Transcription
Strengthening academic psychiatry in the UKMarch 2013
The Academy of Medical SciencesThe Academy of Medical Sciences is the independent body in the United Kingdom (UK) representingthe diversity of medical science. Our mission is to promote medical science and its translationinto benefits for society. The Academy’s elected Fellows are the United Kingdom’s leading medicalscientists from hospitals, academia, industry and the public service. We work with them to promoteexcellence, influence policy to improve health and wealth, nurture the next generation of medicalresearchers, link academia, industry and the National Health Service (NHS), seize internationalopportunities and encourage dialogue about the medical sciences.Cover image taken from - Anacker C., et al. (2013). Glucocorticoid-related molecular signaling pathwaysregulating hippocampal neurogenesis. Neuropsychopharmacology doi:10.1038/npp.2012.253.ISBN No: 978-1-903401-36-1
Strengthening academic psychiatry in the UKMarch 2013
Acknowledgements and disclaimerThe Academy of Medical Sciences (AMS) is most grateful to Sir David Carter FRSE FMedSci and to themembers of the working group for undertaking this review. We thank the Academy’s Council membersand staff, study observers, external review group, workshop attendees and all individuals whocontributed to the report. The Academy is grateful to the Wellcome Trust for its financial contributionand for seconding a member of staff, Dr Kate Adcock, to the study. The completion of this study wouldnot have been possible without the hard work and commitment of the study secretariat.This report is published by the AMS and has been endorsed by its Officers and Council.Contributions by the working group were made purely in an advisory capacity. The members of theworking group participated in an individual capacity and not as representatives of, or on behalf of,their affiliated hospitals, universities, organisations or associations. Their participation should notbe taken as endorsement by these bodies.All web references were accessed in February 2013. The Academy of Medical Sciences 2013
CHAPTERCONTENTSTITLEContentsSummary51 Introduction92 Issues facing psychiatry and clinical academic psychiatry113 Strengthening academic psychiatry234 Recommendations43Annex I Working group membership47Annex II Review group membership49Annex III Stakeholder engagement51Annex IV Abbreviations and acronyms553
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UK4
CHAPTERSUMMARYTITLESummaryMental ill health accounts for some 15% of thepsychiatrists in medical schools and beyond ifdisease burden in developed countries, andrecruitment is to be enhanced. It is essentialpatients with serious mental illness diethat psychiatrists position their specialty so that25 years earlier than the rest of the population.it can attract the brightest and best studentsYet despite these worrying statistics, spendingand postgraduate trainees. The recruitmenton mental health research currently amountscampaign launched recently by the Royalto only one-twentieth of the total UK healthCollege of Psychiatrists is timely. Senior clinicalresearch spend. In addition, there are currentlyacademic psychiatrists in particular mustconcerns about recruitment to psychiatry in theportray psychiatry as an exciting scientificUK, and the Academy has previously identifiedspecialty that is integrated in the broaderpsychiatry as a vulnerable academic discipline.context of overall patient care and offeringThis is at a time when the UK needs a poolgreat potential for research at undergraduateof talented academic psychiatrists who canand postgraduate levels.strengthen our understanding of mental illnessand take full advantage of scientific advances inits prevention, diagnosis and treatment.Balancing the needs of clinical andacademic trainingIn response to these concerns, the Academyestablished a high-level working group inPostgraduate training in psychiatry mustearly 2012 under the chairmanship of Siremphasise the underlying science base of theDavid Carter FRSE FMedSci to consider how todiscipline and produce a workforce that canstrengthen academic psychiatry in the UK. Thetake full advantage of the march of science andworking group engaged with key stakeholdersadapt to changing patient and service needs.through meetings, correspondence, a widelyThe subset of psychiatrists who wish to developcirculated discussion paper and a workshop.a clinical academic career should receive mostAlthough the main focus of the inquiry was theof their clinical training in an environmentrecruitment and training of clinical academicwhere research is valued.psychiatrists, the related challenges facingpsychiatry in general were also considered.Training programmes must encourage andmaintain a flexible approach to balancingclinical