Transcription
ETHICON delivers value through a full lineof proven products, innovative technology,and responsive business services.
PREFACEThis manual has been prepared for the medical professional whowould like to learn more about the practice of surgery–thedynamics of tissue healing, the principles of wound closure, and thematerials available to today’s practitioners. Most important, ittouches on some of the critical decisions which must be made on adaily basis to help ensure proper wound closure.ETHICON PRODUCTS, a Johnson & Johnson company, is theworld’s leading marketer of surgical sutures and is the only U.S.company that offers an adhesive with microbial protection as analternative to sutures for topical skin closure.ETHICON enjoys a reputation for developing quality products toenhance the lives of patients and for providing outstanding serviceto customers. We hope you find this manual useful. But, above all,we hope that it reflects our high regard for the men and womenwho have chosen the medical profession as a career. ETHICON PRODUCTS
CONTRIBUTING EDITORDavid, L. Dunn, M.D., Ph. D.Jay Phillips Professor and Chairman of Surgery,University of MinnesotaWe thank Dr. Dunn for his contributions to the Wound ClosureManual. Dr. Dunn is currently the Jay Phillips Professor andChairman of Surgery at the University of Minnesota. Thisdepartment has a long-standing tradition and has attainednational and international recognition for excellence in trainingacademic general surgeons and surgical scientists. He is also theDivision Chief of General Surgery, Head of Surgical InfectiousDiseases, Director of Graduate Studies, and Residency ProgramDirector of the Department of Surgery.Dr. Dunn has published over 400 articles and book chapters in theareas of Surgical Infectious Diseases and Transplantation. He hasreceived regional and nationwide recognition in severalacademic organizations and is a Past-President of the SurgicalInfection Society, the Association for Academic Surgery, theMinnesota Chapter of the American College of Surgeons, theSociety of University Surgeons and the Society of UniversitySurgeons Foundation.
TABLE OF CONTENTS1WOUND HEALINGAND MANAGEMENTThe Wound. 2Recovery of Tensile Strength. 2Patient Factors that Affect Wound Healing. 2Surgical Principles. 4Classification of Wounds. 5Types of Wound Healing. 6Healing by Primary Intention. 6Healing by Second Intention. 7Delayed Primary Closure. 72THE SUTUREWhat is a Suture?. 10Personal Suture Preference. 10Suture Characteristics . 11Size and Tensile Strength. 11Monofilament vs. Multifilament . 11Absorbable vs. Nonabsorbable Sutures. 12Specific Suturing Materials. 13Synthetic Absorbable Sutures . 14Nonabsorbable Sutures . 16Synthetic Nonabsorbable Sutures. 17Common Suturing Techniques. 18Ligatures. 18The Primary Suture Line. 19Continuous Sutures. 19Interrupted Sutures. 22Deep Sutures. 22Buried Sutures . 22Purse-String Sutures. 22Subcuticular Sutures. 22The Secondary Suture Line. 23Stitch Placement. 23Knot Tying .Knot Security.Knot Tying Techniques Most Often Used .Square Knot .Surgeon’s or Friction Knot .Deep Tie .Ligation Using a Hemostatic Clamp .Instrument Tie .Endoscopic Knot Tying Techniques .Cutting the Secured Sutures .Suture Removal .Suture Handling Tips .Suture Selection Procedure .Surgery within the Abdominal Wall Cavity.Closing the Abdomen .Closing Contaminated or Infected Wounds.324242525262626262626262727283040THE SURGICAL NEEDLEElements of Needle Design .Principles of Choosing a Surgical Needle.Anatomy of a Needle .The Needle Eye .The Needle Body .Straight Needle .Half-Curved Needle .Curved Needle.Compound Curved Needle .The Needle Point .Types of Needles .Conventional Cutting Needles.Reverse Cutting Needles .Side Cutting Needles.Taper Point Needles .Taper Surgical Needles .Blunt Point Needles.Needleholders .Needleholder Use.Placing the Needle in Tissue .Needle Handling Tips .424344454646464647474748494950505151525253
4PACKAGINGAn Integral Part of the Product . 56RELAY* Suture Delivery System . . 56Modular Storage Racks. 56Dispenser Boxes. 57Primary Packets . 57E-PACK* Procedure Kit . 59Expiration Date. 60Suture Sterilization . 60Anticipating Suture Needs. 61Sterile Transfer of Suture Packets. 61Suture Preparation in the Sterile Field. 62Suture Handling Technique. 635TOPICAL SKIN ADHESIVESDERMABOND* Topical Skin Adhesive. 686OTHER SURGICALPRODUCTSAdhesive Tapes. 74Indications and Usage. 74Application . 74After Care and Removal . 74Skin Closure Tapes . 75Polyester Fiber Strip. 75Umbilical Tape . 75Surgical Staples . 75Indications and Usage . 76Aftercare and Removal . 76PROXIMATE* Skin Staplers. 76Looped Suture . 77Retention Suture Devices . 777PRODUCT TERMSAND TRADEMARKS8PRODUCT INFORMATION9INDEX
