 15 of 36
Diabetes MellitusPopulationAdults age 40 and aboveRecommendation andrationale (if any)Screening should begin at age 40 years, and be considered at an earlier age (e.g. 30 years) ifany of the risk factors for diabetes is present.Risk factors for Diabetes Mellitus include (any one of the following): Overweight (body mass index 25.0 kg/m2) / obesity (body mass index 30.0 kg/m2) Hypertension ( 140/90 mmHg) A first degree relative (parent, sibling) with diabetes mellitus Previous gestational diabetes mellitus Coronary heart disease Polycystic ovary disease Dyslipidaemia (HDL cholesterol 1.0 mmol/l, and/or triglyceride level 2.30 mmol/l) Previously identified impaired fasting glycaemia (IFG) or impaired glucose tolerance (IGT)Risk AssessmentScreening tool/test:Note: Biochemical criteria for diagnosis of:o Impaired fasting glycaemia (IFG): FBS/FPG of 6.1 to 6.9mmol/L and (if measured)OGTT 2-hour post glucose 7.8mmol/Lo Impaired glucose tolerance (IGT): FBS/FPG of 7.0mmol/L and OGTT 2-hour postglucose 7.8 and 11.1mmol/Lo Diabetes: FBS/FPG 7.0mmol/L or Random Plasma Glucose 11.1mmol/L or OGTT2-hour post glucose 11.1mmol/L or HbA1c 6.5%(In asymptomatic individuals, performing the test on one occasion is insufficient toestablish diagnosis. One further test must be carried out on a subsequent day to confirmdiagnosis.)Three tests have been used to screen for diabetes: Fasting blood sugar (FBS) / Fasting plasma glucose (FPG) Haemoglobin A1c (HbA1c)* 75-gram oral glucose tolerance (OGTT)** Either of these tests can be used for individuals if FPG/FBS 6mmol/LPage 16 of 36
Screening interval ortiming Every three years with FBS for those with normal glucose tolerance with no risk factorsAnnually with FBS for those with normal glucose tolerance with risk factorsAnnually with FBS for those with impaired fasting glycaemia (IFG) or impaired glucosetolerance (IGT).o To perform 75 gram oral glucose tolerance test every three years for this groupEvidence strengthIVNote: Body Mass Index is calculated using a person's height and weight. The formula is BMI kg/m 2 where kg is aperson's weight in kilograms and m2 is their height in metres squared. E.g. BMI 85kg / (1.7m)2 29.4 kg/m2Page 17 of 36
HyperlipidaemiaPopulationAll adults aged 40 years andaboveRecommendation& rationale (if any)Screening recommended:All individuals 40 years and aboveshould be screened as they havean elevated risk for atheroscleroticcardiovascular diseaseIndividuals aged below 40 years with one or more riskfactors given belowIndividual level decision based on additional risks givenbelowAll adults with the following:Risk AssessmentScreeningtool/test:Screening intervalor timingEvidence StrengthA. Pre-existing atherosclerotic cardiovascular disease(includes atherosclerotic cardiovascular disease,cerebrovascular and peripheral arterial disease)B. Diabetes mellitusC. Impaired fasting glycaemia or impaired glucose toleranceD. Family history of premature atheroscleroticcardiovascular diseaseE. Familial hyperlipidaemiaF. HypertensionG. ObesityH. Smoker (including ex-smokers)I. Chronic inflammatory disease (eg rheumatoid arthritis,psoriasis, HIV)J. Chronic kidney diseaseFasting lipid panel: (Total cholesterol, high-density and low-density lipoprotein cholesterols)Every 3 years: If results of prior cholesterol are normal for patients at low atheroscleroticcardiovascular disease risk of 10% over 10 yearsYearly: If patients at increased riskIIIVPage 18 of 36
