Transcription
32nd Annual MeetingPosterAbstract BookTrauma and Public Health:Innovative Technology and Knowledge DisseminationNovember 10 –12, 2016Pre-Meeting Institutes, November 9Sheraton Dallas HotelDallas, Texas USAJointly Provided byBoston University Schoolof Medicine andthe International Society forTraumatic Stress Studieswww.istss.org
www.istss.orgCopyright 2016 ISTSS Annual MeetingISTSS 32nd Annual MeetingPoster AbstractsTable of ContentsPagesGuides to Information in the Schedule2-3Thursday Poster Session OneThursday Poster Session One InformationThursday Poster MapStudent Poster Award FinalistsClinical/Intervention Research PostersTechnologyTraining/Education/Dissemination PostersAssessment and Diagnosis PostersClinical Practice PostersBiological/Medical PostersResearch Methodology PostersVicarious Traumatization and Therapist Self-Care PostersGlobal Issues PostersCulture/Diversity PostersCommunity-Based Programs PostersSocial Issues & Public Policy and Multi-Media PostersPrevention/Early Intervention PostersEthics PostersPublic Health PostersThursday Welcome Reception Poster SessionWelcome Reception Poster Session InformationWelcome Reception Poster Floor PlanAging, Trauma and the Life Course SIG PostersComplex Trauma SIG PostersDiversity and Cultural Competence SIG PostersEarly Interventions SIG PostersFamily Systems SIG PostersGender and Trauma SIG PostersIntergenerational Transmission of Trauma & Resilience SIG PostersLesbian, Gay, Bisexual & Transgender (LGBT) SIG PostersPsychodynamic Research and Practice SIG PostersTheory and Traumatic Stress Studies SIG PostersTerrorism and Bioterrorism Related Trauma SIG PostersResearch Methodology SIG PostersTrauma and Substance Use Disorders SIG PostersTrauma Assessment and Diagnosis SIG PostersTraumatic Loss and Grief SIG 9100101102103104105106107108Friday Poster Session TwoFriday Poster Session Two InformationFriday Poster MapClinical/Intervention Research PostersTechnologyTraining/Education/Dissemination PostersAssessment and Diagnosis PostersClinical Practice PostersBiological/Medical PostersResearch Methodology PostersGlobal Issues PostersCulture/Diversity PostersCommunity-Based Programs PostersSocial Issues & Public Policy PostersPrevention/Early Intervention andEthics PostersPublic Health Posters1 PagePresenting Author is 188188-195
ISTSS 32nd Annual MeetingFinal ProgramGuides to Information in ScheduleKeyword Type DescriptionsPrimary Keywords Assessment/Diagnosis (Assess Dx)Biological/Medical (Bio Med)Clinical/Intervention Research (Clin Res)Clinical Practice (Practice)Community-Based Programs (Commun)Culture/Diversity (Cul Div)Ethics (Ethics)Global Issues (Global)Journalism and Trauma (Journalism) Multi-Media (Media)Prevention/Early Intervention (Prevent)Public Health (Pub Health)Research Methodology (Res Meth)Social Issues – Public Policy (Social)Technology (Tech)Training/Education/Dissemination (Train/Ed/Dis)Vicarious Traumatization and Therapist Self-Care(Self-Care) Illness/Medical Conditions (Illness)Intergenerational Trauma (Intergen)Journalism and Trauma (Journalism)Multi-Media (Media)Natural Disaster (Nat/Dis)Neglect (Neglect)(Neuro)Biological Processes/Interventions (Bio/Int)Neuro Imaging (Neuro)Prevention/Early Intervention (Prevent)Primary Care (Care)Psychodynamic Research (Psych)Public Health (Pub Health)Quality of Life (QoL)Rape/Sexual assault (Rape)Refugee/Displacement Experiences (Refugee)Research Methodology (Res Meth)Sexual Orientation and Trauma (Orient)Sleep (Sleep)Social Issues – Public Policy (Social)Substance Use/Abuse (Sub/Abuse)Survivors/Descendants of Historical Trauma (Surv/Hist)Technical Disaster (Tech/Dis)Technology (Tech)Terrorism (Terror)Theory (Theory)Torture (Torture)Training/Education/Dissemination (Train/Ed/Dis)Traumatic Grief (Grief )Vicarious Traumatization and Therapist Self-Care(Self-Care)War – Civilians in War (Civil/War)War – Military/Peacekeepers/Veterans (Mil/Vets)Secondary Keywords Accident/Injury (Acc/Inj)Acute/Single Trauma (Acute)Affective Processes/Interventions (Affect/Int)Aggression/Aggressive Behavior (Aggress)Aging/Lifecourse (Aging)Anxiety (Anx)Assessment/Diagnosis (Assess Dx)Biological/Medical (Bio Med)Child Physical Abuse/Maltreatment (CPA)Child Sexual Abuse (CSA)Chronic/Repeated Trauma (Chronic)Clinical/Intervention Research (Clin Res)Clinical Practice (Practice)Cognitive Processes/Interventions (Cog/Int)Community-Based Programs (Commun)Community/Social Processes/Interventions (Comm/Int)Community Violence (Comm/Vio)Complex Trauma (Complex)Culture/Diversity (Cul Div)Death/Bereavement (Death)Depression (Depr)Developmental Processes/Interventions (Dev/Int)Domestic Violence (DV)(Epi)Genetic Processes/Interventions (Gen/Int)Ethics (Ethics)Ethnicity (Ethnic)Family Relationship Processes/Interventions (Fam/Int)Gender and Trauma (Gender)Genetics/Epigenetics (Genetic)Global Issues (Global)Health Impact of Trauma (Health)Human Rights (Rights)2 Page
ISTSS 32nd Annual MeetingFinal ProgramGuides to Information in ScheduleRegions Central and Eastern Europe and the Commonwealth ofIndependent States (C & E Europe & Indep) Eastern and Southern Africa (E & S Africa) East Asia and the Pacific (E Asia & Pac) Industrialized Countries (Industrialized) Latin America and the Caribbean (Latin Amer & Carib) Middle East and North Africa (M East & N Africa) South Asia (S Asia) West and Central Africa (W & C Africa)Population Types Child/Adolescent (Child/Adol) Adult (Adult) Older People/Aging (Older) Both Adult and Child/Adolescent (Lifespan) Mental-Health Professionals (Prof) Other Professionals (Other)Presentation LevelAll presentations designate the knowledge/skill level required of the participant as either: Introductory (I), Intermediate (M)or Advanced (A). These are used as a general guide only since attendees have very diverse educational and professionalbackgrounds.Introductory (I): Presentationsthat all participants (includingundergraduate students) with anyappropriate background will be able tofully comprehend and/or appreciate.Presentations will discuss concepts thatare considered basic skills/knowledgefor those working in the field.Intermediate (M): Presentationsthat participants may more fullycomprehend/appreciate if they have atleast some work experience in the topicto be discussed.Advanced (A): Presentations consistingof concepts requiring a high-level ofprevious educational background, orwork experience, in the particular area/topic to be discussed as well as beingmost geared for specialists and those inadvanced stages of their career.Presentation Type Descriptions* Case Study Presentation Poster PresentationSessions use material from a single or a set of cases toillustrate clinical, theoretical or policy issues. These sessionsmay involve the audience in discussion of the case materialpresented.Individual presentation in a poster format on a topic relatedto traumatic stress, typically including the presentation ofresearch data. Media PresentationInstitutes are full- or half-day sessions that provide anopportunity for intensive training on topics integral to theconference program, presented by leaders in the field.Session involving presentation of a segment of film, video,music, drama, literature, artwork or other form of mediarelevant to traumatic stress, along with discussion. Oral Paper PresentationIndividual presentations of no more than 15 minutes on a topicrelated to traumatic stress, typically including the presentationof research data. Panel PresentationSessions that include three to four participants discussing acommon theme, issue or question. Panels may include shortstatements during which panelists outline diverse or similarapproaches to the same question. Panels are typically moreinteractive than symposia, involving active discussion amongthe panelists.3 Page Pre-Meeting Institute (PMI) SymposiumSession that includes a group of three to four sequentialpresentations, each related to the overall theme of thesymposium. Workshop PresentationInstructional session that helps increase participants’understanding and skill in a particular area of interest. Suchsessions may include active involvement of the audience.* Presentation types are color-coded throughout the schedule.