CHAPTER 1WOUND HEALINGAND MANAGEMENT
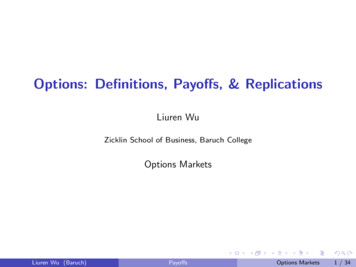
2WOUND HEALING & MANAGEMENTTHE WOUNDInjury to any of the tissues ofthe body, especially that causedby physical means and withinterruption of continuity is definedas a wound.1 Though most oftenthe result of a physical cause, aburn is also considered a wound.Both follow the same processestowards the restoration tohealth – otherwise knownas healing.1Wound healing is a natural andspontaneous phenomenon. Whentissue has been disrupted so severelythat it cannot heal naturally(without complications or possibledisfiguration) dead tissue andforeign bodies must be removed,infection treated, and the tissuemust be held in apposition until thehealing process provides the woundwith sufficient strength to withstandstress without mechanical support.A wound may be approximatedwith sutures, staples, clips, skinclosure strips, or topical adhesives.Tissue is defined as a collection ofsimilar cells and the intercellularsubstances surrounding them.There are four basic tissues in thebody: 1) epithelium; 2) connectivetissues, including blood, bone andcartilage; 3) muscle tissue; and4) nerve tissue. The choice ofwound closure materials and thetechniques of using them are primefactors in the restoration ofcontinuity and tensile strength tothe injured tissues during thehealing process.The parameters for measuring thestrength of normal body tissue are: Tensile Strength—The load percross-sectional area unit at thepoint of rupture, relating to thenature of the material rather thanits thickness. Breaking Strength—The loadrequired to break a wound regardless of its dimension, the moreclinically significant measurement. Burst Strength—The amount ofpressure needed to rupture aviscus, or large interior organ.The rate at which wounds regainstrength during the wound healingprocess must be understood as abasis for selecting the mostappropriate wound closure material.RECOVERY OFTENSILE STRENGTHTensile strength affects the tissue'sability to withstand injury but isnot related to the length of time ittakes the tissue to heal. As collagenaccumulates during the reparativephase, strength increases rapidly butit is many months before a plateauis reached.2 Until this time, thewound requires extrinsic supportfrom the method used to bring ittogether – usually sutures. Whileskin and fascia (the layer of firmconnective tissue covering muscle)are the strongest tissues in the body,they regain tensile strength slowlyduring the healing process. Thestomach and small intestine, on theother hand, are composed of muchweaker tissue but heal rapidly.Variations in tissue strength mayalso be found within the sameorgan. Within the colon, forexample, the sigmoid region isapproximately twice as strong as thececum—but both sections heal atthe same rate. Factors that affecttissue strength include the size, age,and weight of the patient, thethickness of tissue, the presence ofedema, and duration (the degree towhich the tissue has hardened inresponse to pressure or injury).PATIENT FACTORS THATAFFECT WOUND HEALINGThe goal of wound managementis to provide interventions thatefficiently progress wounds throughthe biologic sequence of repair orregeneration. The patient's overallhealth status will affect the speed ofthe healing process. The followingare factors that should be consideredby the surgical team prior to andduring the procedure. 2,3,4 AGE — With aging, both skinand muscle tissue lose their toneand elasticity. Metabolism alsoslows, and circulation may beimpaired. But aging alone is nota major factor in chronic woundhealing. Aging and chronicdisease states often go together,and both delay repair processesdue to delayed cellular responseto the stimulus of injury, delayedcollagen deposition, anddecreased tensile strength in theremodeled tissue. All of thesefactors lengthen healing time. WEIGHT — Obese patientsof any age have, excess fat at thewound site that may preventsecuring a good closure. Inaddition, fat does not have a richblood supply, making it the mostvulnerable of all tissues to traumaand infection. NUTRITIONAL STATUS —Overall malnutrition associatedwith chronic disease or cancer,or specific deficiencies in