and research training needs. SeniorProfile of psychiatryclinical academic psychiatrists need to establishand maintain a strong presence in trainingRecruitment to psychiatry has undoubtedlyprogrammes to maximise their influence onsuffered from a perception that it is remotetraining and the career development of clinicalfrom the rest of medicine, insufficientlyacademics.scientific and concerned with the treatmentof stigmatised and challenging patients ingeographically isolated hospitals. In part, theAcademic training opportunitiesnegative perception may reflect loss of selfesteem among psychiatrists who no longer seeNurturing the career development of trainees isthemselves as having a lead role in a disciplinethe key to strengthening academic psychiatry in‘de-medicalised’ by multi-professional working.the UK. The Academy welcomes the growth oftraining schemes that integrate clinical trainingIt is clear that much needs to be doneand academic development. When aspiringto enhance the profile of psychiatry andclinical academic psychiatrists take time out of5
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UKclinical training to undertake doctoral researchboundaries between diseases of the brain andit is essential that they do so in optimal settingsof the psyche is also underlining the need forthat favour multidisciplinary interaction andclinicians to have a broader understanding ofprovide excellent supervision and mentorship.the scientific basis of the discipline. TrainingWhen applying for research training fellowships,programmes need to develop flexibly sopsychiatrists appear to do as well as those inthat training in psychiatry can be integratedother specialties and concerns about capacityappropriately with that of other specialties. Thein academic psychiatry can be addressedAcademy strongly supports the developmentby increasing the number of high-qualityof integrated training opportunities. It stronglyapplicants, providing excellent mentoring andencourages the Royal College of Psychiatristsencouraging cross-discipline linkages.to work with other Colleges and thoseresponsible for postgraduate training in theUK to develop cross-training opportunitiesSustaining academic careersfor trainee psychiatrists. Of the options forintegrated training considered in this review,It is important to ensure that there is anthe Academy recommends the creation of aappropriate balance between the availabilitynew sub-specialty that will allow psychiatristsof training posts and more senior academicto have up to two years of training in a relatedpositions in psychiatry. The Medical Schoolsspecialty important for their clinical academicCouncil is encouraged to continue monitoringdevelopment. Given the complex naturethe number of academic positions in UKof mental illness and its management, themedical schools so that it can be determinedAcademy sees this option as the best take-offwhether the desired increase in clinical lecturerpoint for an evolutionary approach to integratedpositions is being matched by a significanttraining.increase in the number of senior lecturers andreaders. The UK is fortunate to have severalAlthough this Review has been primarilyoutstanding centres of excellence linkedconcerned with training for clinical academicto or based in Higher Education Institutes.psychiatrists, the Academy holds strongly toThese centres provide extensive researchthe view that integrated training opportunitiesand clinical training opportunities for aspiringshould be available for all trainee psychiatristsacademic psychiatrists. The Academy stronglyand tailored to their career needs and thosesupports a strategic approach on the partof the patients they will serve. To developof research funders to develop and sustainand implement new and effective treatmentsthese internationally competitive centres offor mental health disorders, the UK will needexcellence. Collaboration between centres andcadres of clinical academic psychiatrists whowith university departments of psychiatry iswill not be constrained by current boundariesstrongly encouraged.between specialties and who have acquiredexpertise in other related scientific disciplines.Interdisciplinary opportunitiesRecommendationsBiomedical advances are currently posing majorquestions about the traditional boundariesThis review has developed recommendations,between specialties in medicine. It is imperativethe aims of which are grouped in thethat training programmes are refined asthree areas outlined below. Individualknowledge of disease and its prevention,recommendations are set out in the finaldiagnosis and management increases. Inchapter of this report.psychiatry a blurring of traditional conceptual6
