Transcription
Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications forPharmacotherapyActivity No. 0217-0000-11-066-L01-P (Knowledge-Based Activity)Monday, October 179:15 a.m.–10:45 a.m.Convention Center: Spirit of Pittsburgh Ballroom AModerator: Tien M.H. Ng, Pharm.D., FCCP, BCPSAssociate Professor, Department of Pharmacy Practice, University of Southern California, Los Angeles,CaliforniaAgenda9:15 a.m.Overview of the Immune System and Application to DiseasePathophysiologyVal R. Adams, Pharm.D., FCCP, BCOPAssociate Professor of Pharmacy Practice and Science,University of Kentucky College of Pharmacy, Lexington,Kentucky9:45 a.m.Immunotherapy in Neurologic DiseaseMelody Ryan, Pharm.D., MPH, FCCP, BCPS, CGPAssociate Professor, University of Kentucky, Lexington,Kentucky10:15 a.m.PRO/CON Debate: Targeting Inflammation and the Preventionand Treatment of Cardiovascular DiseaseSheila L. Stadler, Pharm.D., BCPS (AQ Cardiology)Clinical Pharmacy Specialist, Kaiser Permanente of Colorado,Aurora, Colorado; Clinical Assistant Professor, University ofColorado–Denver School of Pharmacy, Aurora, ColoradoandCraig D. Williams, Pharm.D.Clinical Associate Professor, Department of Pharmacy PracticeCollege of Pharmacy, Oregon Health & Science University,Portland, OregonFaculty Conflict of Interest DisclosuresVal R. Adams: no conflicts to discloseMelody Ryan: no conflicts to discloseSheila L. Stadler: no conflicts to discloseCraig D. Williams: no conflicts to discloseAnnual MeetingCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy1
Learning Objectives1. Describe the key components of the innate immune system and acquired immune response.2. Identify how components of the immune system can contribute to pathophysiologic processes ofdisease.3. Describe the current understanding of the pathophysiologic mechanisms of immune-mediatedneurologic disease.4. Evaluate the evidence and controversies for the use of immunomodulating therapy in thetreatment of demyelinating neuropathies.5. Discuss the evidence for inflammatory markers and their association with various cardiovasculardiseases.6. Compare and contrast the evidence for treatment modalities targeting inflammation and theireffect on clinical outcomes.Self-Assessment QuestionsSelf-assessment questions are available online at www.accp.com/amAnnual MeetingCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy2
2011 ACCP Annual MeetingConflicts of InterestVal R. Adams, Pharm.D., FCCP, BCOPAssociate ProfessorUniversity of KentuckyI have no real or perceived conflict of interest toreportOverview of the ImmuneSystem and Application toDisease PathophysiologyThe Immune SystemAn Army Within A crucial component for survivalWell coordinated system primarily focused onkilling foreign invading predators (but it doesmuch more))If it becomes dysfunctional due tocommunication errors, lack of soldiers, etc. therisk of damaging the nation goes up drasticallyAn overview of the ranks, their charges, andcommunications, and will be reviewed.Immune System Protection against pathogensAllergic reactions to innocuous substancesOrgan graft rejectionAutoimmunityTumor immunity/surveillanceOthers AtherosclerosisNeuronal protectionAngiogenesisLipid metabolismObjectives1. Describe the key components of theinnate immune system and acquiredimmune response.2. Identify how components of the immunesystem can contribute topathophysiologic processes of disease.Pathogen ResponsePhysical –biochemical eTimeCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy3
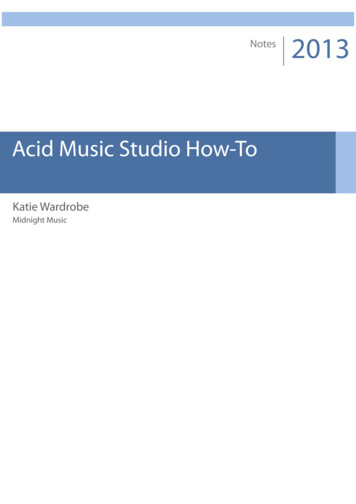
