Transcription
April 2020The Neurobiologyof ADHD
Table of Contents33457101213Introduction and epidemiologyDiagnosis and consequences of ADHDGenetics and epigenetics of ADHDStructural brain changesBrain networks and functional brain changesAltered neurotransmission in ADHDConcluding remarksReferencesDEFINITION OF TERMSBrain networks – Discrete areas of the brain thatwork together to perform complex tasksCatecholamines – Monoamine neurotransmitters(dopamine, norepinephrine, and serotonin)Coherence – When brain regions have similarneuronal oscillatory activity with each otherCopy number variants – Variations in the numberof genes or sections of DNA from one individual tothe nextEpigenetics – Mechanisms for regulating geneexpression that involve postgenomic alterations inDNA and chromatin structure rather than variationsin genetic sequenceEtiopathogenesis – Classification of a disease/disorder that is based on its cause/developmentExecutive function – Higher-level cognitiveprocessing, including planning, goal-directedbehavior, and cognitive flexibilityRadioligand – A substance used in research thatbinds to a targeted receptor for the purpose ofsensitive and quantitative detection“Top-down” regulation of emotion – Emotionalregulation that is in response to a cognitiveappraisal of an event (in comparison to “bottom‑up”regulation, which is based on how the event isemotionally perceived)Bolded terms above correspond to bolded termsin monograph.The Neurobiology of ADHD — April 20202
INTRODUCTION AND EPIDEMIOLOGYAttention deficit/hyperactivity disorder (ADHD)is the most prevalent neurodevelopmentaldisorder.1,2 The prevalence of ADHD in children andadolescents in the United States and around theworld is approximately 9% to 11%, with roughly 4%to 5% continuing to have ADHD as adults.3-6 ADHDis a childhood-onset developmental disorder withcore symptoms of inattentiveness, impulsivity,and/or motor unrest (ie, hyperactivity) that occurto a degree beyond what would be expectedbased on the child’s age, developmental level, andintellectual level.7 Furthermore, varying degreesof emotional dysregulation, irritability, deficitsin executive function, behavioral disturbancesrelated to impulse control (eg, oppositional defiant,conduct disorders), learning disabilities, and motordisturbances (eg, tics), as well as other psychiatricconditions (eg, anxiety, depression), frequentlyaccompany an ADHD diagnosis.8,9This monograph reviews the neurobiological basisof ADHD, including genetics, brain networks,structural and functional brain changes, and alteredneurotransmission.DIAGNOSIS AND CONSEQUENCES OF ADHDClinical definitions of ADHD have progressedfrom George Still’s “defect in moral control” in1903 to “hyperkinesis” in the 1930s, to “minimalbrain dysfunction” and “hyperactive childsyndrome” in the 1950s.8 In 1980, the Diagnosticand Statistical Manual of Mental Disorders, ThirdEdition (DSM‑III) has a diagnosis of attentiondeficit disorder, with or without hyperactivity, andDSM-IV and DSM‑5 include 3 ADHD subtypes:predominantly inattentive, predominantlyhyperactive/impulsive, and combined.8,10,11ADHD usually does not occur as a singlepsychopathology; approximately 75% of patientswith ADHD have at least 1 comorbid psychiatriccondition (eg, depression, anxiety, substanceabuse), which can mask underlying ADHD, makeThe Neurobiology of ADHD — April 2020differential diagnosis more challenging, andpredict a worse prognosis.7,12 In a longitudinalanalysis of a large birth cohort followed throughage 18 to 19 years, individuals with ADHD hadsignificantly higher rates of comorbid depression,bipolar disorder, and anxiety disorders comparedto individuals without ADHD.13 By adulthood,up to 50% of individuals with ADHD havedeveloped