CHAPTERSUMMARYTITLEEnhancing recruitment to academicThe Academy attaches great importance topsychiatrythe drive to strengthen academic psychiatry Improving recruitment to psychiatry andin the UK. It appreciates that implementationclinical academic psychiatry in medicalof the recommendations made in this reviewschools.will constitute a sustained but surmountableImproving career pathways for medicalchallenge. The Academy is confident thatgraduates aspiring to a career in academicestablished psychiatrists, the Royal College ofpsychiatry.Psychiatrists, those concerned with medical workforce planning and training programmes,Increasing research opportunities forUniversities, medical schools and their Deans,academic psychiatristsresearch funders and regulators will work Improving research capacity in clinicalconstructively with each other to accomplishacademic psychiatry.desirable and necessary change. Ensuring that trainee clinical academicpsychiatrists can carry out doctoralresearch in optimal settings. Providing excellent mentoring for trainees. Ensuring that clinical academic psychiatryhas a balanced workforce that is able todevelop and deliver mental health services. Enhancing the international standing of UKresearch in clinical science by realising thefull potential of centres of excellence andcollaboration between them.Integrating psychiatry with otherneuroscience disciplines Removing unhelpful and constrainingboundaries between psychiatry and relatedspecialties through a pragmatic and evolutionary approach to development of novelintegrated training programmes.7
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UK8
1 INTRODUCTIONCHAPTER TITLE1 IntroductionBiomedical and clinical research is criticallylarge numbers of patients, samples and data.important in the drive to improve healthAs key parts of its vision for improving mentaland healthcare in the UK and has significanthealth research, the Review identified the needimplications for the nation’s wealth andto increase research capacity and innovation,wellbeing. Given the large burden of disabilityaugment support for multidisciplinary researchcaused by poor mental health, it is vital thatgroups, enhance research training and ensurethe UK maintains excellent psychiatric servicesa critical mass of research workers. Greaterand an academic psychiatry constituency that isbreadth in structured training programmes,able to contribute fully to improving knowledgecapacity building through studentships andof mental illness and its prevention, diagnosisfellowships, and project funding calls toand management. In 2009 an Academy reportstimulate research activity were all seen asreflected concern that most UK academicimportant in incentivising and strengtheningspecialties outside internal medicine appearedresearch training in mental health. Academicto have experienced some decline (datapsychiatry in the UK must be able to play afrom Medical Schools’ Council); psychiatryfull part in the burgeoning of mental healthwas seen as one of several ‘vulnerable’research and the improved management ofacademic specialties where there weremental illness.particular concerns about decreasing academicrecruitment and unfilled academic posts.1In January 2012 the Academy formed aworking group to develop a position paper onThe Medical Research Council (MRC)-led Reviewthe training of academic psychiatrists in the UK.of Mental Health Research in 2010 chairedThe decision was made in response to concernsby Professor Christopher Kennard FMedSciexpressed about the state of academicconcluded that although the UK is well-placedpsychiatry training and against a backgroundto be at the forefront of advances in basicof a marked recent decline in fill rates ofunderstanding and improved prevention,psychiatry training positions and a perceptiondiagnosis and management of mental illness,that fewer trainees were taking up an academicmental health research spend (estimatedcareer in the specialty.at 5–6.5% of total UK health researchspend) is not proportionate to the burden ofThe terms of reference for the working groupdisease (estimated as 15% of health burdenwere as follows:in the developedworld).2,3The UK base in To identify the challenges and barriers,neuroscience, social science and mental healthperceived or otherwise, in recruiting andresearch needs to be better integrated with theretaining trainees in academic psychiatrypotential of the National Health Service (NHS)and make recommendations to strengthento conduct large-scale studies and with thepotential of industry to develop novel therapies.the workforce in this area. To consider how psychiatry and theMajor obstacles to progress were identified asneurosciences can work across traditionalthe suboptimal capacity of UK mental healthboundaries to develop an academicresearch, the stigmatisation of mental illnesstraining programme that will equip futureand the need to improve research access togenerations with the knowledge and skills123The Academy of Medical Sciences (2009). Building clinical academic capacity and the allocation of resources across academic tmlMental Health Foundation (2010). Economic burden of mental illness cannot be tackled without research arch-Nov2010.pdfMedical Research Council (2010). Review of mental health research - report of the Strategic Review d/index.htm?d MRC0068489