2011 ACCP Annual MeetingInnate Immunity:Soldier on Patrol (Phagocytes) Macrophages First on the scene, resident in most tissues (skin, mucosalsurfaces, vessels)gg , virus via receptor(s)p ( ) that recognizegRecognizebacteria,, fungus,common pathogen surface constituents (activate themacrophage)Pathogen is engulfed and degradedCommunication to comrades via cytokines/chemokinesRecruitment of other cells (neutrophils) and initiation ofinflammationInnate Immunity:MØ Recognize PatternsNK-like C-typelectin-like: e.g.Dectin-1Scanvenger:e.g. SR-A orCD36Integrine.g. CR3(CD18/11bGPI-anchored:e.g. CD14Toll-like receptorse.g. TLR2, TLR4Ig Superfamily:e.g. FcRAnnu. Rev. Immunol. 2005. 23:901–44Janeway’s immunobiology 7th ed Garland ScienceInnate Immunity:MØ Activation ResponseTNF- – Vascular effects - permeabilityallowing cell, Ig, compliment access - lymph drainage, fever, shockInnate Immunity:ComplementClassical ActivationLectin ActivationLectin binding toPathogen surfaceAntigen: AntibodyAlternative ActivationCompliment bindingto pathogen surfaceIL-1 – Vascular effect, activates Lymphs,local tissue destruction, fever, IL-6IL-6 – Lymph activation, Ig production,fever, acute phase protein productionIL-8 (CXCL8) – Chemotactic factor toattract neutrophils, basophils, and T-cellsto siteActivated MØ engulfs pathogen andSecretes cytokines/chemokinesIL-12 - Activates NK cells, inducesdifferentiation of CD4 cells to TH1Activation of the Compliment CascadeC3a, C5aInflammatory mediatorRecruitment ofphagocytesC3b (opsonization)Binds to complementReceptors onPhagocytes – leads toRemoval of pathogensJaneway’s immunobiology 7th ed Garland ScienceInnate Immunity:Next to Arrive: Neutrophils Formation of a membraneAttach complex (MAC)Creates holes in cellWall leading to death.Janeway’s immunobiology 7th ed Garland ScienceInflammatory ResponseNeutrophils (inflammatory cell responder) Attracted to the infection via chemokines (e.g. IL-8)Vascular effects (part of inflammation): vasodilation(slow blood flow)flow), increase endothelial adhesion andmolecule expression; allowing neutrophils to adhere tothe vessel at the infection site, then exit the circulationinto the tissue (diapedesis), where they can identifypathogens via receptors (similar to MØ) andphagocytize and destroy them.Short lived and usually die after phagocytosisNormal Vessel w/ NeutrophilInflamed vessel w/ NeutrophilsExtravasating into the tissueJaneway’s immunobiology 7th ed Garland ScienceCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy4
2011 ACCP Annual MeetingInnate Immunity:Natural Killer Cells Innate Immunity:InflammationLymphoid cells that circulate in blood and areactivated by IL-12 and IFN- and IFN- IL-12 synergistically w/ TNF- stimulate NKcells to make and secrete INF- INF Recognize cells through (activating &inhibiting) surface receptors to helpdifferentiate normal cells versusabnormal/infected target cellsRelease cytotoxic granules that kill target cellsInflammatory ResponseCytokines release initiated by MØ – then expandedLipid inflammatory mediators: prostaglandins,leukotrienes, and platelet-activating factor areenzymatically produced by MØ3 essential roles Augment killing by front line cells Induce local blood clotting to prevent infectiousspread to the blood Promote tissue repair and healing Antigen Presentation Professional APCs Macrophages, dendritic cells, B cellsPresent antigens in context of MHC molecules MHC – I: presents to CD8 T cells Activated monocytes differentiate intoMØs and dendritic cells and canbecome antigen presenting cells (APCs),which bridge the innate and adaptiveImmune systemInflamed vessel w/ MonocytesExtravasating into the tissueCell Mediated ImmunityExpressed on