depression, with up to 35% sufferingfrom anxiety.14 Is this a consequence of ongoingdistress due to suboptimal ADHD treatment or aconsequence of ongoing changes in the neuralcircuitry of ADHD which is shared with mood andanxiety disorders?15 Further research is neededbefore this question can be answered.The importance of effective, evidence-basedADHD treatment should not be underestimated,especially as the impact of the disorder canbe pervasive and lifelong.16 Consequences ofADHD include increased risk of school failureand injuries in children and adolescents, andcar accidents (fatal and nonfatal), substanceuse/abuse/dependence, unplanned pregnancy,sexually transmitted diseases, criminalbehavior, employment/financial issues, andrelationship problems/divorce in adolescentsand adults. 3,13,17-23 ADHD also imparts a highermortality rate. Studies show up to a 3-timesgreater risk of premature death and up to a4-times greater risk of death from all causes inindividuals with ADHD compared to individualswithout ADHD, often due to accidents andtrauma, comorbid psychiatric disorders, andsuicide. 24-27 Importantly, pharmacotherapy hasbeen found to significantly reduce the risk ofmany of these consequences, including repeatinga grade, motor vehicle accidents, trauma leadingto emergency room visits, and criminality, aswell as improve quality of life and social/familyfunctioning. 28-34 ADHD treatment has alsodemonstrated a reduced risk of developingcommon psychiatric comorbid conditions, as wellas reducing their risk of recurrence. 34-373
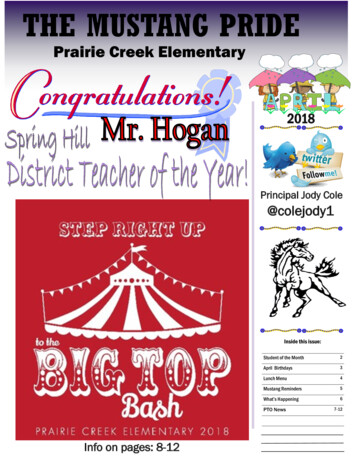
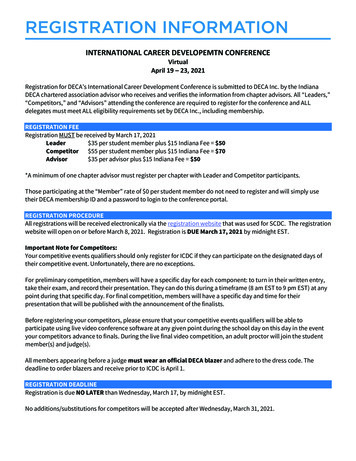
GENETICS AND EPIGENETICS OF ADHDADHD is one of the most heritable psychiatricdisorders, with heritability estimates rangingfrom 75% to 90%.38,39 Although identical twinstudies have demonstrated consistently highconcordance rates (68%-81%), first-degree relativeshave only a modest risk of manifesting ADHD(approximately 20%), consistent with a complexpolygenetic pattern of inheritance.39 There areseveral sources of relevant information regardinggenetic contribution to ADHD, including genomewide association studies (GWAS), research focusingon rare but very influential copy number variants(CNVs), studies examining associations betweencandidate genes and ADHD, and work examininginteractions between genes and environment.Some GWAS research has yielded surprisingfindings related to ADHD and its shared geneticswith other psychiatric disorders, with majordepressive disorder the closest genetic “relative”to ADHD.40 A recent, very large-scale GWAS ofapproximately 20,000 individuals with ADHDand approximately 35,000 controls found that agenetic makeup that carries a risk of ADHD is alsoassociated with increased risk of mood disorders,including depression, mood swings, anxietydisorders, bipolar disorder, irritability, and addictivebehaviors, including alcohol use/dependency(Figure 1).41 It is anticipated that additional researchwill clarify whether tendencies toward higher risk forthese disorders/behaviors are true comorbidities ofADHD or are manifestations of the ADHD geneticunderpinning itself. Other candidate genes thathave been implicated in ADHD etiopathogenesisinclude those involved in the neurotransmissionof dopamine (DA), norepinephrine (NE),serotonin (5‑HT), and glutamate (Glu).42,43Rare ( 1% frequency), subtle chromosomalmutations, deletions, and duplications (CNVs) mayplay a substantial role in contributing to ADHDrisk.9,43,44 In fact, one study found that approximatelytwice as many individuals with ADHD than withoutcarried large CNVs (15.6% vs 7.5%).45 CNVsassociated with ADHD include genes involved incalcium signaling, glutamatergic transmission, andregulation of sleep-wake behavior and vigilance.46-48Numerous environmental risk factors whichinteract with genetic and epigenetic vulnerabilitiesplay a significant role in the etiology of ADHD.Figure 1. Polygenic risk for ADHD and associated traits. 