Transcription
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.MUCOSAL IMMUNITYLEARNING GOALYou will be able to describe the mucosal immune system.OBJECTIVESTo attain the goal for this lecture you will be able to: Describe the components of the mucosal immune system.Draw the structure of secretory IgA.Explain the mechanism of IgA transport across mucosal surfaces.Explain how a response to antigen is generated in the mucosal system.Identify the differences in tolerogenic versus immunogenic responses to mucosalantigen administration.Delineate the functions of the mucosal immune system, including M cells.Describe how the mucosal immune system might be used for immunization.Describe the characteristics of selective IgA deficiency.Describe how intestinal commensal bacteria interact with the host to promote ahealthy environmentREADING ASSIGNMENTJaneway’s Immunobiology 8th Edition (2012), Chapter 12 and Article “Mucosal Immunity andVaccines” by Robyn Seipp attached at end of lecture notes.LECTURERKatherine L. Knight, Ph.D.Page 1
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.CONTENT SUMMARYI. INTRODUCTION TO MUCOSAL IMMUNITYII. ORGANIZATION OF THE MUCOSAL IMMUNE SYSTEMA.B.C.D.Components of the Mucosal Immune SystemInduction of a ResponseFeatures of Mucosal ImmunityIntraepithelial lymphocytes (IEL)III. IgA SYNTHESIS, STRUCTURE AND TRANSPORTIV. FUNCTIONS OF IgA AT MUCOSAL SURFACESA. Barrier FunctionsB. Intraepithelial Viral NeutralizationC. Excretory ImmunityD. Passive ImmunityE. IgA Deficiency StateV. MUCOSAL IMMUNIZATIONVI. MUCOSAL TOLERANCEA. The Induction of Tolerance via Mucosal SitesB. The interaction Between Gut Bacteria and the IntestineI. INTRODUCTION TO MUCOSAL IMMUNITYMucosal surfaces are continually exposed to external infectious agents, and consequently,immunologic defense against pathogens is paramount at these surfaces. Specific immunologicdefense at mucosal surfaces is mediated by a specialized arm of the immune system that istermed the mucosal immune system. The mucosal immune system includes lymphoid tissuesof the gastrointestinal tract, respiratory tract, salivary glands, lacrimal glands, mammaryglands, and genito-urinary tract. The mucosal, or secretory, branch of the immune system isquite extensive, as the mucosal surfaces of the human body represent an area 100 times greaterthat of the skin. The importance of this system is underscored by the fact that 70 to 80% of allimmunoglobulin producing cells in the body are physically located within the tissues of themucosal immune system. Worldwide, over 12 million (1.2 x 107) deaths result from mucosalPage 2
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.infections.Mucosal tissues are exposed to a large number of both potentially harmful and benign antigensfrom the environment, food, and microorganisms. For example, the intestine is host tohundreds/thousands of different bacteria. The mucosal immune system must thereforecontinually control responsiveness and unresponsiveness. Unlike many other components ofthe immune system, our understanding of the regulation of mucosal immunity remainssomewhat incomplete.II. ORGANIZATION OF THE MUCOSAL IMMUNE SYSTEMA. Components of the Mucosal Immune SystemMucosal immunity is triggered by the coordinated interaction of multiple cell types withinthe mucosal tissues. The process involves the initiation of the response at an inductive site,leading to an immune response at multiple effector sites.Components of the mucosal immune system (MALT) include: Gastrointestinal tract – gut associated lymphoid tissue (GALT); includes tonsiland appendix Respiratory tract – bronchial associated lymphoid tissue (BALT) Nasal associated lymphoid tissue (NALT) Genitourinary tract Lacrimal glands Salivary glands Mammary glandsCells of the mucosal immune system are located in anatomically defined compartments (e.g.,Peyer’s patches and isolated lymphoid follicles) as well as throughout mucosal tissues.Page 3