all nucleated cellsPresent antigens from intracellular pathogens (virus)MHCII—presents to CD4 T cells Expressed mostly by lymphoid cells (APCs)Present antigens from extracellular pathogens (Bacteria)All about the T-cellTH1APCCTLIL-10IL-2IL-2TcNKThCytokinesM Stimulates MØProd. IL-2, INF- TrIL-4, IL-5, IL-6B-cellB cellCD8 TcellMHC1 andantigenCD28B7CD4 TTcellllMHC2 andantigenTH2APCIL-8Virally InfectedPMNAntibodyIL-1, TNF- THKillIL-1TH17Not pictured: T reg which suppressThe immune system (IL-10)StimulateB-cell (IL-4, IL-5)differentiation toplasma cellsStimulateEndothelial cellsrecruit PMNsearly in adaptivephaseCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy5
2011 ACCP Annual MeetingT-cell activation/inhibitionT-cell signal transductionAPCCD137-LCD137 ( )T cellMHC-AgSignal 1CD3CD4/CD8T-CellCD28 ( )B7Signal 2TCRLckAntigenPresentingCellPD-1-LPPPD-1 (-)CD40ZAP-70PCTLA-4 (-)B7Ca dependentCalcineurinCD40-L ( )PDAGPKC pathRAS, ERKJNK pathNFATNF-kBAP-1Ag Antigen; CTLA-4: Cytotoxic T-lymphocyte associated antigen 4; L ligand; MHC major histocompatibilitycomplex; TCR T-cell receptor; PD-1 Program death 1. Seetharamu et al. Expert Rev Anticancer Ther. 2009;9:839-849.AntibodyQuantitative ResponseB-cell Activation, Proliferation,and DifferentiationIL-4, IL-5, IL-6TH2CD40LBIL-4CD40BBAntigenPlasmaCellBBBSurface IgProliferationDifferentiation andAntibody ProductionAntibody MOA Host DefenseIgG1 ADCC ComplementComplementInnate Immediate0-4 hoursInfection recognized bypreformed non-specificelements and effectorsDefeatPathogenInnateIt –Early4-96 hoursPathogenrecognizedP thi dby MØ throughmicrobial moleculesInflammation,recruitmentI fltiittand activation of effectorcellsAdaptiveResponse 96 hoursInnate immune effectorcells activated,inflammation–Dendritic cells presentantigenAntigen recognition by Band T cells – cellexpansion, differentiation,and activation of effectorfunctionsBacteriaFCReceptorDefeatD f tPathogenDefeatPathogenMacrophageCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy6
2011 ACCP Annual MeetingWhen Things Go WrongThe Army Within10,000 foot InfectiousPathogenInnocuousSubstanceHost DefenseRecurrent/infectionAllergyNo responseRejectionAcceptanceGrafted OrganTumorTumor ImmunityCancerNormalTissue/OrganNo responseAutoimmunityCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy7
2011 ACCP Annual MeetingConflicts of InterestMelody Ryan – nothing to declareImmunotherapy in NeurologicDiseaseMelody Ryan, Pharm.D., MPHUniversity of KentuckyObjectives Describe the current understanding of thepathophysiologic mechanisms of immunemediated neurologic diseaseEvaluate the evidence and controversies forthe use of immunomodulating therapy in thetreatment of multiple sclerosisT Cells Adhesion molecule (α4β1-integrin)on T cells allows binding to ICAM-1and VCAM-1 on vascular endothelialcellsT cell transmigratesgthroughg the cellsand breaches the blood-brain barrierT cell re-activated by an APCActivated T cell enters theparenchyma with help of matrixmetalloproteinases 2 and 9Walter S, Fassbender K. Cell Physiol Biochem 2010;25:49-56.Pathophysiology of MSc. 1995 It is an autoimmunediseaseSomething bad happensto the myelinc. 2011 Inflammatory component Responsible for relapsesNeurodegenerativecomponent Responsible for disabilityTh17 Cells IL-6, produced by activated T cells andmacrophages, is important for generation ofTh17 cellsTh17 cells produce IL-6IL 6, IL-17IL 17, IL-21IL 21, IL-22IL 22,and tumor necrosis factor-α (TNF-α)Codarri L, et al. Curr Opin Neurol 2010;23:205-11.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy8