41BMIGeneral cognitive ability4.5 10 368.1 10 29Risk taking9.3 10 25Neuroticism-log10 modelP -value402.2 10 24Tobacco use4.2 10 21Depression202.2 10 13Alcohol dependency104.5 10 6Anxiety disorder302.9 10 4Bipolar disorder0.0070.0020.004Variance Explained: R 26.7 10 44Fed-up feelings6.9 10 42Loneliness/Isolation4.5 10 34Miserableness5.4 10 29Irritability3 10Tense/High strung-log10 modelP -value403.4 10 12Sensitivity/Hurt feelingsSuffer from nerves 183.5 10 13Guilty feelings6 10 120.002Worry after embarrassment0.009Nervous feeling0.042Worrier/Anxious feelings0.1620.000Phenotype (best fit)Phenotype (best fit)Alcohol intakeSchizophreniaMood swings4.5 10 1293020100.2670.0000 0.0005 0.0010 0.0015 0.0020 0.0025Variance Explained: R 2ADHD, attention deficit/hyperactivity disorder; BMI, body mass index.The Neurobiology of ADHD — April 20204
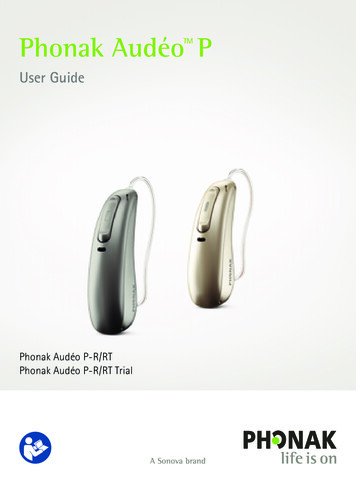
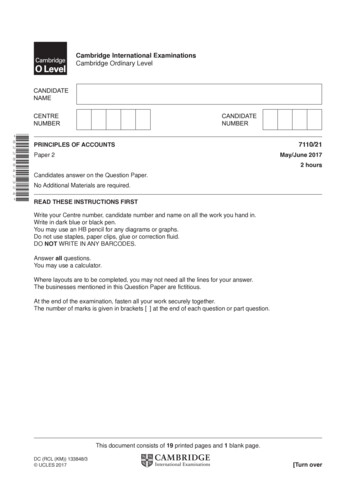
These include poor maternal nutrition, maternalanemia, parental psychopathology and lowersocioeconomic status, complicated and stressfulpregnancy/birth, prematurity, low birth weightand small head circumference, and prenatalexposure to drugs (eg, tobacco, cocaine, alcohol,antidepressants) and toxins (eg, lead).2,49-51Furthermore, a number of childhood adversities,such as viral infections (including meningitis/encephalitis), cerebral trauma, epilepsy, anemia,and disorders of the endocrine, immune, andmetabolic systems, have all been implicated as riskfactors for ADHD.49In summary, genetic research indicates thatADHD is not due to a single gene.39 Rather,it appears that a large number of genes withminor effects, CNVs, and interactions betweengenes and environmental risks/adversitiesall play a relevant role in the pathogenesis ofADHD.39,44,49 These studies also offer insight intothe association of ADHD and mood dysregulation,anxiety, and substance use, which leads to thequestion whether these are traits inherent inthe expression of ADHD or symptoms of trulycomorbid disorders. Future genetic studiesmay clarify the role of developmental phases ingene-environment interactions, provide a betterunderstanding of the link between genetics andspecific neurobiological underpinnings of ADHDsubtypes, and provide guidance for the mosteffective treatment choices.key takeaway: The pathogenesis ofADHD is complex, involving an interplay ofgenes and environment.STRUCTURAL BRAIN CHANGESDysfunctional brain areas frequently implicated inthe pathophysiology of ADHD are the prefrontalcortex (PFC, including the dorsolateral prefrontalcortex [DLPFC] and the ventrolateral prefrontalcortex [VLPFC]), anterior cingulate cortex(ACC), parietal cortex, striatum, and cerebellum(Figure 2; Table 1).52,53Structural imaging studies have found reducedgray matter volume in most of the brain structuresimplicated in the pathogenesis of ADHD.2,54,55Reduced striatal volume is one of the mostreplicated findings in the brains of individuals withADHD.55,56 Imaging studies have also noted reducedvolume of the PFC (including the DLPFC) and theACC (Figure 3), corpus callosum, and cerebellum,as well as the globus pallidus, caudate nucleus,and thalamus (Figure 4).57-59 Relevance of structuralchanges in the pathophysiology of ADHD isTable 1. Brain Structures Implicated in ADHD and Their Functions15,52,60-62StructureFunctionPrefrontal cortexAttention, planning, working memory (DLPFC); behavioral inhibition (VLPC); complexdecision making, strategic planning (VMPC)ACCMovement (caudal regions); attention, cognition (anterior