CHAPTER t s(Weak)Bladder(Weak)carbohydrates, proteins, zinc, andvitamins A, B, and C can impairthe healing process. Adequatenutrition is essential to supportcellular activity and collagensynthesis at the wound site. DEHYDRATION — If thepatient's system has beendepleted of fluids, the resultingelectrolyte imbalance can affectcardiac function, kidneyfunction, cellular metabolism,oxygenation of the blood, andhormonal function. These effectswill not only impact upon thepatient's overall health status andrecovery from surgery but mayalso impair the healing process. INADEQUATE BLOODSUPPLY TO THE WOUNDSITE — Oxygen is necessary forcell survival and, therefore,healing. Skin healing takes placemost rapidly in the face andneck, which receive the greatestblood supply, and most slowly inthe extremities. The presence ofany condition that compromisesthe supply of blood to thewound, such as poor circulationto the limbs in a diabetic patientor arteriosclerosis with vascularcompromise, will slow and caneven arrest the healing process. IMMUNE RESPONSES —Because the immune responseprotects the patient frominfection, immunodeficienciesmay seriously compromise theoutcome of a surgical procedure.Patients infected with HIV, aswell as those who have recentlyundergone chemotherapy or whohave taken prolonged highdosages of catabolic steroids, may3have debilitated immune systems.Some patients have allergies tospecific suturing materials, metalalloys, or latex. These, on theother hand, will cause a heightened immune response in theform of an allergic reaction.This may also interfere with thehealing process. Therefore,the surgeon should alwayscheck beforehand on apatient's allergies. CHRONIC DISEASE —A patient whose system hasalready been stressed by chronicillness, especially endocrinedisorders, diabetes, malignancies,localized infection, or debilitatinginjuries will heal more slowly andwill be more vulnerable to postsurgical wound complications.All of these conditions meritconcern, and the surgeon mustconsider their effects upon thetissues at the wound site, as wellas their potential impact uponthe patient's overall recoveryfrom the procedure.Malignancies, in addition, mayalter the cellular structure oftissue and influence thesurgeon's choice of methods andclosure materials. RADIATION THERAPY —Radiation therapy to the surgicalsite prior to or shortly aftersurgery can produce considerableimpairment of healing and leadto substantial wound complications. Surgical procedures formalignancies must be plannedto minimize the potential forthese problems.* Trademark
4WOUND HEALINGSURGICAL PRINCIPLESMany factors that affect the healingprocess can be controlled by thesurgical team in the operating room,by the obstetrical team in labor anddelivery, or by the emergency teamin the trauma center. Their firstpriority is to maintain a sterileand aseptic technique to preventinfection. Organisms foundwithin a patient's own body mostcommonly cause postoperativeinfection, but microorganismscarried by medical personnel alsopose a threat. Whatever the source,the presence of infection will deterhealing. In addition to concernsabout sterility, the following mustbe taken into consideration whenplanning and carrying out anoperative procedure.3 THE LENGTH ANDDIRECTION OF THEINCISION — A properlyplanned incision is sufficientlylong to afford sufficient optimumexposure. When deciding uponthe direction of the incision, thesurgeon must bear the followingin mind: The direction in which woundsnaturally heal is from side-toside, not end-to-end. The arrangement of tissue fibersin the area to be dissected willvary with tissue type. The best cosmetic results may beachieved when incisions are madeparallel to the direction of thetissue fibers. Results may varydepending upon the tissuelayer involved. DISSECTIONTECHNIQUE — When incisingtissue, a clean incision shouldbe made through the skin withone stroke of evenly appliedpressure on the scalpel. Sharpdissection should be used to cutthrough remaining tissues. Thesurgeon must preserve theintegrity of as many of theunderlying nerves, blood vessels,and muscles as possible. TISSUE HANDLING —Keeping tissue trauma to aminimum promotes fasterhealing. Throughout theoperative procedure, the surgeonmust handle all tissues verygently and as little as possible.Retractors should be placed withcare to avoid excessive pressure,since tension can cause seriouscomplications: impaired bloodand lymph flow, altering of thelocal physiological state of thewound, and predisposition tomicrobial colonization. HEMOSTASIS — Variousmechanical, thermal, andchemical methods are available todecrease