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.B. Induction of a ResponseThe inductive process has been best described for the GALT, which can be used as aprototype to explain the generation of mucosal immunity. Another inductive site that isgaining attention is the NALT, as inductive sites that are similar to those found in the GItract are also present in nasal mucosa. Evidence for induction through BALT is alsoavailable.Lymphocytes reside in defined compartment of MALT (GALT is best defined example).Mechanistically, the induction process can be divided into the following steps: Antigens entering the digestive tract can be taken upPage 4
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.- By nonspecific transport across the epithelium or by specialized mucosal cells calledM cells which internalize the antigen and transport it across the epithelium whereantigen can be taken up by APCs such as dendritic cells (DC).- By FcRn transport of Ag/Ab complexes- By apoptosis of infected enterocytes- By DC that have dendrites extending through the epithelial tight junction into thelumen Antigens are then presented to lymphocytes (in the intestine, these are located in Peyer’spatches). Lymphocytes (both B and T cells) leave the mucosal site and travel to the mesenteric lymphnodes, then into the lymph.Page 5
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D. Via the thoracic duct, the lymphocytes exit the lymph and enter the circulation. Circulating lymphocytes “home” to positions within the mucosal lamina propria throughoutthe body, including sites distant from the original antigenic encounter. The homing oflymphocytes to mucosal sites involves specific interactions of both adhesion molecules andchemokines. B Lymphocytes within the peripheral tissues proliferate and differentiate into IgA secretingplasma cells at effector sites.C. Features of Mucosal Immunity1. The administration of antigen at one mucosal site results in specific antibody production atdistant mucosal sites. Some regional preference seems to occur, however. For example,induction via NALT leads to a more robust response in the respiratory sites than ingastrointestinal sites.2. B cells in the mucosa are selectively induced to produce dimeric IgA rather than otherisotypes. The selective switch of B cells to IgA is believed to be mediated by specificcytokines produced by T cells in the inductive sites.3. Conventional T cells, particularly CTLs, are also an important component of the mucosalimmune response. The induction and homing requirements for these cells are not as welldescribed as those for mucosal B cells.Page 6
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.4. Induction of a response via a mucosal site generally elicits a systemic immune response aswell, such that serum antibodies can be detected. This indicates that a mucosal encounter withantigen generates subsets of T and B cells that home to mucosal sites and also to spleen andregional nodes.D. Intraepithelial Lymphocytes (IEL)A distinct population of lymphocytes, mostly CD8 T cells are found in the gut epithelium.There are 10-15 IEL for every 100 epithelial cells and because the mucosa has a huge surfacearea, IELs are one of the largest population of lymphocytes in the body. The function ofthese cells is still not clear but they may readily kill infected epithelial cells.III. IgA SYNTHESIS, STRUCTURE AND TRANSPORTThe predominant immunoglobulin in mucosal secretions is IgA.Serum Ig – 12% IgA class, primarily monomericSecreted Ig at mucosal sites – 96% IgA, primarily dimericIgA in mucous secretions is called secretory IgA, or sIgA.The production of secretory IgA (sIgA) requires both plasma cells in the lamina propria andepithelial cells of the mucosa. Dimeric IgA (2 monomeric IgA units covalently joined a J chain) is produced by plasma cellswithin the mucosal lamina propria. Dimeric IgA binds to the polymeric immunoglobulin receptor (pIgR) on the basal surface ofmucosal epithelial cells. The IgA-pIgR complex is endocytosed and transported through the epithelial cell to thelumenal surface for release.Page 7
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D. During this transport, the pIgR is cleaved and a small fragment is lost. The remaining large component, secretory component, is covalently bound to the dimericIgA. IgA is secreted at the mucosal surface as dimeric IgA covalently bound to secretorycomponent. Secretory IgA production requires two different cell types. Only polymeric immunoglobulins (dimeric IgA or pentameric IgM) are capable of bindingand being transported by pIgR. Mice that are genetically deficient for pIgR exhibit the expected decreases in IgA transport.PIgR deficiency also leads to an increased mucosal leakiness.IV. FUNCTIONS OF IgA AT MUCOSAL SURFACESPage 8