regions); emotion, motivation(rostral and ventral regions); affective and cognitive components of executive control(dorsal regions)CerebellumMotor control; cognitive and affective processesParietal cortexOrientation of attentionBasal ganglia (includes the striatum[caudate nucleus, putamen] andglobus pallidus)Motivation, reward processing, goal-directed behavior, motor controlACC, anterior cingulate cortex; ADHD, attention deficit/hyperactivity disorder; DLPFC, dorsolateral prefrontal cortex; VLPC, ventrolateral prefrontalcortex; VMPC, ventromedial prefrontal cortex.The Neurobiology of ADHD — April 20205
supported by studies that have noted a relationshipbetween frontal, temporal, caudate, andcerebellar volumes and ADHD symptom severity.63Furthermore, reduced thalamic and ventrostriatalvolumes have been found to significantly correlatewith measures of impulsivity, hyperactivity, andinattention in individuals with ADHD compared toindividuals without ADHD.64,65 Total brain volume isalso reduced, with studies reporting volumes 3% to5% smaller in individuals with ADHD compared toindividuals without ADHD.62,63Figure 2. Brain structures implicated in ADHD (adaptedfrom Faraone 2015). 52Prefrontal cortexLateral viewDorsolateralprefrontal entromedialprefrontal cortexCerebellumMedial viewAnterior cingulatecortexPutamenVentral anteriorcingulate cortexGlobuspallidusADHD, attention deficit/hyperactivity disorder.Figure 3. Reduced volume (in blue) in the dorsolateralprefrontal cortex and anterior cingulate gyrus (adaptedfrom Seidman 2006). 58CGa, anterior cingulate gyrus; DLPFC, dorsolateral prefrontal cortex.Figure 4. Reduced volume (green) in the globus pallidus,caudate, and thalamus. 57The Neurobiology of ADHD — April 2020Basal gangliaDoral anteriorcingulate cortexStriatumCaudatenucleusIn addition to decreased brain volume, delayedcortical development is also seen in children withADHD compared to children without.66 A landmarkstudy conducted in 2007 found that peak corticalthickness was achieved, on average, 3 years later inchildren with ADHD relative to controls.66 The delaywas longest in the PFC (approximately 5 years inthe middle PFC), an area important for executivefunctioning, reward, memory, suppression ofinappropriate responses, and motor control.66Extending these findings, a group of authorsreported “normalization” of caudate volume overthe course of extended maturation.63 Sophisticateddiffusion tensor imaging studies have discovereddelayed/reduced myelination of prefrontal-striataltracts, cortico-cortical connections, thalamocortical white matter tracts, and connectionswithin the default mode network (DMN; includingprefrontal, cingulate, and parietal corticesand temporal lobes) in individuals with ADHDcompared with controls.67-69 These differences maybe responsible for the delayed development ofcognitive-executive control observed in ADHD.67-69Cortical thinning, like cortical thickening, is anormal brain process.70 However, enhancedcortical thinning in children and adolescents withADHD vs controls has been found, with significantdifferences noted in areas important for attentionaland motor output (eg, prefrontal regions).71 Corticalthinning has also been reported in longitudinalstructural studies of adults with ADHD, with6