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UK required to meet healthcare needs.general in the UK. The working group did notWhere appropriate, to make comparisons ofconsider issues facing specific sub-specialtiesclinical academic workforce profiles in otherwithin psychiatry: rather, it considered wayscountries, in particular the USA.of strengthening clinical academic psychiatryacross the discipline. Nevertheless, the workingThe working group met on two occasionsgroup was aware that some sub-specialties,(in March and April 2012), supplemented itssuch as forensic psychiatry and psychiatrywork by discussions with leading figures inof learning disability, may have particularacademic psychiatry in the UK and overseas,difficulties in recruitment, training andand obtained evidence from organisationsacademic profile.responsible for the direction, funding andregulation of clinical academic training in theIt is also important to emphasise that whenUK. A discussion paper was approved by thediscussing science and research fieldsAcademy’s Council in June and circulatedrelevant to clinical academic psychiatry infor comment to selected individuals andthis document, the working group and theorganisations. The Academy hosted a workshopAcademy see them as stretching widely fromin September 2012 that allowed furtherbasic neuroscience to clinical neuroscience,discussion and input to the work of the workingthrough primary care to secondary and highlygroup. The resulting document was agreed byspecialised (tertiary) care, and through athe working group in October, subjected to thebroad range of specialty areas with whichAcademy’s normal governance procedures andpsychiatry has interplay. These areas includethen endorsed for publication at the meeting ofneurology and other medical specialties,the Academy’s Council in November 2012.neurosurgery, neuroimaging, psychology,paediatrics, obstetrics and perinatal medicine,In undertaking its remit, the working groupcare of the elderly, primary care, populationconcentrated on the training of clinicalhealth, infectious diseases, social medicine andacademic psychiatrists but saw it as importantresearch fields such as epidemiology, healthto set issues currently facing academicservices research and molecular genetics.psychiatry in the broader context of thechallenges currently facing psychiatry in10
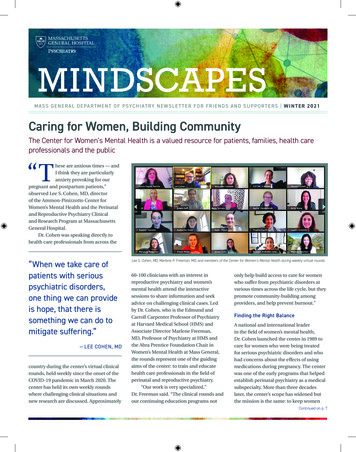
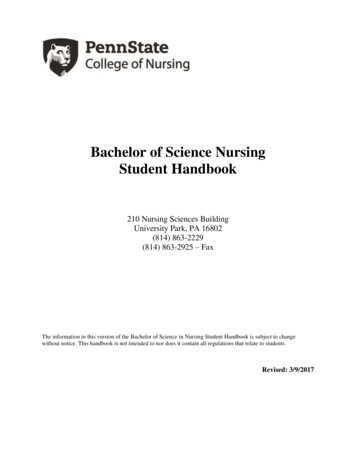
2 ISSUES FACING PSYCHIATRY AND CLINICAL ACADEMICCHAPTERPSYCHIATRYTITLE2 Issues facing psychiatry and clinical academic psychiatryRecruitment to clinical academic psychiatrypsychology and wish to pursue these interestsneeds to be considered in the context ofat university. However, many pupils electingconcern that low levels of recruitment intoto pursue careers in basic neuroscience orpsychiatry in general in the UK will inevitablypsychology may do so because they are notreduce the pool of talented trainees wishing tofully aware of the opportunities presented bybecome clinical academic psychiatrists.psychiatry and the clinical neurosciences.Throughout this report reference is made to the2.1.2 Medical schooltraining pathway for psychiatrists and academicPsychiatry currently has an image problem inpsychiatrists. A typical training pathway formany medical schools.4,5 A common perceptionacademic psychiatrists is illustrated in Box 1.in other sectors of the profession is that itis remote from the rest of medicine, notsufficiently scientific, and deals with patients2.1 Recruitment issues in secondaryschools and medical schoolswho are stigmatised and present a difficulttherapeutic challenge where there are limitedprospects of success. In part, psychiatry’s2.1.1 Secondary schoolproblem may also reflect loss of self-esteemMany secondary school pupils are interestedon the part of psychiatrists who no longer seein the neurosciences, mental health andthemselves as having an uncontested leadrole in a discipline ‘de-medicalised’ by theBox 1: Typical training pathway for academic psychiatrists in F1F2Specialty trainingCCTNIHR AcademicClinical Fellow(25% academic)NIHRClinical Lecturer(50% academic)CT1 CT2 CT3ST4 ST5 ST6ConsultantSenior LecturerSenior Clinical FellowSub-specialty trainingAcademicopportunitiesSSCIntercal. BScMB/PhD4 inicianScientistFellowshipMedical school is followed by two years of foundation training (F1, F2). Psychiatry traineesundergo three years of core training (CT1–3) and