the flow of blood andfluid into the wound site.Hemostasis allows the surgeon towork in as clear a field as possiblewith greater accuracy. Withoutadequate control, bleeding fromtransected or penetrated vesselsor diffused oozing on largedenuded surfaces may interferewith the surgeon's view ofunderlying structures.Achieving complete hemostasisbefore wound closure also willprevent formation of postopera-tive hematomas. Collections ofblood (hematomas) or fluid(seromas) in the incision canprevent the direct apposition oftissue needed for complete unionof wound edges. Furthermore,these collections provide an idealculture medium for microbialgrowth and can lead to seriousinfection.When clamping or ligating avessel or tissue, care must betaken to avoid excessive tissuedamage. Mass ligation thatinvolves large areas of tissue mayproduce necrosis, or tissue death,and prolong healing time. MAINTAINING MOISTUREIN TISSUES — During longprocedures, the surgeon mayperiodically irrigate the woundwith warm physiologic (normal)saline solution, or cover exposedsurfaces with saline-moistenedsponges or laparotomy tapes toprevent tissues from drying out. REMOVAL OF NECROTICTISSUE AND FOREIGNMATERIALS — Adequatedebridement of all devitalizedtissue and removal of inflictedforeign materials are essentialto healing, especially in traumaticwounds. The presence offragments of dirt, metal, glass,etc., increases the probabilityof infection. CHOICE OF CLOSUREMATERIALS — The surgeonmust evaluate each case individually, and choose closure materialwhich will maximize theopportunity for healing andminimize the likelihood of
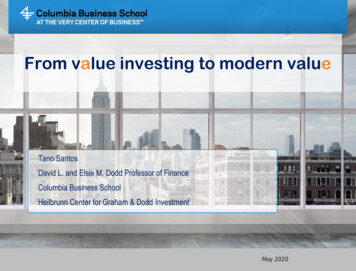
CHAPTER 1infection. The proper closurematerial will allow the surgeonto approximate tissue with aslittle trauma as possible, and withenough precision to eliminatedead space. The surgeon'spersonal preference will play alarge role in the choice of closurematerial; but the location of thewound, the arrangement of tissuefibers, and patient factors influence his or her decision as well. CELLULAR RESPONSE TOCLOSURE MATERIALS —Whenever foreign materials suchas sutures are implanted in tissue,the tissue reacts. This reactionwill range from minimal tomoderate, depending upon thetype of material implanted. Thereaction will be more marked ifcomplicated by infection, allergy,or trauma.Initially, the tissue will deflect thepassage of the surgeon's needleand suture. Once the sutureshave been implanted, edema ofthe skin and subcutaneous tissueswill ensue. This can causesignificant patient discomfortduring recovery, as well asscarring secondary to ischemicnecrosis. The surgeon must takethese factors into considerationwhen placing tension upon theclosure material.the fatty layer which tends tolack blood supply. Serum orblood may collect, providing anideal medium for the growthof microorganisms that causeinfection. The surgeon mayelect to insert a drain or applya pressure dressing to helpeliminate dead space in thewound postoperatively. CLOSING TENSION —While enough tension must beapplied to approximate tissue andeliminate dead space, the suturesmust be loose enough to preventexaggerated patient discomfort,ischemia, and tissue necrosisduring healing. POSTOPERATIVEDISTRACTION FORCES —The patient's postoperativeactivity can place undue stressupon a healing incision.Abdominal fascia will be placedunder excessive tension aftersurgery if the patient strains tocough, vomit, void, or defecate.5Tendons and the extremities mayalso be subjected to excessivetension during healing. Thesurgeon must be certain thatthe approximated wound isadequately immobilized toprevent suture disruptionfor a sufficient period of timeafter surgery. IMMOBILIZATION —Adequate immobilization of theapproximated wound, but notnecessarily of the entire anatomicpart, is mandatory after surgeryfor efficient healing and minimalscar formation.CLASSIFICATIONOF WOUNDSThe Centers for Disease Controland Prevention (CDC), using anadaptation of the American Collegeof Surgeons’ wound classificationschema, divides surgical woundsinto four classes: clean wounds,clean-contaminated wounds,FIGURE2DEAD SPACEIN A WOUND ELIMINATION OF DEADSPACE IN THE WOUND —Dead space in a wound resultsfrom separation of portions ofthe wound beneath the skinedges which have not beenclosely approximated, or from airor fluid trapped between layers oftissue. This is especially true in* Trademark