the rate of cortical thinning correlating with thenumber of ADHD symptoms.72,73 Furthermore,convergence toward normal brain dimensions wasonly observed in young adults whose symptomsremitted compared with individuals who remainedsymptomatic.73key takeaway: Individuals with ADHDexhibit reductions in gray mattervolume, delayed cortical maturation,and enhanced cortical thinning, whichhave been shown to be related to ADHDsymptomatology.BRAIN NETWORKS AND FUNCTIONALBRAIN CHANGESBrain networks involved in attention and, therefore,especially relevant to ADHD, include the cognitiveexecutive network, the cortico-striatal-thalamiccortical network, and the cortico-limbic network(Figure 5; Table 2).The cognitive-executive network (Figure 5A) iscomposed of interconnected cortical areas thathave a role in executive function and workingmemory and in selective and sustained attention.74,75Dorsal prefrontal cortical areas participate in“top-down” regulation of emotion.75-77 In addition,prefrontal cortical areas are connected to premotorcortices, where they participate in the planningof motoric activity, with abnormalities in theseconnections found in individuals with ADHD.15 Thecortico-striatal-thalamic-cortical network (Figure 5B)comprises parallel loops that connect the PFC withthe basal ganglia and thalamus.15,78 The network isrelevant in ADHD because it has a role in regulatingascending sensory information that reaches thePFC and assigning salience to this information(ie, selecting what information is important andwhat is not), as well as in motivation and inhibitinginappropriate actions.78 Interestingly, diminishedactivity of this network during tasks of motorinhibition and cognitive shifting have been shownto correlate with persistence and severity of ADHDTable 2. Brain Networks Involved in tive-executivenetworkDLPFC, posterior parietal cortexInvolved in executive function, working memory, selectiveand sustained attention; regulating emotion; planning ofmotor activityCortico-limbic networkVLPFC, amygdala, hypothalamus, brainstemRegulating level of , basal ganglia, thalamusRegulating and assigning salience to sensory information;inhibiting inappropriate actions, motivationDefault mode networkMPFC, posterior cingulate cortex, lateral parietal Involved in self-reflection, planning future activities,cortex, precuneus, medial temporal lobemonitoring environmentDorsal attentionalnetworkPrecentral and parietal regionsMediating goal-directed, executive control processes,including reorienting attention during visual attentionalfunctioningMotor networkPrimary and secondary motor cortices,supplementary motor area, putamen,thalamus, cerebellumInvolved in motor activityVentral attentionalnetworkTemporoparietal junction, frontal operculum,anterior insulaMonitoring environment for emergence of salient stimuliand interrupting ongoing activity when necessaryVisual networkOccipital visual cortex and temporalstructuresInteracting with dorsal attentional network to maintainattention and suppress attention to irrelevant stimuliADHD, attention deficit/hyperactivity disorder; DLPFC, dorsolateral prefrontal cortex; MPFC, medial prefrontal cortex; PFC, prefrontal cortex; VLPC,ventrolateral prefrontal cortex.The Neurobiology of ADHD — April 20207
Figure 5. Select brain networks involved in attention.15A. Cognitive-executive networkTop-Down Guidance ofAttention and ThoughtDorsalSensoryCorticesPrefrontalCortexBasal l/RewardSystemsB. Cortico-striatal-thalamic-cortical and corticothalamic-cerebellar ActionsPrefrontalCortexBasal l/RewardSystemsC. Cortico-limbic networkDorsalBasal toms.84,85 Connections in the cortico-limbicnetwork (Figure 5C) originate from the ventral PFCand link to limbic areas, such as the amygdala andhypothalamus, as well as with brainstem NE nucleithat regulate level of arousal.76,81,86 Dysfunction ofthese connections in ADHD may result in emotionallability and deficits in impulsivity and motivation.80The Neurobiology of ADHD — April 2020More recent understanding of the neurobiologicalunderpinnings of ADHD is based on restingfunctional network imaging. Altered activity infunctional brain networks involved in ADHD ishypothetically linked to compromised responseinhibition and impulsivity, difficulty