2011 ACCP Annual MeetingBeta Interferons Suppress proliferation and migration of the Tcells, particularly Th17 cellsDecreases antigen presentation by MHCclass II moleculesDecreases integrin to prevent T cell migrationReduces matrix metalloproteinase 9 tostabilize the blood-brain barrierInhibit inflammatory cytokines increase antiinflammatory cytokinesBeta InterferonsLong-term Efficacy Merson TD, et al. Neuromol Med 2010;17:99-132.Graber J, et al. Clin Neurol Neurosurg 2010;112:583-91.Aktas O, et al. Trends Neurosci 2010;33:140-52.Beta InterferonsControversy Neutralizing antibodies Develop in up to 44% of patients on β interferonsLeast frequent in lowest dose and lowestfrequencyqy administered β interferonsIf persistent, higher relapse rateWith time, may disappearPresence correlates with reduction in MxAinduction assay which also predicts relapse ratesAll forms effective against placebo16 years worth of data with interferon β-1bSustained 40% reduction in relapse rate andslower rate of disease progression in patientstaking continuously compared to placebo orshort-term use of interferon β-1bCaveat: sustained reduction in relapse ratenot seen for IM interferon β-1a, but thosetreated earlier had better long-term outcomesFreedman MS. Neurology. 2011;76(1 Suppl 1):S26.Reder AT, et al. Neurology. 2010;74:1877.Glatiramer Acetate Suppress proliferation and migration of the TcellsInduces apoptosis of T cellsInduces a shift from Th1 to Th2 cellsGoodin DS, et al. Neurology 2007;68:997.Polman CH, et al. Lancet Neurol 2010;9:740.Aktas O, et al. Trends Neurosci 2010;33:140-52.Glatiramer AcetateLong-term EfficacyControversyBest TreatmentInterferon vs. Interferon Approximately 12 years of follow-up data80% reduction in relapse rate compared tobaseline dataDisability scores also improved/remainedstable in patients continuously treatedcompared to those withdrawnFreedman MS. Neurology. 2011;76(1 Suppl 1):S26.TrialDesignResultsEVIDENCEINF β-1a 44 μg SQ 3x/wk vs.INF β-1aβ 1a 30 μg IM 1x/wk; 24weeksDecreased relapse rate andactive lesions on MRI with INFβ-1a 44 μg SQ 3x/wkINCOMININF β-1b 250 μg SQ QOD vs. Decreased relapses and activelesions on MRI with INF β-1bINF β-1a 30 μg IM 1x/wk; 2250 μg SQ QODyearsClanet, et al.INF β-1a 30 μg IM 1x/wk vs.INF β-1a 60 μg IM 1x/wk; 36monthsNo difference betweentreatments in disability or rate ofprogressionPanitch H, et al. Neurology 2002;59:1496-506.Durelli L, et al. Lancet 2002;359:1453-60.Clanet M, et al. Neurology 2002;59:1507-17.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy9
2011 ACCP Annual MeetingControversyBest TreatmentInterferon vs. Glatiramer AcetateTrialDesignBEYONDINF β-1b 250 μg SQ QOD vs. No differenceINF β-1bβ 1b 500 μg SQ QOD vs.vsglatiramer acetate 20 mg QD;2 yearsResultsREGARDINF β-1a 44 μg SQ 3x/wk vs. No differenceglatiramer acetate 20 mg QD;96 weeksBECOMEINF β-1b 250 μg SQ QOD vs. No differenceglatiramer acetate 20 mg QD;2 years; MRI studyCheck-in Question 1Which is the best first-line treatment for MS?a. Interferon β-1a SQ 3x/weekb. Interferon β-1b SQ QODc. GlatiramerGl tiacetatet t 20 mg QDd. One of these is not better than the othersO’Connor P, et al. Lancet Neurol 2009;8:889-97.Mikol DD, et al. Lancet Neurol 2008;7:903-14.Cadavid D, et al. Neurology 2009;72:1976-983.Mitoxantrone Eliminates and deactivates monocytes andmacrophagesInhibits T cell proliferation and migrationInhibits B cell activationCompared to placebo, decreased number ofexacerbations and improved MRI parametersMitoxantrone - Controversy Cardiotoxicity Dose-limiting to 140 mg/m2/lifetimeMay not be dose-relatedMay have late-onsetlate onsetNew FDA guideline for LVEF evaluation prior toeach doseAktas O, et al. Trends