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.A. Barrier FunctionsSecretory IgA can bind to bacteria and viruses and prevent their adherence and invasion intomucosal tissues. Secretory IgA can neutralize many viruses in this way, including polio,herpesvirus, coxsackie virus, and rotaviruses. Secretory IgA can also neutralize bacterialtoxins at mucosal surfacesB. Intraepithelial Viral NeutralizationIgA that is internalized by mucosal epithelial cells (via the pIgR) may contribute tointracellular viral inactivation.C. Excretory ImmunityViral particles that complex with dimeric IgA in the lamina propria may be endocytosed andtransported out by the pIgR pathway.D. Passive ImmunitysIgA in breast milk provides passive immunity to the infant.E. IgA DeficiencySelective IgA deficiency is the most common primary immune deficiency, with an estimatedincidence of 1 per every 500 to 1000 persons. The precise characteristics of the deficiencyare variable, as some patients have complete IgA deficiency but others have decreased butdetectable levels of IgA.Patients present with low or no levels of serum IgA, but have normal cell mediated immunityand serum antibody responses. Not all patients exhibit increased susceptibility to infection.Reasons to suspect selective IgA deficiency include 1) a family history of IgA deficiency ofagammaglobulinemia, 2) a high incidence of oral infections, 3) frequent respiratoryinfections, and 4) chronic diarrhea.Autoimmune diseases, including SLE, juvenile rheumatoid arthritis, and thyroiditis, are oftenassociated with selective IgA deficiency. Immunoglobulin therapy is generally notindicated, as the patient’s normal antibody response can produce anti-IgA antibody inresponse to IgA treatment. People with a complete absence of IgA may develop allergies oreven anaphylactic shock if given gammaglobulin.Page 9
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.V. MUCOSAL IMMUNIZATIONMucosal surfaces are portals of entry for many pathogens (e.g. cholera, HIV, influenza).The development of immunization strategies that would produce a robust mucosal immuneresponse is a high priority.When compared to systemic immunization by intramuscular, intraperitoneal, or intradermalroutes, immunization with mucosally administered antigens has both advantages anddisadvantages.ORAL IMMUNIZATIONAdvantages Ease of administration (oral) Generates both mucosal and systemicimmunityDisadvantages Difficulty in eliciting robust response Response may not be long-lastingAn example of an effective oral immunization is the polio vaccine. Effective nasal sprayvaccines for influenza have recently been developed.New strategies for oral immunization include the use of cholera toxin chimeric molecules aswell as recombinant avirulent bacteria (e.g. avirulent salmonella expressing S. pneumoniaeproteins). Can also target M cells using bacteria and viruses that preferentially bind M cellsor antigen encased in biodegradable particles such as latex. These strategies attempt toboost the uptake of foreign antigen at mucosal induction sites.VI. MUCOSAL TOLERANCEA. The Induction of Tolerance via Mucosal Sites The mucosa is exposed to many environmental antigens such as food that are notinfectious. To operate in an effective manner, the mucosal immune system mustdistinguish between pathogenic antigens, which require a response, and non-dangerousantigens, such as those in food and in the commensal bacteria that make the gut theirhome. The response to most antigens is tolerance, and the type of antigen is critical toeliciting the appropriate response. The key feature that appears to distinguish between theinduction of a response and the induction of tolerance is inflammation. Antigen encountersthat occur alongside inflammation generally illicit an immune response. Antigenencounterd in the absence of inflammation generally induces tolerance. Thus: Food antigens generally induce tolerance.Page 10