sustaining andappropriately shifting attention, altered arousaland vigilance, deficits in working memory andexecutive function, and impairment of socialcognition.53-55,87-89 Functional imaging studieshave also looked at fronto-amygdalar connectionsand the ventral attentional network. Atypicalfronto-amygdalar connectivity and reducedVLPFC‑amygdalar connectivity in ADHD hasbeen linked to inadequate emotional control andemotional reactivity (behaviors that sometimesaccompany ADHD),90 while malfunction of ventralattentional pathways has been associated withmotivational deficits and difficulty delayinggratification (common symptoms of ADHD).2Moreover, VMPFC functional deficits have beenlinked not only to impaired motivational control, butalso to conduct disorder in individuals with ADHD.91Resting functional network imaging is also usedto support more contemporary elaborations ofADHD underpinnings. The frontoparietal networkincludes the DLPFC, VLPFC, anterior PFC, ACC,and the inferior parietal lobes (these regions arealso described as the cognitive executive network[CEN]), as well as the lateral cerebellum, caudate,and anterior insula. Its main role is to exerciseexecutive control and participate in decisionmaking. Most of the components of this networkdemonstrate reduced activity in individualswith ADHD, except the dorsal ACC, which hasdemonstrated heightened activity (possibly acompensatory adaptation) in some studies.1,92,93The previously mentioned ventral attentionalnetwork shares components with the saliencenetwork and includes the temporoparietal junction,operculum, and anterior insula. It is tasked withmonitoring the environment for emergence ofsalient stimuli and interrupting ongoing activity8
when necessary.1 The dorsal attentional network iscomposed of precentral and parietal regions (alsoshares components with the CEN) and appears tohave diminished activity in ADHD, which coincideswith inattentiveness, working memory deficits, andinadequate response inhibition.1The motor network includes the primary motorcortex, secondary motor cortex (ie, the premotorcortex and supplementary motor area), primaryand secondary sensory cortices, putamen,thalamus, and cerebellum.1,94 Individuals withADHD have been shown to manifest decreasedactivation of the primary and premotor corticescompared with controls. Substantially reducedcortical inhibition in ADHD has been correlatedwith deficient motor performance.1The visual network includes the occipital visualcortex and temporal structures. It interacts with thedorsal attentional network to maintain attentionand suppress attention to irrelevant stimuli.1Decreased cortical and gray matter volume in theoccipital cortex has been reported in individualswith ADHD.1,95 Interestingly, a 33-year follow-upstudy of childhood-diagnosed ADHD found anassociation between persistence of an ADHD anddecreased occipital cortical thickness.1Main hubs of the DMN are the medial prefrontalcortices, posterior cingulate cortex, precuneus,and medial temporal lobe.1,82 Increased DMNactivity coincides with self-reflection, rumination,reminiscing, processing social information, andplanning future activities.96 Typically, the DMNis not active when an individual is engaged incognitive-executive tasks.96 Convergent imagingevidence suggests that individuals with ADHDhave diminished recruitment of DMN activity whenengaged in tasks requiring focus and sustainedattention.97 Daydreaming and distractibilitycommonly described in children with ADHDmay be a consequence of inadequate DMNsuppression during cognitive tasks.1 ProperThe Neurobiology of ADHD — April 2020deactivation of DMN in ADHD occurs only incircumstances of elevated salience or withstimulant use.1,98 One can wonder whether