Neurosci 2010;33:140-52.Hartung HP, et al. Lancet 2002;360:2018.Coyle PK. Am J Manag Care 2010;16(6 Suppl):S164.Kingwell E, et al. Neurology 2010;74:1822-6.www.fda.govCheck-in Question 2Natalizumab Why is there a lifetime maximum dose formitoxantrone?a. There is a risk of leukemiab. There is a ppermanent discoloration ofthe sclerac. There is a risk of cardiotoxicityd. There is a risk of allergic reaction Humanized monoclonal IgG4-antibodyBinds to α4β1-integrin so the T cell cannotbindPrevents the migration of the T cell into theCNSReduced relapse rates by 68% (0.23/y v.0.73/y)Reduced disability progression by 42% over2 yearsReduced new lesions on MRI by 83%Coyle PK. Am J Manag Care 2010;16:S164-70.Polman CH, et al. N Engl J Med 2006;354:899-910.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy10
2011 ACCP Annual MeetingNatalizumab - Antibodies 9% of patients develop antibodies at somepoint during treatment; 6% have persistentantibodies82% with persistent antibodies develop themwithin the first 12 weeks of therapyCauses decreased efficacyNatalizumab – ProgressiveMultifocal Leukoencephalopthy Opportunistic infection caused by reactivationof the JC DNA virus 50-86% of adults have antibodies to JCVRapid progression and often causes death orsevere disabilityShortly after marketing, 3 cases reported andnatalizumab was suspendedRe-introduced in 2006 with a restricteddistribution and extensive monitoring programFoley J. Am J Manag Care 2010;16:S178-83.Clifford DB, et al. Lancet Neurol 2010;9:438-46.Miravalle A, Corboy JR. Neurol Clin Pract 2010:75(Suppl 1):S22-7.PML after Re-introductionTreatment of PML Exposure of 65,000 MS patients with 28 newcases of PMLReporting rate 1-2/monthRisk is proportional to exposure durationSymptoms: neurobehavioral, motor,language, cognitive, or vision changes,seizures, hemiparesis, tremor Withdrawal of natalizumabAggressive immune reconstitution Immune reconstitution inflammatorysyndrome Plasma exchangeImmunoabsorptionHigh-dose steroidsOnly 8 fatalitiesClifford DB, et al. Lancet Neurol 2010;9:438-46.Clifford DB, et al. Lancet Neurol 2010;9:438-46.Sphingosine 1-phosphateSphingosine 1-phosphate Sphingolipids are structural components of cellmembranesSphingomyelin is metabolized to sphingosine 1phosphate (S1P)There are 5 receptors for S1P S1PR1-3 are widespread in CNS, vascular, andimmune systemsS1P4 is in lymphoid tissueS1P5 is on natural killer cells and in oligodendrocytesHla T, Brinkmann V. Neurology 2011;76(suppl 3):S3-8. S1P and S1PR1 controls entry and exit of naïveB and T cells into the lymphatic systemsS1P regulates heart rate, vascular tone, andblood pressure and may have effects onpulmonary functionS1P promotes the survival of oligodendrocytesand oligodendrocyte precursor cells (OPC) andOPC differentiationS1P is involved with neurite extension andretractionHla T, Brinkmann V. Neurology 2011;76(suppl 3):S3-8.Soliven V, et al. Neurology 2011;76(suppl 3):S9-14.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy11
2011 ACCP Annual MeetingFingolimod S1PR modulator Prevents the exit of naïve T cells and centralmemory T cells (TCM) from the lymphoidtissues Binds to all S1PR except S1PR2TCM include Th17 cellsIncreases the number of progenitor and matureoligodendrocytes and protects them from celldeathIncreases brain-derived neurotrophic factorFingolimod - EfficacyStudyRelapse Rate Relapse-freeNew orEnlarged MRILesions(mean)Fingolimod v.1033Placebo; 2-year studyF 0.18/yP 0.40/yF 74.7%P 45.6%F 2.5 P 9.81153F 0.16/yI 0.33/yF 82.6%I 69.3%F 1.7 I 2.6Fingolimod v.Interferon β-1a IMQweek; 1-year studynChun J, Hartung HP. Clin Neuropharm 