www.istss.orgCopyright 2016 ISTSS Annual MeetingPoster Session One PresentationsThursday, November 10, Grand Hall5:30 p.m – 6:30 p.m.Author Attended Poster Session OneThursday, November 105:30 p.m. to 6:30 p.m.Poster OrganizationEach poster is scheduled for either Author Attended Poster Session One on Thursday, the Featured PosterPresentations at the Welcome Reception or Author Attended Poster Session Two on Friday and includes a timeperiod when the presenting author is available to answer questions.Posters are organized in the conference program by poster number on each day. The presenting author is bolded. Afloor map showing the layout of posters is on the next page.Key:Poster # Number (Primary keyword, Secondary Keywords, Population type)Presentation Level – Region Keyword type descriptions can be found on page 2.Regions and Population Types can be found on page 3.Presentation levels and descriptions can be found on page 3.Session One: Thursday, November 10Poster Setup:8:00 a.m. – 10:30 a.m.Poster Viewing:10:30 a.m. – 5:30 p.m.Author Attended Poster Session:5:30 p.m. – 6:30 p.m.Poster Dismantle:6:30 p.m.Poster DismantleImmediately following your scheduled poster session, display materials must be taken down and removed. Items notremoved by the appointed poster dismantle time will be disposed of and are not the responsibility of ISTSS.4 PagePresenting Author is Bolded
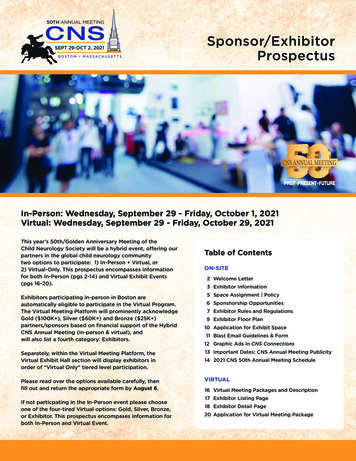
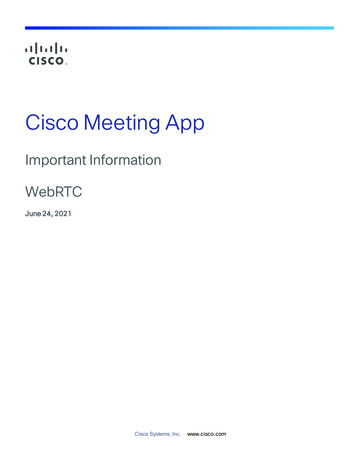
Copyright 2016 ISTSS Annual MeetingISTSS 32nd Annual MeetingThursday Poster Session One Distribution MapGrand nationAssessment/Diagnosis223 224 225 226 227 228229 230 231 234235 236 237 238240 241 242 243244 245 246 247248 249 251 252 253 254 255 256222 219 218 217 216 215214 213 212 211210 209 206 205272 271 270 269268 267 266 265264 263 262 261 260 259 258 257TechnologyClinical Practice193 194 195 196197 198 199 200201 202 203 204273 275 277 278192 191 190 189188 187 186 185184 183 182 181Clinical Intervention/ResearchBiological/Medical279 280 281 283284 285 286 287301 300 299 298297 296 295 293292 291 290 289 MethodologyGlobalVicarious Traumatization & Therapist Self CareCulture/Diversity167 168 169 170171 172 173 174177 178 179 180302 303 304 306166 165 164 163162 161 160 159158 157 156 155329 327 326 325ResearchCommunity-based Programs Social Issues/Public Policy308 309 310 311Multi-Media313 314 315 316324 323 322 321320 319 318 317Prevention/Early InterventionEthics141 143 144 145146 147 148 149150 151 153 154330 331 332 333334 335 336 337339 340 341 342140 138 136 135134 133 132 131130 129 128 126356 355 354 353352 351 350 349348 345 344 343Public Health113 114 115 116112 111 110 109117 118 119 121122 123 124 125108 107 106 105104 103 102 101FireExitsStudent Poster Award FinalistsEntranceFXFXGlobalSTREEENTRA297 – 302Culture/Diversity303 – 306Community-basedProgramsDOWNDOWN308 – 311Thursday Poster DistributionStudent Poster Award Finalists101 – 118Clinical Intervention/ResearchREGISTRATIONREGISTRATION119 – 216Technology217 – blicPolicy222 –ENTRANCE228UPUPENTRANCEAssessment/Diagnosis229 – 255DUMPSTERMulti-Media315EthicsResearch Methodology285 – 293Public HealthLOUNGELOUNGEELEV.MACH. RM.ELEV.MACH. RM.316 – 332FX333EXIT5 Page295 – 296EXITVicarious Traumatization & Therapist Self CareWFWFUNISEX270 – 284UNISEXBiological/MedicalWFFX334 – 356EXITPrevention/Early InterventionWFEXIT256 – 269Clinical PracticeFireExits313 – 314