a minimum of three years of advancedtraining (ST3–6) before gaining their certificate of completion of training (CCT) in one of sixpsychiatry specialties: general psychiatry (with the option of three sub-specialties in liaisonpsychiatry, rehabilitation psychiatry or substance misuse psychiatry); child and adolescentpsychiatry; forensic psychiatry; old age psychiatry; psychiatry of learning disability; or medicalpsychotherapy.4 Rajagopal S, Rehill KS & Godfrey E (2004). Psychiatry as a career choice compared with other specialties: a survey of medical students.The Psychiatrist 28, 444–446.5Curtis-Barton MT & Eagles JM (2011). Factors that discourage medical students from pursuing a career in psychiatry. The Psychiatrist 35,425–429.11
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UKadvent of multi-professional working.6 In manyyears. Commenting on these trends, Professorcentres, psychiatry’s image and ability to relateJohn Oldham, President of the Americanto mainstream medicine is not helped by thePsychiatric Association said ‘we need to reachgeographical isolation of ageing psychiatricout to medical students in more effective wayshospitals at some distance from the mainthan simply exposing them to a four-weekteaching hospital campus.clerkship on an inpatient unit with no follow-upof the patients they have cared for’.9 WhereasTo medical students, psychiatry can appearProfessor Sidney Weissman (Past President, USremote from the rest of medicine, divorcedAssociation of Directors of Psychiatric Residencyfrom its science base and perhaps lackingTraining Programmes) remarked ‘The picture ofclinical academic role models. This maycontemporary psychiatry is confusing to many ofdisillusion students who initially wereus and must be confusing to our students’ andinterested in a career in psychiatry and lead to‘until we restore clarity to what our disciplineunfavourable comparisons with other clinicalis and develop creative ways to communicateneuroscience disciplines that appear to beit in a few weeks of psychiatry clerkship tocapitalising more effectively on the recentour medical students, I am concerned thatexciting growth in scientific understanding.recruitment will continue to decline.’An unintended consequence of the ResearchAssessment Exercise (RAE) has been adowngrading of the importance of teachingin some medical schools and this will remain2.2 Recruitment to postgraduatetraining in psychiatry in generala concern in the forthcoming ResearchExcellence Framework.7 This downgrading2.2.1 Psychiatry: a discipline in crisis?coupled with a diminished capacity of someAccording to the Medical Programme Board foruniversity departments of psychiatry may haveEngland, the ratio of applicants to psychiatrysignificantly weakened psychiatry teaching totraining places fell beneath 1:1 in 2010 inthe detriment of recruitment. A review of UKEngland. Although the ratio may since havemedical graduates in years one and three afterimproved slightly (to 1.4:1 in 2011) there canqualification shows that three factors havebe no grounds for complacency. In Englandgreater influence on choice of psychiatry asand Wales at the end of the second recruitmentopposed to other careers: experience of theround in August 2011, only 83% of the 478subject as a medical student, self-assessmentCore Training year-one (CT1) vacancies hadof skills and aptitudes, and anticipated hoursbeen filled, a far smaller proportion than otherand working conditions.8major specialties. In 2012 the fill rate for CT1vacancies in psychiatry rose only slightly toConcern about the attractiveness of psychiatry85.3%. The uneven geographical distribution ofto medical students is not confined to the UK.filled posts may leave some parts of the UK atIn 2012 the number of senior medical studentsconsiderable disadvantage.applying for psychiatry residency programmesin the USA dipped to 616 from a high of 670 inAlthough recruitment may be better in Scotland2010. This means that only 3.9% of graduatingand Northern Ireland, numbers of applicantsUS medical students now enter the specialty,are also lower than desirable and work tothe lowest proportion to do so in the past sixreshape the medical workforce in Scotland is678912Craddock N, et al. (2008). Wake-up call for British psychiatry. British Journal of Psychiatry 193, 6–9.The Academy of Medical Sciences (2010). Redressing the balance: the status and valuation of teaching in academic careers in the biomedicalsciences. http://www.acmedsci.ac.uk/index.php?pid 99&puid 181Goldacre MJ, et al. (2012). Choice and rejection of psychiatry as a career: surveys of UK medical graduates from 1974-2009. British Journalof Psychiatry published ahead of print October 25, 2012, doi:10.1192/bjp.bp.112.111153.Moran M (2012). Fewer US grads matching in psychiatry. Psychiatric News 47 (8), 1b–30.