2010;33:91-101.Kappos L, et al. N Eng J Med 2010;362:387-401.Cohen JA, et al. N Eng J Med 2010;362:402-15.Check-in Question 3Controversy -TreatmentEscalation vs. InductionSP is started on fingolimod. She has a CBC 1week after beginning therapy. What do youexpect the results to show? a.b.c.d.e.Increased WBCDecreased WBCIncreased plateletsDecreased plateletsNo change Escalation algorithms begin with the safesttreatments and move on to more aggressivetherapies only in the event of treatmentfailureInduction algorithms concentrate alltherapeutic efforts on the early phases of thedisease, which ultimately defines prognosisEdan G, et al. J Neurol Neurosurg Psychiatry 2011.Boggild M. J Neurolog Sci 2009;277(Suppl 1):S50-4.Conclusion Much is now known, but much is left to learnabout the role of the immune system in MSSeveral therapies are now available fortreatment of MS; however,however there is noconsensus on the best therapyThere is controversy regarding the place intherapy of all currently available medicinesCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy12
2011 ACCP Annual MeetingPRO: Targeting inflammationshould be a goal for theprevention and treatment ofpcardiovascular disease No conflicts to discloseMonday, October 17, 2011Sheila L. Stadler, Pharm.D., BCPSClinical Pharmacy Specialist, Kaiser Permanente ofColorado, Aurora, Colorado; Clinical AssistantProfessor, University of Colorado–Denver School ofPharmacy, Aurora, ColoradoObjectivesBackground Discuss the evidence for inflammatorymarkers and their association with variouscardiovascular diseases Compare and contrast the evidence fortreatment modalities targetinginflammation and their effect on clinicaloutcomes Cardiovascular disease (CVD) is abnormalfunction of the heart and blood vessels CVD is the leading cause of death worldwideInflammation in Early AtherosclerosisMacrophage and Inflammation Triggers of atherosclerosis can initiateexpression of adhesion molecules byendothelial cells which allows attachmentof leukocytes to arterial wall Likely culprit: vascular cell adhesionmolecule-1 (VCAM-1) Proinflammatory cytokines provide achemotactic stimulus to adherentleukocytes to migrate into the intima Monocytes transform into macrophages,express scavenger receptors, engulf lipidparticles, and become foam cells Macrophages multiply and releaseproinflammatory growth factors andcytokinesCurricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy13
2011 ACCP Annual MeetingT-cells and Plaque InflammationCytokine Cascade Antigens presented by macrophages anddendritic cells trigger the activation of antigenspecific T cells in the artery Activated T cells produce Th1 cytokines (e.g.,interferon-γ), which activate macrophages andvascular cells, leading to inflammation Regulatory T cells modulate the process bysecreting antiinflammatory cytokines(interleukin-10 and transforming growth factorβ) Activated immune cells in the plaqueproduce inflammatory cytokines(interferon-γ, interleukin-1, and tumornecrosis factor), which induce theproduction of interleukin-6 Interleukin-6 stimulates the production oflarge amounts of acute-phase reactants,including C-reactive protein (CRP), serumamyloid A, and fibrinogenLipoprotein-associatedphospholipase A2 (Lp-PLA2) Lp-PLA2 is an inflammatory biomarker andis directly related to propensity of plaquerupture Lp-PLA2 is an enzyme that hydrolyzesoxidized phospholipids and releaseslysophosphotidylcholineBiomarkers of Inflammationproposed for diagnostic use VCAM-1IL-6hsCRPLp-PLA2So .inflammation is a key factor inatherosclerosis.DDoesththatt mean we shouldh ld targetttinflammation for the prevention andtreatment of CVD?hsCRP for Risk Prediction 4040-50%50% off ththose att iintermediatetdi t riski kaccording to ATP III were reclassified bythe addition of hsCRP and family history toclinically relevant higher or lower riskgroupsJAMA. 2007;297:611-619.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy14