www.istss.orgCopyright 2016 ISTSS Annual MeetingPoster Session One PresentationsThursday, November 1005:30 PM to 06:30 PMStudent Poster AwardFinalistsTHU 102Resilience as a Predictive Factor of TherapeuticChange(Abstract #1244)THU 101Premature Termination Factors among ChildrenReceiving Trauma-Focused Treatment at a ChildAdvocacy Center(Abstract #73)(Clin Res, Affect/Int, Complex, Civil/War,Child/Adol) M - M East & N Africa(Clin Res, Affect/Int, Chronic, Practice,Complex, Child/Adol) I - IndustrializedGrandHallSteinzor, Cazzie, Wamser-Nanney, RachelUniversity of Missouri St. Louis, St. Louis, Missouri,USATo ultimately prevent attrition, it is critical to identify dropoutfactors in child trauma-focused therapy. As differentdefinitions of attrition may impact findings, weoperationalized attrition as: 1) clinician-rated dropout and2) whether the child received an adequate dose oftreatment (i.e., 12 sessions or more). Four hundred andsixty-six children (ages 2-18; M 9.23, SD 3.78; 66.1%females; 52.8% minority) referred to a Child AdvocacyCenter for trauma-focused therapy were included in thestudy. Demographic variables, trauma eventcharacteristics, and pretreatment symptoms levels wereassessed in relation to clinician-rated dropout and whetherthe child received an adequate dose of treatment. Severaldemographic factors, Child Protective Servicesinvolvement, Cognitive Behavioral Therapy (CBT) versusnon-CBT treatment type, number of traumatic events, andcaregiver-rated pretreatment symptom levels were relatedto clinician-rated dropout. Fewer factors were associatedwith whether an adequate dose of treatment was received.Complex trauma exposure and child-reported pretreatmenttrauma symptoms were unrelated to either attritiondefinition. Demographic factors, number of traumaticevents, and caregiver-reported symptoms may help toidentify children at risk for dropout.6 PageGrandHallJoachim, Brandon1, D'Andrea, Wendy2, Bergholz, Lou3,Freed, Steven21The New School, New York, New York, USA2New School for Social Research, New York, New York,USA3Edgework Consulting, Boston Massachusetts, USAThe study examines the relationship between traitresilience, optimism, and self-reported and peerassessment of positive change following interventionamong two samples of children between the ages of 8 and13 living within the occupied West Bank and Gaza Strip(N 834, 888 respectively). Prior research links traitresilience to a number of positive emotional and behavioraloutcomes following stress. Two samples completed thepreviously validated Brief Resilience Scale (BRS) and theOutlook Questionnaire (OQ) assessing optimism. Scoreson these questionnaires are compared to scores on theYouth Self Report questionnaire, which provides scores forinternal and external maladaptive behavior. Overall scoresof resilience predicts an overall positive change postintervention in the YSR (b .783, t(687) 3.773 , p .001),and correlates with positive change in every YSRsubscale. Overall scores on optimism predict overallchange in YSR scores after intervention (b -.147, t(830) -2.070, p .038) and significantly negatively correlateswith change in withdrawn depression (r (874) .067,p .048), aggression (r (874) .072, p .033), and rulebreaking behavior (r (875) .091, p .007). Data suggeststhe tendency to bounce back after a stressful event may bea more powerful moderating factor of a positive responseto therapy than having a hopeful outlook for the future.Presenting Author is Bolded