Host Defense 2013April 16, 2013 Mucosal ImmunityKatherine L.Knight, Ph.D. Microbes (bacteria and viruses) that cause inflammation generally evoke amucosal immune response. Peptides generally induce tolerance, unless attached to a mucosal adjuvant, suchas cholera toxin. Tolerance can occur by anergy (unresponsiveness) or regulatory T cells (Treg)The induction of tolerance might be exploited therapeutically in autoimmune diseases, or tolimit transplant rejection.B. Interaction Between Gut Bacteria and the Intestine Commensal bacterial species coinhabit the gut; 10X more bacterial cells than human cells The mechanism by which the mucosal administration of some antigens induces tolerance,rather than immunity, is incompletely understood. Recent studies suggest that mucosaltolerance is mediated by mucosal dendritic cells.Page 11
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D. Regulatory T cells are a prominent feature at mucosal sites, and may synergize withsuppressive dendritic cells. Regulatory populations have been isolated from draining lymphnodes of mucosal sites.Page 12
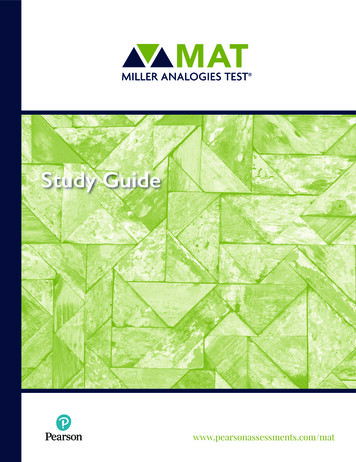
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.MUCOSAL IMMUNITY AND VACCINESBy Robyn SeippThe mucous membranes are one of the largest organs of the body (Figure 1).Collectively, they cover a surface area of more than 400m2 (equivalent to one and ahalf tennis courts) and comprise the linings of the gastrointestinal, urogenital andrespiratory tracts [15,18].Figure 1: Schematic diagram of the mucous membranes of the body and surfaceswith which they are in contact.These mucosal surfaces, while located inside the body, are actually a physicalbarrier between the outside and the sterile interior cavity of the body known as the“systemic” environment. Critical nutrients, oxygen and other molecules areconstantly taken up across these mucosal barriers; however, another importantfunction of the mucous is to keep invading pathogens out [15]. Daily these mucousmembranes are bombarded by outside elements and it is up to the unique immunesystem of the mucous to determine what is potentially harmful and what is beneficial[15,18].Why mucus mattersInterest in mucosal tissues stems from their importance in immunity, with the vastmajority of human pathogens initiating infections at mucosal surfaces, making thegastrointestinal, urogenital and respiratory tracts major routes of entry into the body[14,18]. In fact, virtually the only way to contract an infection other than mucosally isthrough blood-borne routes such as injections, transfusions and bites. Examples ofmucosally-infecting agents include cold viruses, influenza, food poisoning agents,tuberculosis, sexually transmitted diseases, cholera, diphtheria and plague [15].Despite its important role, only a handful of vaccines specifically target this area ofPage 13
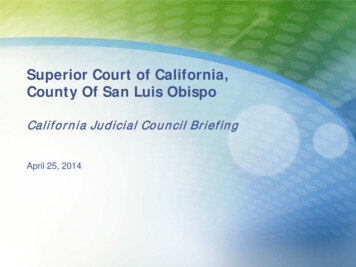
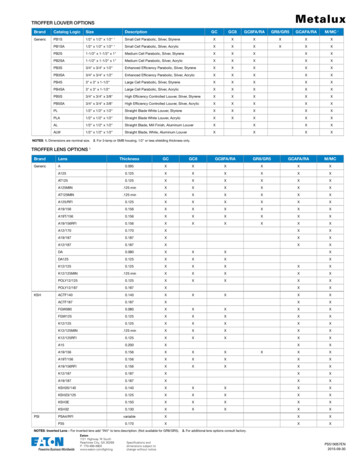
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.the immune system despite strong evidence that a good mucosal response caneffectively prevent systemic infections [15].Components of a mucosal immune responseThe systemic and mucosal immune systems have an arsenal of moleculesspecifically designed to eliminate invading pathogens. One of the first lines ofdefense are antibodies, made and secreted by plasma B cells. Antibodies are largeprotein molecules capable of binding and neutralizing an invading organism7. Apicture of a typical antibody is shown in Figure 2.Figure 2: Schematic diagram of the prototypical IgG antibody. It shows the twoantigen binding sites of the variable regions of light and heavy chains. The constantregion determines the type of antibody and its effector function. It is composed ofheavy chains only.The mucous membranes produce a special type of antibody called secretory IgA orsIgA. In the mucous, this antibody is secreted as a dimer, joined at the non-antigenbinding end by a protein known as the J chain as shown in Figure 3.Figure 3. Structure of secretory IgA. It consists of at least two IgA moleculescovalently linked by a J chain and the secretory component, which is added as theantibody crossed the mucosal epithelial cells into the lumen.This form of the antibody is more stable, less resistant to proteolysis by the digestiveenzymes of the gut, and has higher avidity for mucosal surfaces [13,15,18]. Themucous membranes are bathed in huge quantities of sIgA, which act as a first line ofPage 14