2011 ACCP Annual MeetinghsCRP as a Potential Therapeutic Goal Clinical outcomes bestamong statin-treatedstatin treatedpatients who not onlyachieved LDL-C 70mg/dL, but also achievedhsCRP 2 mg/L 28% lower chance ofrecurrent MI or vasculardeathJ Am Coll Cardiol. 2005;45:1644-8. JUPITER trial enrolled 17,802 without CVD withLDL-C 130 mg/dL and hsCRP 2 mg/L Randomized to rosuvastatin 20 mg or placebo 44% reduction in primary endpoint of all vasculareventsCirculation. 2006;114:281-288.Lp-PLA2 as a Therapeutic Target Darapladib is a direct inhibitor of Lp-PLA2 Shown to prevent necrotic expansion ofhuman coronary atherosclerotic plaque PhasePhIII studyt d currentlytl recruiting:itiTheThstabilization of plaques using darapladibthrombolysis in myocardial infarction 52trial (SOLID-TIMI 52)RebuttalhsCRP to Target TherapyN Engl J Med 2008;359:2195-207.Conclusion There is evidence that numerousinflammatory markers are associated withCVD Strongest evidence lies with utilizing hsCRPfor risk prediction, to identify patients whomay benefit from statins, and as a potentialdual goal along with LDL-C Lp-PLA2 may provide information aboutplaque inflammation and stability and as adirect target for treatment1. Proof of concept2 Prospective validation2.3. Incremental value4. Clinical utility5. Clinical outcomes6. Cost-effectivenessCirculation. 2009;119:2408-2416.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy15
2011 ACCP Annual MeetingCost-Effectiveness for hsCRP 5 year NNT for JUPITER was 25 forprimary trial end point and 32 for “hard”end point of MI, stroke, or death. Comparable 5 year NNT values between86-140 have been reported as costeffective for treatment of hypertension Recommendations for measurement of CRP Class IIa– In men 50 years or women 60 years with LDL-C 130 mg/dL; not on lipid-lowering, hormonereplacement, or immunosuppressant therapy; withoutCHD, diabetes, chronic kidney disease, severeinflammatory conditions, or contraindications tostatins, measurement of CRP can be useful in theselection of patients for statin therapy.– Level of Evidence: BCirculation. 2010;122:2748 –2764.CVD continues to be the leading cause ofdeath world wide Recommendations for measurement of CRP Class IIb– In asymptomatic intermediate-risk men 50 years ofage or women 60 years of age, measurement ofCRP may be reasonable for cardiovascular riskassessment– Level of Evidence: BEven with treating to patients to goal fortraditional risk factors, there is still residualriskWe need to explore beyond the traditionalrisk factors and target inflammation for theprevention and treatment of CVDCirculation. 2010;122:2748 –2764.Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy16
2011 ACCP Annual MeetingACCP Pro-Con debate 2011: No conflicts to discloseTargeting inflammation should NOT be a goal for the prevention andtreatment of cardiovascular diseaseCraig D. Williams, Pharm.D.Clinical Associate Professor, Department of PharmacyPractice College of Pharmacy, Oregon Health & ScienceUniversity, Portland, OregonI accept, as should we all, that inflammation plays a veryimportant role in atherosclerosisWhile hs-CRP gets most attention, the inflammatory process inatherosclerosis clearly involves multiple lines of inflammationJCI, 2001Circulation 2000Circulation,JACC, 2002NEJM, Jan 14th, 1999But .the question is