www.istss.orgCopyright 2016 ISTSS Annual MeetingTHU 103Role of Coping Self-efficacy on ParasympatheticResponse to an Online Intervention(Abstract #663)(Clin Res, Bio Med, Prevent, Pub Health,Tech, Adult) M - IndustrializedGrandHallDevane, Amanda, Shoji, Kotaro, Boult, Terrance, Benight,CharlesUniversity of Colorado at Colorado Springs, ColoradoSprings, Colorado, USAMy Trauma Recovery is an online intervention consisting ofsix modules (e.g., relaxation, triggers). The current studyevaluated the effect of module order on changes in heartrate variability (ΔHRV), a measure of parasympatheticdominance, moderated by changes in coping self-efficacy(ΔCSE). Thirty-five trauma exposed females completed therelaxation and triggers modules. They were assigned tocomplete the relaxation module then triggers or triggersmodule then relaxation in session 1. The reverse order wasused in session 2. Electrocardiogram was measuredthroughout the sessions. A high frequency power domainwas calculated as an HRV measure, and residual changescores between first and second modules in each sessionwere computed as ΔHRV. Residual change scores werecalculated between baseline CSE and CSE post-session 1as ΔCSE. Results showed that ΔHRV was greater (i.e.,greater relaxation response) as ΔCSE increased (i.e.,improved mastery) when the triggers module wascompleted first in session 1, and ΔHRV remained high insession 2. No such effect was found when the relaxationmodule was completed first in session 1 (partial etasquared .10). This finding suggests that working on thetriggers module first, then relaxation may result in greaterparasympathetic dominance and improved sense of copingcapability.THU 104Emotion Regulation as a Mechanism of Change inGroup-Delivered Unified Protocol for VeteransDiagnosed with PTSD(Abstract #666)(Clin Res, Affect/Int, Clin Res, Practice,Adult) I - IndustrializedGrandHallSherrill, Andrew, Varkovitzky, RuthVA Puget Sound Healthcare System, Tacoma,Washington, USABarlow’s unified protocol (UP) for the transdiagnostictreatment of emotional disorders targets emotion regulation7 Pageas a mechanism of change (Barlow et al., 2011). Emergingevidence indicates favorable outcomes for UP applied to arange of emotional disorders (Ciraulo et al. 2013;Farchione et al., 2012; Lotfi et al., 2014; Mohammadi et al.,2014), including PTSD (Gallagher & Barlow, 2015;Varkovitzky & Reger, 2015). UP may be well-suited fortrauma-related pathology due to the association betweenemotion dysregulation and PTSD symptoms (Boden et al.,2012; Bonn-Miller et al., 2011; Ehring & Quack, 2010;Moore et al., 2008; Tull et al., 2007). However, research isneeded to examine if UP treatment gains are due tochanges in emotion regulation. The current studyexamined the role of emotion regulation within a groupdelivered, 16-week UP program offered at a large VeteransAffairs hospital using a sample of 48 mixed-genderedmilitary veterans diagnosed with PTSD andcomorbidities. Consistent with predictions, results suggestimprovements in emotion regulation during treatment(Difficulties in Emotion Regulation Scale; Gratz & Roemer,2004) negatively predict posttreatment PTSD symptomswhile controlling for pretreatment PTSD symptoms (PTSDChecklist for DSM-5; Weathers et al., 2013). Clinicalimplications and future research directions will bediscussed.THU 105Reconsolidation Blockade (RB) for the Treatment ofTorture Survivors: A Randomized Control Trial in Nepal(Abstract #664)(Clin Res, Cul Div, Global, Civil/War, Adult) GrandM - S AsiaHallDescamps, Melanie1, Kienzler, Hanna2, Sharma,Bhogendra3, Sapkota, Ram P.2, Pedersen, Duncan1,Brunet, Alain41Douglas Mental Health University ResearchInstitute/McGill University, Montreal, Quebec, Canada2McGill University, Montreal, Quebec, Canada3Center for Victims of Torture, Kathmandu ,Kathmandu, Nepal4McGill