6WOUND HEALINGcontaminated wounds and dirty orinfected wounds.5 A discussion ofeach follows.contaminated by entry into aviscus resulting in minimal spillageof contents.Seventy-five percent of all wounds(which are usually elective surgicalincisions) fall into the clean woundscategory—an uninfected operativewound in which no inflammationis encountered and the respiratory,alimentary, genital, or uninfectedurinary tracts are not entered.These elective incisions are madeunder aseptic conditions and arenot predisposed to infection.Inflammation is a natural part ofthe healing process and should bedifferentiated from infection inwhich bacteria are present andproduce damage.Contaminated wounds includeopen, traumatic wounds or injuriessuch as soft tissue lacerations, openfractures, and penetrating wounds;operative procedures in which grossspillage from the gastrointestinaltract occurs; genitourinary or biliarytract procedures in the presenceof infected urine or bile; andoperations in which a major breakin aseptic technique has occurred(as in emergency open cardiacmassage). Microorganismsmultiply so rapidly that within6 hours a contaminated woundcan become infected.Clean wounds are closed by primaryunion and usually are not drained.Primary union is the most desirablemethod of closure, involving thesimplest surgical procedures andthe lowest risk of postoperativecomplications. Apposition of tissueis maintained until wound tensilestrength is sufficient so that suturesor other forms of tissue appositionare no longer needed.Dirty and infected wounds havebeen heavily contaminated orclinically infected prior to theoperation. They include perforatedviscera, abscesses, or neglectedtraumatic wounds in whichdevitalized tissue or foreign materialhave been retained. Infectionpresent at the time of surgery canincrease the infection rate of anywound by an average of four times.Clean-contaminated wounds areoperative wounds in which therespiratory, alimentary, genital, orurinary tracts are entered undercontrolled conditions and withoutunusual contamination. Specifically,operations involving the biliarytract, appendix, vagina, andoropharynx are included in thiscategory provided no evidenceof infection or major break intechnique is encountered.Appendectomies, cholecystectomies,and hysterectomies fall into thiscategory, as well as normallyclean wounds which becomeTYPES OFWOUND HEALINGThe rate and pattern of healing fallsinto three categories, dependingupon the type of tissue involvedand the circumstances surroundingclosure. Timeframes are generalizedfor well-perfused healthy softtissues, but may vary.HEALING BYPRIMARY INTENTIONEvery surgeon who closes a woundwould like it to heal by primaryunion or first intention, withminimal edema and no localinfection or serious discharge. Anincision that heals by primaryintention does so in a minimum oftime, with no separation of thewound edges, and with minimalscar formation. This takes place inthree distinct phases:2,3Inflammatory (preparative) –During the first few days, aninflammatory response causes anoutpouring of tissue fluids, anaccumulation of cells andfibroblasts, and an increased bloodsupply to the wound. Leukocytesand other cells produce proteolyticenzymes which dissolve and removedamaged tissue debris. These arethe responses which prepare the siteof injury for repair. The processlasts 3 to 7 days. Any factor whichinterferes with the progress, mayinterrupt or delay healing. Duringthe acute inflammatory phase, thetissue does not gain appreciabletensile strength, but depends solelyupon the closure material to hold itin approximation.Proliferative – After thedebridement process is well along,fibroblasts begin to form a collagenmatrix in the wound known asgranulation tissue. Collagen, aprotein substance, is the chiefconstituent of connective tissue.Collagen fiber formation determinesthe tensile strength and pliability ofthe healing wound. As it fills withnew blood vessels, the granulationbecomes bright, beefy, red tissue.The thick capillary bed which fills