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.defense to neutralize invading pathogens [15,15]. Experimental evidence shows thatthe presence of sIgA correlates with resistance to infection by various pathogens,including bacteria, viruses, parasites and fungi [13,15,18]. It has also been shown toneutralize viruses and prevent their adherence to the epithelial cells lining themucous (thereby preventing infection) as well as mediating excretion of pathogensand preventing the assembly of mature virus particles [13,15,18,21].Another important component of mucosal immunity is the T cell-mediated immuneresponse. T cells that specifically recognize pathogens can help antibodies to clearthe infection or directly kill the invader themselves. T cells produced in the mucousare capable of traveling throughout the mucosal tissues through special “homing”receptors on their membranes [13,15,18]. This means that if an immune response isgenerated in the gastrointestinal lining, T cells produced there can travel to othermucosal sites, for example, the lungs or nasal cavity, providing protection over alarge surface area [13,15,21].The importance of mucosal immunology lies in the interplay between the mucosalresponse and the systemic immune response. Several studies have demonstratedthat stimulating the immune system systemically (i.e. via injection or blood-borneroutes) results in production of protective antibody and T cells only within the sterile,internal environment of the body—no mucosal response is generated. On the otherhand, stimulation of the mucosal immune response can result in production ofprotective B and T cells in both mucosal and systemic environments so thatinfections are stopped before they get into the body [13,15,18].Mucosal vaccinationsThe goal of current mucosal vaccination strategies is to prevent both initial stages ofdisease (colonization and infection by pathogens) and block its development [14].Currently, the vast majority of vaccines available only block disease developmentonce the pathogen has crossed the mucosal barrier into the normally sterilesystemic environment [13]. Mucosal vaccines have several advantages overtraditional systemic vaccines. They can be administered orally or nasally rather thanvia injection. This is more widely accepted by the public, as well as making thevaccine simpler to administer and distribute. In addition, there is less risk of needlestick injury or cross-contamination [13,15,18]. Inoculation could be accomplishedusing recombinant bacteria to express pieces of proteins from the pathogen (knownas antigens) that the immune system will respond to and “remember” for the nextinfection. Another possibility is the creation of transgenic plants expressing pathogenantigens that could be eaten to administer the vaccine. Certain types of transgenicplants such as banana trees and potatoes have also been modified to overexpressprotein antigens from pathogens such as hepatitis B and rotavirus; however, to datethe level of protein expressed in the plant is variable and often too low for effectiveimmunization [13,14,15].Page 15
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.Spotlight on a mucosal AIDS vaccineStudies of populations with high incidences of HIV infection have shed some light onpossible approaches to the development of an effective vaccine. Analysis of severalgroups of HIV-exposed individuals has consistently revealed the existence of a smallsubgroup that is resistant to infection despite multiple, long-term exposures [11,12].In about 30% of cases it appears to be the presence of high levels of HIVneutralizing sIgA in the genital tract and HIV-reactive T cells in the cervix thatconfers resistance to infection [10-12]. Because 70-80% of people contract thedisease mucosally, and because the gut is the major reservoir for HIV replication,there is interest in the potential of the mucosal immune response in preventingand/or clearing infection [2,10]. Among the newer vaccines designed to induce aprotective immune response to HIV is one designed to mimic the mucosalresponses seen in these resistant individuals [2]. In 2001, a US group tested the firstmucosal HIV vaccine in