University, Douglas Mental Health UniversityInstitute, Montreal, Quebec, CanadaMost traumas occur in low- and middle-income countries(LMICs) where mental health resources are scarce.Although pharmacotherapy is recommended to treat thesymptoms of posttraumatic stress disorder (PTSD), sideeffects lead patients to abandon their treatment.Psychotherapy is effective for PTSD but requires qualifiedpersonnel, is fairly slow and may be culture-bound. Theaim of this study was to explore the feasibility, socialacceptability and efficacy of reconsolidation blockade (RB)to treat PTSD symptoms in Nepalese torture survivors. Inthis pilot clinical trial, participants were randomized for a13-week treatment either to RB group (n 23) or to thePresenting Author is Bolded
www.istss.orgCopyright 2016 ISTSS Annual MeetingParoxetine group (n 20). There was a main effect oftreatment whereby both groups improved equally: 78%(reconsolidation group) and 80% (paroxetine group) of Sswere rated (blindly) as ‘much improved’ or better at week13th according to the CGI. Results suggest a significantimprovement over all outcome measures for both groups:PTSD symptom severity (PCL-S), F(1.6, 82) 258; selfreported distress (SCL-25), F(2, 82) 351; and disability(WHODAS), F(1.8, 82) 153. RB appears to be anattractive alternative to the classic pharmacologicaltreatment of PTSD in LMICs. A larger clinical trial would benecessary.THU 106Use of the AUDIT Screener in a Trauma-ExposedSample: Comparing the Predictive Value of Phone andComputer Administration Techniques(Abstract #580)(Clin Res, Assess Dx, Sub/Abuse, Adult) I - GrandIndustrializedHallDutton, Courtney1, Bujarski, Sarah2, Lang, Katelyn1,Bermudez, Andrea1, Timmerman, Jesse1, Feldner, Matthew11University of Arkansas, Fayetteville, Arkansas, USA2VA, Omaha, Nebraska, USAPosttraumatic stress disorder (PTSD) and alcohol usedisorders (AUD) frequently co-occur, and the presence ofboth has been linked to greater impairment and poorertreatment outcomes. Screening individuals with PTSD foran AUD is recommended practice, and the Alcohol UseDisorders Identification Test (AUDIT) is commonly utilized.Different administration methods may impact disclosure onthe AUDIT, and it is important to assess which screeningmethod is best at predicting AUDs for those with PTSD. Inthe current study, the AUDIT was administered both via thephone and computer prior to the administration of the MINIto assess psychopathology, including current AUDs.A logistic regression analysis was used to predict thepresence of a current AUD using the AUDIT screenerconducted over the phone and computer. The CAPS totalscore was used to control for PTSD symptom severity. TheWald criterion indicated that only the AUDIT screeneradministered via the computer was a significant predictor ofa current AUD (b .466, SE .161, Wald 8.41, p .004).Neither the AUDIT phone screener, nor PTSD symptomswere significant predictors of a current AUD. Indeed, foreach point the computerized AUDIT score increased,individuals were 1.5 times more likely to meet criteria for anAUD. The important clinical implications of these findingswill be discussed.8 PageTHU 107Prevalence and Correlates of Sexual Dysfunctionamong Male and Female Veterans who HaveExperienced Military Sexual Trauma(Abstract #1173)(Train/Ed/Dis, Clin Res, Health, Rape,Gender, Adult) I - IndustrializedGrandHallDetweiler, Laura1, Garneau-Fournier, Jade1, McBain,Sacha1, Torres, Tammy2, Turchik, Jessica31Pacific Graduate School of Psychology at Palo AltoUniversity, Palo Alto, California, USA2Pacific Graduate School of