thetendency to procrastinate in individuals withADHD may be a pseudo-adaptive maneuverdirected toward increasing salience andsuppressing distracting DMN activity. Furthersupporting these findings, newer studies havefound decreased connectivity between the dorsaland ventral attentional networks and increasedconnectivity within the DMN in individuals withADHD relative to controls.99,100Due to the high rate of comorbid depression andanxiety in ADHD,7 one may question whetherthese 3 disorders share common neurobiologicalalterations. A recently published paper looking atmood and anxiety disorders evaluated whethertheir shared clinical features are reflected inshared neurobiological substrates.101 Basedon a meta-analyses of 226 relevant studiesin mood and anxiety disorders, alterations inbrain functioning were found to be similar andcorrelated with cognitive deficits and negativeemotions (ie, transdiagnostic convergence).These results suggest that the symptoms ofmood and anxiety disorders are associatedwith similar neurobiological patterns.101 Ofnote, although ADHD was not included inthis meta-analysis, many of the ADHD-relatedneurobiological alterations discussed aboveare consistent with those observed for moodand anxiety disorders, lending support for thepathophysiological overlap between ADHD andthese comorbidities.41,102key takeaway: Multiple brain networksare involved in attention, with reducedfunction of these networks associated withsymptoms and characteristics of ADHD,including deficits in sustained attention,response inhibition, executive function,and emotional control.9
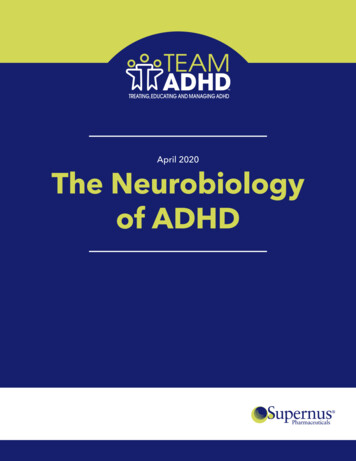
ALTERED NEUROTRANSMISSION IN ADHDIn addition to studies implicating candidate genesregulating NE and DA synthesis and breakdownin ADHD, imaging studies have provided furthersupportive evidence of catecholamine and otherneurotransmitter dysregulations in ADHD (Table 3).Table 3. Potential Neurotransmitters Involved in ADHD52,103-107NeurotransmitterAttention-related functionsDAPlanning and initiation of motorresponse, reaction to novelty,processing of rewardNEArousal modulation, cognitiveprocessing5-HTManagement of depression, anxiety,and sleep; emotional regulationGABAMotor control, behavioral inhibitionGluLearning, memory5-HT, serotonin; ADHD, attention deficit/hyperactivity disorder; DA,dopamine; GABA, gamma-aminobutyric acid; Glu, glutamate; NE,norepinephrine.Functional imaging studies, such as positronemission tomography and single-photon emissioncomputed tomography, which use selective ligandsfor the dopamine transporter (DAT), have reportedincreased DAT binding in up to 70% of children andadults diagnosed with ADHD, indicating a higherdensity of DAT in the brains of these individualsthan in controls.2,108 It is important to mention thatthis is not conclusive, as a number of studies havenot found altered DAT binding in ADHD, and it ispossible that medication status may explain someof the discrepancy.2,108 Both reduced and elevatedDA receptor D2 availability, as well as reducedD2 and D3 binding in the striatum and nucleusaccumbens, have also been noted, differentiatingADHD from control groups.2,108,109Absence of appropriate radioligands for NEhas limited imaging research into NE function inADHD,2 however, non-imaging evidence for NEdysfunction in ADHD comes from multiple othersources. Neurobiological evidence includes theabundance of the α2A adrenoceptor subtype in theThe Neurobiology of ADHD — April 2020PFC110 and enhanced PFC functioning followingstimulation of postsynaptic α2A receptors by NE.111Genetic studies have found an association betweena variation in the gene encoding for dopamine ßhydroxylase, resulting in reduced NE synthesis112and deficits in sustained attention.113,114 