rhesus macaques [2]. While the vaccine showed promisingresults, it failed to prevent infection.AutoimmunityAutoimmunity occurs when the immune system begins attacking “self” componentsof the body aberrantly. The reasons why this occurs remain largely unknown, but theconsequences can be devastating as parts of the body are slowly destroyed by thevery system designed to protect them. Examples of autoimmune diseases includemultiple sclerosis, rheumatoid arthritis, lupus and type I diabetes [15]. Mucosalimmunity offers some possibilities for alleviating or reversing symptoms ofautoimmune diseases. The basis of treatment involves a phenomenon known asmucosal tolerance. In the 1940’s, M.W. Chase noticed that repeated feeding of asubstance to mice reduced their immune response when the same substance wasinjected systemically [15]. His experiment is outlined in Figure 4.Figure 4. Chase’s experiment that demonstrated mucosal tolerance. a) Injection ofpicryl chloride into mice led to a strong systemic immune response. b) When micePage 16
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.were first fed picryl chloride for several weeks, then injected with picryl chloride, asignificant loss in the systemic immune response was observed.This phenomenon, known as mucosal tolerance, has been demonstrated not onlywith picryl chloride, but also with heavy metals, proteins, blood cells, mites,inactivated viruses, bacteria and many other substances [15]. The exactmechanisms of how the body adapts its immune response in this way are still notwell understood [15]. Nevertheless it is believed to be a normal body function toprevent hypersensitivity to food proteins, normal bacterial flora that inhabit thegastrointestinal tracts and other mucosal surfaces of healthy individuals, and otherenvironmental macromolecules [15].Mucosal tolerance is being exploited for the development of autoimmune diseasetherapies. Because autoimmunity is caused by the immune system reacting to “self”antigens, the theory is that administration of the self antigen to which the body isaberrantly reacting by oral or nasal routes could induce mucosal tolerance and thuslower the harmful systemic immune response [15]. For example, in multiple sclerosis(MS), myelin (a fatty substance surrounding nerve cells) is slowly degraded by theimmune system, resulting in gradual loss of nerve function (see Figure 5 andhttp://www.mssociety.ca/).Figure 5. Electron micrograph of a cross-section of a nerve cell showing the myelinsheath.Mice suffering from EAE (acute experimental autoimmune encephalomegalitis) havevery similar symptoms and are used as experimental models for human MS. Myelindeterioration was suppressed in these mice by oral or nasal administration of veryhigh doses of MBP (myelin basic protein) [6,9,15]. Clinical trials in humans usingbovine MBP have had controversial results: MBP reappeared on nerves of patientsin a pilot study but with a larger group the positive observations of the initial studyfailed to be confirmed [6,9,15].ImmunocontraceptivesPage 17
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.The idea of harnessing the immune response to control fertility was first proposed inthe 1930’s [3]. However, only recently has our comprehension of the immunesystem progressed to the level where the idea may finally be put into practice. Overthe past 30 years, the World Health Organization Task Force on Vaccines forFertility Regulation has supported basic and clinical research on the development ofbirth control “vaccines” [8]. Studies have shown that approximately 30% of humaninfertility is associated with the presence of anti-sperm antibodies in mucoussecretions of men and/or women and sperm-reactive T cells in men only [3,16].These individuals show no other health problems other than immune-mediatedinfertility: therefore, inducing an immune response against critical components ofreproduction might be a safe and effective way to control conception [3,16].One approach being considered is the design of a “vaccine” capable of inducing animmune response against sperm antigens in either partner. Immunization of themale partner would result in inviable sperm production, while immunization of thefemale partner would result in reduced sperm motility or neutralization in the cervixand/or impaired penetration of sperm into the oocyte [3]. Another target forimmunocontraceptive vaccines are reproductive hormones such as folliclestimulating hormone and human gonadotropin. Interfering with the functioning ofthese hormones can also reduce fertility.References and Additional Reading1) Barber B. Introduction: Emerging vaccine strategies. Sem. Immunol. 