Psychology-StanfordPsy.D. Consortium, Palo Alto, California, USA3Center for Innovation to Implementation & NationalCenter for PTSD, VA Palo Alto Health CareSystem/Stanford University, Menlo Park, California,USAPrevious research has found that American veterans whohave experienced military sexual trauma (MST) are atincreased risk for sexual dysfunction (SD). The goal of thecurrent research was to further explore the impact ofdemographics, physical health factors, mental healthfactors, and sexual trauma history on the presence of SD ina nationwide sample of veterans who had experiencedMST. A sample of 362 mixed-era veterans, 129 men and233 women, enrolled in Veterans’ Health Administration(VHA) care were mailed a survey assessing for a numberof physical health, mental health, and sexual traumarelated factors. Results revealed that 73.3% of men and73.7% of women reported at least one type of SD. Twohierarchical binomial logistic regressions were run bygender. Analyses revealed that antidepressant use was asignificant correlate of SD in men (p .008), whereas beingmarried/in a committed relationship (p .002) andincreased PTSD symptoms (p .004) were correlatesamong women. Given the reported high rates of SD, it isimportant that psychoeducation andpsychopharmacological training be considered in order topromote sexual health and prolong sexual vitality amongveteran populations, both young and old. It isrecommended that healthcare provider education andveteran sexual health screening, assessment, education,and interventions be considered within the VHA.THU 108Associations between Pain, Morphine Use, andPosttraumatic Stress after Pediatric Injury(Abstract #430)(Assess Dx, Acc/Inj, Child/Adol) I IndustrializedPresenting Author is BoldedGrandHall
www.istss.orgCopyright 2016 ISTSS Annual MeetingHildenbrand, Aimee1, Kassam-Adams, Nancy2, Barakat,Lamia3, Kohser, Kristen3, Marsac, Meghan21Drexel University, Philadelphia, Pennsylvania, USA2University of Pennsylvania School of Medicine,Philadelphia, Pennsylvania, USA3Children's Hospital of Philadelphia, Philadelphia,Pennsylvania, USAAfter injury, many children experience posttraumatic stresssymptoms (PTSS) that negatively impact recovery. Acutepain and PTSS share neurobiological pathways, and acutedosage of morphine has been linked to reduced PTSS innaturalistic studies. However, the complex interactionsbetween pain, morphine use, and PTSS have yet to beinvestigated in robust pediatric samples. This studyexamined relationships between peri-trauma pain,morphine use, and subsequent PTSS after pediatric injury.Children ages 8-17 years hospitalized for unintentionalinjury (N 101) completed assessments at baseline (T1)and 6 (T2) and 12 weeks (T3) later. Pain ratings andmorphine administration were obtained via chart review.Worst pain during hospitalization (M 7.60 2.41) wasassociated with T1 and T3 PTSS (r .25-.28, p .02).Hierarchical regressions revealed that worst pain was asignificant independent predictor of T3 PTSS (R2 .045,p .045), even when controlling for other risk factors (i.e.,age, sex, trauma history, perceived life threat, heart rate,T1 PTSS). Morphine dosage (mg/kg/day) was notsignificantly related to PTSS at any time point and did notmoderate the relationship between pain and T3 PTSS.Findings suggest that pain during hospitalization mayincrease susceptibility for concurrent and later PTSS,above and beyond the influence of other empirical riskfactors.THU 109Examining the Relationships among InterpersonalViolence, Re-experiencing Symptoms, and Self-injuryin a Sample of Incarcerated Women(Abstract #14)(Practice, Chronic, Health, Social, Gender,Adult) I - N/AGrandHallKaplan, Stephanie, DeCou, Christopher, Cole, Trevor,Lynch, ShannonIdaho State University, Pocatello, Idaho, USAIncarcerated women report high rates of interpersonalviolence (IPV), posttraumatic stress disorder (PTSD), andnon-suicidal self-injury (NSSI). Research has suggestedthat IPV is a robust predictor of NSSI; and work withcommunity samples found re-experiencing symptoms ofPTSD significantly mediates the relationship between IPVand NSSI. The current study sought to elucidate therelationship between IPV, re-experiencing symptoms, and9 PageNSSI in a sample of incarcerated women. Participantswere 203 treatment seeking female offenders whocompleted self-report measures of IPV, PTSD, and NSSI.Women reported extensive histories of violence, traumasymptoms, and self-injurious behavior. Regression modelswere used to examine the indirect effect of PTSDsymptoms upon the association between IPV and NSSI. Inthe first model IPV significantly predicted re-experiencingsymptoms (β 1.25, p .001). In the second regressionmodel, re-experiencing (β .09, p .05) but not IPV (β .03,p .81) significantly predicted NSSI severity. Thus, reexperiencing symptoms of PTSD fully mediated therelationship between IPV and NSSI severity. The mediatedeffect was statistically significant, as reflected by theasymmetric confidence interval (95% ACI .01 to .28).These findings suggest that trauma symptoms may be apotential point of intervention among women in prison whoreport self-injurious behaviors.THU 110Intranasal Oxytocin Administration Improves NeuralSensitivity for Social Reward in Patients with PTSD(Abstract #830)(Bio Med, Affect/Int, Bio/Int, Neuro, Police)M - IndustrializedGrandHallNawijn, Laura1, van Zuiden, Mirjam1, Koch, Saskia1,Frijling, Jessie1, Veltman, Dick2, Olff, Miranda31Academic Medical Center, University of Amsterdam,Amsterdam, Noord Holland, The Netherlands2VU University, Amsterdam, Noord Holland, TheNetherlands3Academic Medical Center at the University ofAmsterdam and Arq Psychotrauma Expert Group,Amsterdam, Noord-Holland, The NetherlandsAbout 30% of patients with PTSD do not respond totreatment. Therefore, available treatments need to beimproved. Intranasal oxytocin is a promising candidate formedication-enhanced psychotherapy (MEP), as it is knownto increase sensitivity for social reward. This couldenhance therapeutic alliance and perceived social support,two determinants of treatment response. To explore thepotential of intranasal oxytocin, we conducted arandomized placebo-controlled fMRI study in PTSDpatients (n 35) and trauma-exposed controls (n 37). Weinvestigated the effects of oxytocin administration (40IU) onneural sensitivity to social reward and punishment using asocial incentive delay task. Under placebo, PTSD patientshad significantly lower anterior insula responses to socialreward and higher anterior insula responses to socialpunishment compared to controls. Oxytocin administrationnormalized aberrant insula responses, such that underoxytocin PTSD patients no longer significantly differed fromcontrols under placebo. This suggests that oxytocin hasPresenting Author is Bolded
www.istss.orgCopyright 2016 ISTSS Annual Meetingbeneficial effects on social reward and punishmentsensitivity in PTSD. As a result, oxytocin may increaseperceived social support and therapeutic alliance, therebypotentially enhan
32nd Annual Meeting Trauma and Public Health: Innovative Technology and Knowledge Dissemination November 10 - 12, 2016 Pre-Meeting Institutes, November 9