2 ISSUES FACING PSYCHIATRY AND CLINICAL ACADEMIC PSYCHIATRYuncovering concern about unfilled consultantWhereas the combinations of three four-posts in mental health. Further concerns relatemonth attachments are fixed in F1 in Scotland,to the quality of those applying to train inthere is some flexibility in the combinationspsychiatry in the UK and the fact that aroundof attachments in F2. As in other parts of the40% of trainees currently fail to pass theUK, there is no impediment to trainees seekingMRCPsych examination, although pass rates areto have four-month attachments in bothmuch higher for UKgraduates.10neurology and psychiatry.It is also recognised that some doctors whoIn England (informed by discussions involvinginitially choose psychiatry do not pursue it asthe RCPsych, Medical Education England, thea long-termcareer.11Reasons given includeUK Foundation Programme and the Departmentperceived lack of respect from medical peers,of Health) the number of psychiatry placementsperceived threat of violence from patients, jobwill rise to 460 posts in both foundation yearsstress, self-assessed unsuitability and concernsby 2014. This will mean that around 45% ofabout lack of evidence-based treatments. Tendoctors will have had psychiatry placementsyears after graduation, 64% of those whoseby the end of their foundation training insole first career choice was psychiatry inEngland.15 However, only a small proportion ofpostgraduate year one were still working in thethese will be academic foundation placements,specialty as opposed to 81% who had chosen itat least in the first instance.as their sole first career choice in year three.122.2.3 Specialty training programmes and2.2.2 Foundation trainingclinical academic trainingThe Royal College of Psychiatrists (RCPsych)There is a growing sense that postgraduatehas been greatly concerned by the relativetraining in psychiatry in the UK, as in alllack of opportunity for foundation programmespecialties, could be improved and becomedoctors to experience working in psychiatry.13much more flexible. There is also concern thatThe 2011 UK Foundation Programme Annualtraining programmes may be unnecessarilyReport reveals that only around 4.6%protracted, particularly for those pursuing anof Foundation Year one (F1) doctors andacademic career or those wishing to acquireapproximately 11.7% of Foundation Year twoexperience in a related specialty while training(F2) doctors rotated through a placementprincipally in psychiatry. There is a perceptionin psychiatry.14 The College also stressesin some quarters that academic and clinicalthe desirability of psychiatry placements inexcellence has been undervalued in traineeAcademic Foundation Programmes for thoseselection, and that the training needs of juniorcontemplating a career in academic psychiatry.staff are too often subjugated to the staffingneeds of the NHS. Lack of flexibility in specialtyIn Scotland, 24% of all foundation traineestraining programmes can have a profoundlycurrently have a four-month post in psychiatry.negative effect on career development,Almost all posts are hospital-based rather thanparticularly in the case of clinical academiccommunity-based and they are predominantlytrainees. Trainees move frequently from postavailable in F2, although a few F1 posts areto post in rotational programmes, have feweravailable in liaison psychiatry in acute hospitals.patient-contact hours, seldom experience101112131415For further information see %20Results%20Report%20-%20August%202011.pdfLambert TW, et al. (2006). Reasons why some UK medical graduates who initially choose psychiatry do not pursue it as a long-term career.Psychological Medicine 36(5), 679–684.Goldacre MJ, et al. (2012). Choice and rejection of psychiatry as a career: surveys of UK medical graduates from 1974-2009. British Journalof Psychiatry published ahead of print October 25, 2012, doi:10.1192/bjp.bp.112.111153.The Royal College of Psychiatrists (2012). Recruitment strategy 2011-2012. y%20%28RCPsych,2012%29.pdfFor further information see eydocsDr Stuart Carney, Deputy National Director, Foundation Programme Office: personal communication13
STRENGTHENING ACADEMIC PSYCHIATRY IN THE UKcontinuity of care, and rarely develop strongThe ‘Inquiry into Modernising Medical Careers’working relationships with their trainers.led by Professor Sir John Tooke PMedSci in 2008highlighted the need for flexibility in integratedThis said, the 2012 GMC survey of all UKclinical academic training pathways so thatpsychiatry trainees reveals an averagetrainees can move seamlessly and withoutsatisfaction score of 82.4%, range across allstigma in and out of conventional clinicalspecialties 76.2–87.8%, overall response ratetraining pathways.17 Although schemes such95%) when trainees were asked about qualityas the Academic Clinical Fellowship in Englandof teaching, clinical supervision and experience,allow some 25% of programme time for trainingwhether they would recommend the postin research methodology and developmentto a friend, and how useful the post wouldof research proposals, the Tooke Report alsobe for their future career. Although traineesrecommended that opportunities should also bein integrated academic training pathwaysavailable for those wishing to pursue a researchwere included in the survey, they were notcareer after entry into higher specialist trainingquestioned specifically as a subgroup aboutschemes. Out-of-
psychiatry in general were also considered. Profile of psychiatry Recruitment to psychiatry has undoubtedly suffered from a perception that it is remote from the rest of medicine, insufficiently scientific and concerned with the treatment of stigmatised and challenging patients in geographically isolated hospitals. In part, the