what to do about it: “Should we targetinflammation to prevent and treat CAD?”Non-steroidal, anti-inflammatory agents also clearly offer no benefit forCAD and appear to be associated with riskTwo potential areas to target:1. Directly target inflammation with an anti-inflammatory approach2. Use of inflammatory biomarkers to better target anti-atherogenic therapyScand J Rheumatol 2010;39:485-89Circ 2011;123:2226-35“mean IMT was correlated with a higher cummulative corticosteroid intake ”Contem ChallAutoimmun2009;1173:814-21Conclusions: “Even short-term treatment with NSAIDs was associated with increasedrisk of death and recurrent MI .any NSAID use should be limited from a CVDsafety point of view.”And we all know the story of Vioxx and selective COX2 inhibitors .“There are conflicting data regarding the effect of biologics on atherosclerosis”Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy17
2011 ACCP Annual MeetingAtherosclerosis is a lipoprotein driven processBasic Science for CliniciansSubendothelial Lipoprotein Retention as the Initiating Process in AtherosclerosisUpdate and Therapeutic ImplicationsIra Tabas, MD, PhD; Kevin Jon Williams, MD;Jan Borén, MD, PhDSo, the inflammation in atherosclerosis is a RESPONSE to theunderlying disease which is subendothelial retention of lipoproteins.Treating atherosclerosis with anti-inflammatory agents is akin to treatingpneumonia with prednisone.There may even be some benefit of vascular inflammation:Circulation2007;115:548“local arterial inflammation signals the release of bone marrow-derived stemcells that participate in the healing response of the injured blood vessel”Circulation, October 16th, 2007One area where ‘smart’ targeting of native immunity has been tried is inthe elevation of HDL to retard atherosclerosis.Tr in Endo Metab, Jan 2011Immunology and Cell Biology, Jan 2010HDL isi a particleti l whichhi h did nott evolvelas part of the traditional lipoproteinpathway but rather as part of our innateimmune system (note its completelyseparate lifecycle from the atherogenic,apoB-containing lipoproteins)CETP inhibition with torcetrapib in 15,067 high risk patients increased HDLc by 72%and increaseed total mortality by 58%2. Use of inflammatory biomarkers as prognostic factors to direct therapyA word of caution:New England Journal of MedicineApril 1st, 2004“C-Reactive Protein and Other Circulating Markers of Inflammation inthe Prediction of Coronary Heart Disease”To minimize confounding from fluctuations in hs-CRP, this analysis performed over 12year period on 2,459 case patients who had an MI compared to 3,696 controles whoremained disease free.PK Shaw, Circulation, 2000“It remains to be proven that any of the inflammatory markers provideincremental information over and above traditional risk stratification.”Curricular Track I—The Role of the Immune System in Disease Pathophysiology: Implications for Pharmacotherapy18
2011 ACCP Annual MeetingThe story of inflammatory cytokines in CAD is long and tortuous:Inflammatory cytokines clearly play an important role in atherosclerosis Framingham: Many CHD Patients Have TC Below orNear AverageNo.Non-CHD 137840May 2001CHD193Mean (mg/dL) SD219412445130Population (%) but VCAM-1, like others has an unclear role in predicting eventsSept 2001“no meaningful,
Janeway's immunobiology 7th ed Garland Science Innate Immunity: MØ Recognize Patterns Scanvenger: e.g. SR-A or CD36 NK-like C-type lectin-like: e.g. Dectin-1 GPI-anchored: e.g. CD14 Integrin e.g. CR3 (CD18/11b Ig Superfamily: e.g. FcR Toll-like receptors e.g. TLR2, TLR4 Annu. Rev. Immunol. 2005. 23:901-44 Innate Immunity: MØ Activation .