The roleof NE dysfunction in the pathogenesis of ADHDis also supported by the fact that all US Food andDrug Administration–approved medications forADHD have either direct or indirect effects onNE, presumably leading to improvement of PFCfunction.114 Peripheral levels of NE, monoamineoxidase, and the NE metabolite, 3-methoxy4-hydroxyphenyl-ethylene glycol, are beingstudied as biomarkers that could differentiateindividuals with ADHD from controls, as well asreflect symptom severity and predict treatmentresponse.115Evidence of catecholamine dysfunction in ADHDlends further credibility to the pathophysiologicalhypothesis implicating prefrontal cortical, caudate,and cerebellar dysfunction. Studies have found thatthe PFC is especially sensitive to its neurochemicalenvironment, particularly DA and NE signaling.111These catecholamines are so critical to the functionof the PFC that either too little or too muchneurotransmitter results in impaired functioning.15,116In fact, DA and NE regulate the activity of prefrontalpathways in an inverted u-shaped dose-responsemanner (Figure 6).111 Namely, hypoactive andhyperactive catecholamine signaling in thesecircuits (including excessive DA signaling dueto stress or an excessive dose of a stimulantmedication) can cause disruption in attention,impulse control, and executive function.15,111 Thishas ramifications for ADHD treatment, as currentlyapproved pharmacotherapies (both stimulantsand nonstimulants) correct for catecholamineimbalance in the PFC.116As was the case with catecholamines, studies havepointed to involvement of variations of genes in theregulation of Glu signaling.42 Further supporting10
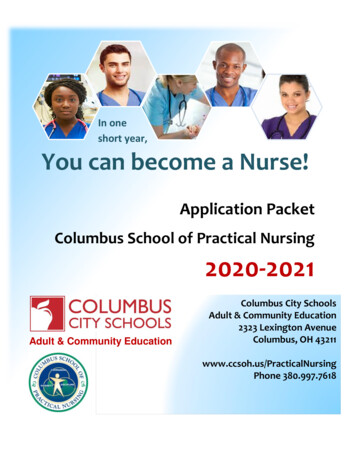
Figure 6. Catecholamine levels and PFC function (adapted from Arnsten 2009).111,117OptimalFocusedOrganizedResponsiblePFC AbilitiesEngage NE α 2(mostly α 2A, α 2C)Moderate DA edAnxiousIrritable“Brain freeze”ExcessiveInadequateEngage NE α1, ß1(mostly α1B and α 2C?)Too much DA D1Too littleNE and DALevels of Catecholamine ReleaseIncrease With Arousal StateDA, dopamine; NE, norepinephrine; PFC, prefrontal cortex.Note: Optimal NE levels also engage α1, associated with wakefulness and alertness.118these findings, a proton magnetic resonancespectroscopic (MRS) study reported reduced Gluglutamine (Glx) concentrations in the striatumof participants with ADHD relative to controls.Interestingly, lower basal ganglia Glx was significantlycorrelated with greater symptom severity in theADHD group.119 Gamma-aminobutyric acid (GABA)has also been implicated in ADHD, with an MRSstudy reporting reduced GABA concentrations insomatosensory and motor cortices of participantswith ADHD compared with controls, possiblyreflecting deficient intracortical inhibition in ADHD.104Serotonin also appears to play a role in ADHD.Functional brain imaging of 5-HT binding andplatelet 5-HT binding in individuals with ADHD haveyielded inconsistent results,109 most likely supportingthe biological heterogeneity of ADHD. Furthermore,we previously mentioned that α2A adrenoceptorsare implicated in the pathophysiology of ADHD: notonly are α2A adrenoceptors in the PFC involved inregulation of NE release, but they are also involvedin the modulation of 5-HT synthesis and release.120Moreover, data suggest that 5-HT signalingincreases DMN activity, a known imaging finding inThe Neurobiology of ADHD — April 2020ADHD.121 Studies of the 5-HT transporter (SERT) andthe
relationship problems/divorce in adolescents and adults.3,13,17-23 ADHD also imparts a higher mortality rate. Studies show up to a 3-times greater risk of premature death and up to a 4-times greater risk of death from all causes in individuals with ADHD compared to individuals without ADHD, often due to accidents and