1997 9: 269270.2) Belyakov IM, Hel Z, Kelsall B, Kuznetsov VA, Ahlers JD, Nacsa J, Watkins DI,Allen TM, Sette A, Altman J, Woodward R, Markham PD, Clements JD, Franchini G,Strober W, Berzofsky JA. Mucosal AIDS vaccine reduces disease and viral load ingut reservoir and blood after mucosal infection of macaques. Nat Med. 2001Dec;7(12):1320-6.3) Delves PJ, Lund T, Roitt IM. Antifertility vaccines. Trends Immunol. 2002Apr;23(4):213-9. Review.4) Delves PJ, Lund T, Roitt IM. Future prospects for vaccines to controlfertility.Trends Immunol. 2002 Apr;23(4):220-1.5) Fujihashi K, Koga T, van Ginkel FW, Hagiwara Y, McGhee JR. A dilemma formucosal vaccination: efficacy versus toxicity using enterotoxin-basedadjuvants.Vaccine. 2002 Jun 7;20(19-20):2431-8. Review.6) Fukaura H, Kent SC, Pietrusewicz MJ, Khoury SJ, Weiner HL, Hafler DA.Induction of circulating myelin basic protein and proteolipid protein-specifictransforming growth factor-beta1-secreting Th3 T cells by oral administration ofmyelin in multiple sclerosis patients. J Clin Invest. 1996 Jul 1;98(1):70-7.7) Goldsby RA, Kindt TJ and Osborne BA. “Kuby Immunology” 4th ed. W.H.Freeman & Co: New York. 2000.8) Griffin PD. The WHO Task Force on Vaccines for Fertility Regulation. Itsformation, objectives and research activities. Hum Reprod. 1991 Jan;6(1):166-72.Review.Page 18
Host Defense 2013April 16, 2013Mucosal ImmunityKatherine L.Knight, Ph.D.9) Hafler DA, Kent SC, Pietrusewicz MJ, Khoury SJ, Weiner HL, Fukaura H. Oraladministration of myelin induces antigen-specific TGF-beta 1 secreting T cells inpatients with multiple sclerosis. Ann N Y Acad Sci. 1997 Dec 19;835:120-31.10) Kaul R, Plummer FA, Kimani J, Dong T, Kiama P, Rostron T, Njagi E,MacDonald KS, Bwayo JJ, McMichael AJ, Rowland-Jones SL. HIV-1-specificmucosal CD8 lymphocyte responses in the cervix of HIV-1-resistant prostitutes inNairobi. J Immunol. 2000 Feb 1;164(3):1602-11.11) Kaul R, Trabattoni D, Bwayo JJ, Arienti D, Zagliani A, Mwangi FM, Kariuki C,Ngugi EN, MacDonald KS, Ball TB, Clerici M, Plummer FA.HIV-1-specific mucosalIgA in a cohort of HIV-1-resistant Kenyan sex workers. AIDS. 1999 Jan 14;13(1):239.12) Mazzoli S, Lopalco L, Salvi A, Trabattoni D, Lo Caputo S, Semplici F, Biasin M,Bl C, Cosma A, Pastori C, Meacci F, Mazzotta F, Villa ML, Siccardi AG, ClericiM.Human immunodeficiency virus (HIV)-specific IgA and HIV neutralizing activity inthe serum of exposed seronegative partners of HIV-seropositive persons. J InfectDis. 1999 Sep;180(3):871-5.13) McCluskie MJ, Davis HL. Mucosal immunization with DNA vaccines. MicrobesInfect. 1999 Jul;1(9):685-98. Review.14) Medina E, Guzman CA. Modulation of immune responses following antigenadministration by mucosal route. FEMS Immunol Med Microbiol. 2000Apr;27(4):305-11. Review.15) Ogra PL, Faden H, Welliver RC.Vaccination strategies for mucosal immuneresponses. Clin Microbiol Rev. 2001 Apr;14(2):430-45. Review.16) Rajalakshmi M, Griffin PD. Male Contraception: present and future. New AgeInternational (P) Ltd: New Delhi. 1999. pp.309-32817) Raychaudhuri S, Rock KL. Fully mobilizing host defense: building bettervaccines.Nat Biotechnol. 1998 Nov;16(11):1025-31. Review.18) Rosenthal KL, Gallichan WS Challenges for vaccination against sexuallytransmitted diseases: induction and long-term maintenance of mucosal immuneresponses in the female genital tract. Semin Immunol. 1997 Oct;9(5):303-14.Review.19) Talwar GP. Vaccines and passive immunological approaches for the control offertility and hormone-dependent cancers. Immunol Rev. 1999 Oct;171:173-92.Review.20) United Nations AIDS Information.21) van Ginkel FW, Nguyen
Janeway's Immunobiology 8th Edition (2012), Chapter 12 and Article "Mucosal Immunity and Vaccines" by Robyn Seipp attached at end of lecture notes. LECTURER Katherine L. Knight, Ph.D. Host Defense 2013 Mucosal Immunity April 16, 2013 Katherine L.Knight, Ph.D. .