CHAPTER 1DamagedtissuedebrisTissue fluids7FIGURE3PHASES n fibersIncreased blood supplyPHASE 1 –Inflammatory response anddebridement processPHASE 2 –Collagen formation(scar tissue)the matrix, supplies the nutrientsand oxygen necessary for the woundto heal. This phase occurs fromday 3 onward.In time, sufficient collagen is laiddown across the wound so that itcan withstand normal stress. Thelength of this phase varies with thetype of tissue involved and thestresses or tension placed upon thewound during this period.Wound contraction also occurs during this phase. Wound contractionis a process that pulls the woundedges together for the purpose ofclosing the wound. In essence, itreduces the open area, and ifsuccessful, will result in a smallerwound with less need for repair byscar formation. Wound contractioncan be very beneficial in the closureof wounds in areas such as the buttocks or trochanter but can be veryharmful in areas such as the handor around the neck and face, whereit can cause disfigurement andexcessive scarring.3Surgical wounds that are closedby primary intention have minimalcontraction response. Skin graftingis used to reduce avoided contraction in undesirable locations.PHASE 3 –Sufficient collagen laid downRemodelling – As collagen deposition is completed, the vascularity ofthe wound gradually decreases andany surface scar becomes paler. Theamount of collagen that is finallyformed – the ultimate scar – isdependent upon the initial volumeof granulation tissue.2HEALING BYSECOND INTENTIONWhen the wound fails to heal byprimary union, a more complicatedand prolonged healing process takesplace. Healing by second intentionis caused by infection, excessivetrauma, tissue loss, or impreciseapproximation of tissue.3In this case, the wound may be leftopen and allowed to heal from theinner layer to the outer surface.Granulation tissue forms andcontains myofibroblasts. Thesespecialized cells help to close thewound by contraction. Thisprocess is much slower than primaryintention healing. Excessivegranulation tissue may build upand require treatment if it protrudesabove the surface of the wound,preventing epithelialization.DELAYED PRIMARYCLOSUREThis is considered by manysurgeons to be a safe method ofmanagement of contaminated, aswell as dirty and infected traumaticwounds with extensive tissue lossand a high risk of infection. Thismethod has been used extensively inthe military arena and has provensuccessful following excessivetrauma related to motor vehicleaccidents, shooting incidents, orinfliction of deep, penetratingknife wounds.3The surgeon usually treats theseinjuries by debridement ofnonviable tissues and leaves thewound open, inserting gauzepacking which is changed twice aday. Patients sedation or a return tothe operating room with generalanesthesia generally is only requiredin the case of large, complexwounds. Wound approximationusing adhesive strips, previouslyplaced but untied sutures, staplesafter achieving local anesthesia canoccur within 3-5 days if the wounddemonstrates no evidence ofinfection and the appearance of redgranulation tissue. Should this not* Trademark
8WOUND HEALINGoccur, the wound is allowed toheal by secondary intention. Whenclosure is undertaken, skin edgesand underlying tissue must be accurately and securely approximated.IN THENEXT SECTIONThe materials, devices, andtechniques used to repair woundedtissue will be discussed at length.As you will see, the number ofoptions available is extensive. Butno matter how many choices thesurgeon has, his or her objectiveremains singular: to restore thepatient to health with as littleoperative trauma as possible andan excellent cosmetic result.REFERENCES1. Stedman’s Medical Dictionary,27th edition, 20002. Henry, Michael and Thompson,Jeremy: Clinical Surgery, W.B.Saunders, 20013. Skerris, David A.: Mayo ClinicBasic Surgery Skills, Mayo ClinicScientific Press, 19994. Sussman, Carrie: Wound Care,Aspen Publishers, 19985. NNIS Manual, CDC,MHA, 2000
CHAPTER 2THE SUTURE
10THE SUTUREWHAT ISA SUTURE?The word "suture" describes anystrand of material used to ligate (tie)blood vessels or approximate (bringclose together) tissues. Sutures areused to close wounds. Sutures andligatures were used by both theEgyptians and Syrians as far back as2,000 B.C. Through the centuries, awide variety of materials—silk,linen, cotton, horsehair, animaltendons and intestines, and wiremade of precious metals—have beenused in operative procedures. Someof these are still in use today.The evolution of suturing materialhas brought us to a point of refinement that includes sutures designedfor specific surgical procedures.Despite the sophistication oftoday's suture materials and surgicaltechniques, closing a wound stillinvolves the same basic procedureused by physicia
AFFECT WOUND HEALING The goal of wound management is to provide interventions that efficiently progress wounds through the biologic sequence of repair or regeneration. The patient's overall health status will affect the speed of the healing process. The following are factors that should be considered by the surgical team prior to and during the .