HypertensionPopulationRecommendation& rationale (if any)All adults aged 40 years and aboveScreening should begin at age 40 yearsIndividuals aged between 18 years and lessthan 40 yearsScreening should be considered at an earlierage (from 18 years) if felt to be at increasedrisk of hypertension.Individuals with increased risk such as the following:Risk Assessment Renal diseaseDiabetesAtherosclerotic cardiovascular diseaseHyperlipidemiaSmokingObesityFamily of premature cardiovascular disease or hypertension or hyperlipidemiaNote:NORMAL BP is defined as SBP 130mmHg & DBP 79mmHgHIGH NORMAL BP is defined as SBP 130 - 139mmHg with DBP 80-89mmHgHYPERTENSION is defined as SBP 140mmHg & DBP 90mmHgScreeningtool/test:Screening intervalor timingEvidence StrengthBlood pressure measurement in clinicAnnual screeningIPage 19 of 36
ObesityPopulationChildren aged 6 years and older &AdolescentsAdults aged 18 years or olderRecommendation andrationale (if any)Screening recommended & refer tointensive behavioural interventionsScreen for obesity. Patients with a body massindex (BMI) of 30 kg/m2 or higher should beoffered or referred to intensive, multi-componentbehavioral interventions.Risk AssessmentAssociated risk factors include:- Having obese parents- Poor nutrition- Insufficient physical activity- Lack of sleepBeing overweight is an independent risk factorfor cardiovascular diseaseScreening tool/test:Body mass index (BMI)Body mass index (BMI) and waist circumferenceScreening interval ortimingAnnualAnnualEvidence strengthIIVPage 20 of 36
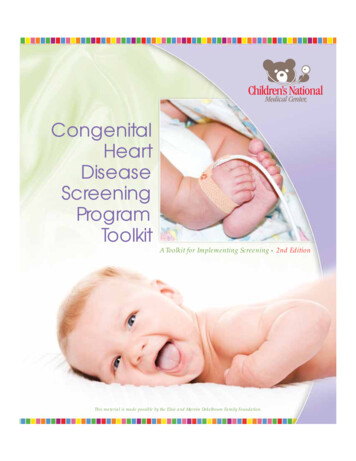
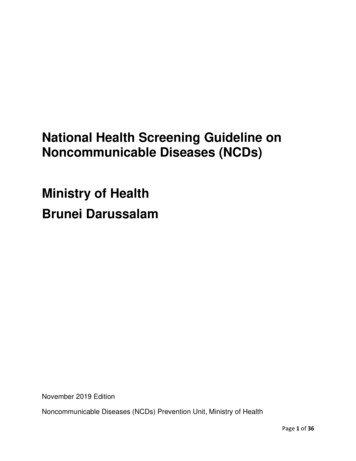
Vascular Conditions: Atherosclerotic Cardiovascular Disease (ASCVD)TargetpopulationRiskAssessmentAsymptomatic adult population 40 years and aboveConsider screening below 40 years old if presence of risk factor(s)Use 10-year global WHO/ISH CHD risk prediction score as per the following Figure 1 (Chart 1 and Chart 2)to assess CHD risk and follow guideline based risk-based preventive therapyRisk CategoryLow 10 %Screeninginterval ortiming5 years interval (or as per employment requirement)Intermediate (10 to 20 %)High/Very High 20 %Screening should be made on aScreening recommended after carefulScreeningcase-by-case basis after carefulNot recommendeddiscussion with the patient about the risksrecommendationdiscussion with the patient about theand benefits of screeningrisks and benefits of screeningIndividualized informed decision may be influenced by additional risk factors including: A family history of premature atherosclerotic cardiovascular disease (atherosclerotic cardiovascularAdditionaldisease event in first degree male relatives 50 years or female relatives 60 years), orfactors whichmay lead to Selected high-risk occupations, such as pilots, offshore workers etc orspecial If it would lead to more aggressive management of atherosclerotic cardiovascular disease-relatedconsiderationconditions (hypertension, diabetes, dyslipidemias, tobacco use) or Certain scenarios may necessitate more aggressive screeningCoronary Calcium: This may lead to reCoronary Calcium: This may lead toclassification of the patient into either there-classification of the patient intolow risk or high risk category, and/oreither the low risk or high riskcategory, and/orCT Angiography for selected individual,ScreeningIndividualized decisionand/ortool/test:Treadmill stress test: Decision toperform this test should be made onTreadmill stress test: Decision to performan individualized basis.this test should be made on anindividualized basis5 years interval or earlier as per clinicianassessmentPage 21 of 36
EvidenceStrengthI & IIFigure 1. WHO/ISH risk prediction chart for WPR A.10-year risk of a fatal or non-fatal cardiovascular event by gender, age, systolic blood pressure, total blood cholesterol, smokingstatus and presence or absence of diabetes mellitus.Chart 1Chart 2Page 22 of 36
OtherNoncommunicableDiseases (NCDs)Page 23 of 36
Abdominal Aortic AneurysmPopulationHigh Risk GroupsRecommendation &rationale (if any)Screening recommended for those with risk factorsRisk AssessmentPopulation at risk:1. Male sex2. History of smoking (defined as 100 cigarettes in a person’s lifetime)3. Age of 65 years or olderImportant risk factors for AAA include older age and a first-degree relative with an AAA; otherrisk factors include a history of other vascular aneurysms, coronary artery disease,cerebrovascular disease, atherosclerosis, hypercholesterolemia, obesity, and hypertension.Abdominal Ultrasonography - Sensitivity (94% to 100%), Specificity (98% to 100%)Screening tool/test:Screening interval orOne-off screening at age 65 and abovetimingEvidence strengthIPage 24 of 36
Anaemia (Iron Deficiency)PopulationRecommendation andrationale (if any)High Risk GroupsScreening recommended for high risk groups onlyGroups at risk:1. Women who are:– Pregnant– Non pregnant women of childbearing age– Having history of extensive menstruation / low iron intake / previous diagnosisof iron deficiency anaemiaRisk AssessmentScreening tool/test:Screening interval or timingEvidence strength2. Selected infants & children:– Preterm infants and low birth weight infants– Infants consuming non-iron-fortified formula for longer than 2 months– Infants introduced to cow’s milk before age 1 year, or children consuming morethan 24oz of cow’s milk daily.– Breast fed infants with inadequate iron in their diet after age 6 months– Young children aged 2 – 5 years at high risk of developing iron-deficiencyanaemia (for example low iron diet or special health care needs)Full blood count (FBC)IVPage 25 of 36
DementiaPopulationScreening for Cognitive Impairment in Older AdultsRecommendation andrationale (if any)Screening recommended for high risk groups only.Universal screening not recommended in view of lack of evidenceSome of the risk factors associated with cognitive impairment:Risk AssessmentScreening tool/test:Screening interval ortimingEvidence strength Increasing age Tobacco use Metabolic syndrome Depression Learning disabilities Alcohol abuseMini-Mental State ExaminationOther instruments with more limited evidence include the Clock Draw Test, Mini-Cog,Memory Impairment Screen, Abbreviated Mental Test, Short Portable Mental StatusQuestionnaire, Free and Cued Selective Reminding Test, 7-Minute Screen, TelephoneInterview for Cognitive Status, and Informant Questionnaire on Cognitive Decline in theElderly.IPage 26 of 36
Depression (Children & Adults)PopulationRecommendationand rationale (ifany)Risk AssessmentAdolescents (12-18 years)Screening is recommended. Screenwhen professional management andsupport are in place to assureaccurate diagnosis, effectivetreatment, and follow-upRisk factors for major depressivedisorder (MDD): parents with historyof depression, having co-morbidmental health or chronic medicalillness or previously experienced amajor negative live eventScreening intervalor timingEvidence strengthScreen high risk group and vulnerable group. Screenwhen professional management and support are in placeto assure accurate diagnosis, effective treatment, andfollow-upIncreased risk for depression include: history of chronicillnesses (eg. diabetes, renal disease, cancer, learningdisability, physical disability), post-natal women, beingelderly. For post-natal women: The Edinburgh Post NatalDepression Scale For people with chronic illnesses: Beck’s DepressionInventory, Hospital Depression Scale, Hamilton Anxiety and Depression scale can all be used For the elderly: Geriatric Depression ScaleThe interval for screening as per clinical judgement. In older adults, significant depressivesymptoms are associated with common life events, including medical illness, cognitive decline,bereavement, and institutional placement in residential or inpatient settings.II Screeningtool/test:Adults aged 18 years or olderPatient Health QuestionnaireModified for Adolescents (PHQ9-A)Beck’s Depression InventoryPrimary Care Version (BDI-PC)Page 27 of 36
Renal Impairment / Chronic Kidney DiseasePopulationHigh Risk GroupsRecommendation andrationale (if any)Risk AssessmentScreening recommended for high risk groups onlyScreening tool/test:High risk groups (Any one of the following risk factors):1) Any individual with diabetes mellitus2) Any individual with hypertension3) Any individual with acute kidney injury4) Any individual with cardiovascular disease5) Any individual with structural renal tract disease, recurrent renal calculi or prostatichypertrophy6) Any individual with a family history of end-stage renal disease (ESRD) or hereditary kidneydisease7) Any individual having multisystem diseases with potential kidney involvement – for example,systemic lupus erythematosus8) Any individual with a previous history of kidney injury or childhood kidney disease9) Individuals with opportunistic detection of haematuriaeGFR and urine albumin:creatinine ratio (ACR)Screening interval ortimingFrequency of monitoring tailored to the person according to: the underlying cause of CKD past patterns of eGFR and ACR (but be aware that CKD progression is often non-linear) comorbidities, especially heart failure changes to their treatment intercurrent illness whether they have chosen conservative management of CKDEvidence strengthIIPage 28 of 36
Appendix 1: Body Mass Index (BMI) ClassificationBMI CLASSIFICATIONUnderweight 18.5Normal range18.5 – 24.9Overweight 25.0 – 29.9Obese class I 30.0 – 34.9Obese class II 35.0 – 39.9Obese class III 40.0(Based on WHO International BMI Classification)Page 29 of 36
Acknowledgement1. Cardiology Unit, Raja Isteri Pengiran Anak Saleha (RIPAS) Hospital2. Community Maternal and Child Health, Ministry of Health3. Department of Internal Medicine, RIPAS Hospital4. Endocrinology Department, RIPAS Hospital5. Gastroenterology Department, RIPAS Hospital6. General Surgery Department, RIPAS Hospital7. Geriatrics and Palliative Unit, RIPAS Hospital8. Haematology Department, RIPAS Hospital9. Health Promotion Centre, Ministry of Health10. Jerudong Park Medical Centre (JPMC)11. Nephrology Department, RIPAS Hospital12. Noncommunicable Diseases (NCDs) Prevention Unit, Ministry of Health13. Obstetrics and Gynaecology Department, RIPAS Hospital14. Occupational Health Division, Environmental Health Services, Ministry of Health15. Otorhinolaryngology (ENT) Department, RIPAS Hospital16. Paediatrics Department, RIPAS Hospital17. Primary Healthcare, Department of Health Services, Ministry of Health18. Psychiatry Department, RIPAS Hospital19. Radiology Department, RIPAS Hospital20. Pantai Jerudong Specialist Centre (PJSC)Literature review on health screening policies and guidelines from: World Healt
Page 3 of 36 Background Information Health Screening "Screening is defined as the presumptive identification of unrecognized disease in an apparently healthy, asymptomatic population by means of tests, examinations or other procedures that can be applied rapidly and easily to the target population" (WHO) Criteria for an effective screening test as according to The Wilson & Jungner Classic