Transcription
Economic Effects of the1918 Influenza PandemicImplications for a Modern-day PandemicThomas A. GarrettAssistant Vice President and EconomistFederal Reserve Bank of St. LouisNovember 2007CA0721 11/07
Economic Effects of the1918 Influenza PandemicImplications for a Modern-day PandemicThomas A. GarrettAssistant Vice President and EconomistFederal Reserve Bank of St. LouisThomas A. Garrett received his doctoral and master’s degrees ineconomics from West Virginia University in Morgantown, W.Va.,in 1998 and 1997, respectively. He received his bachelor’s in business administration from Shippensburg University of Pennsylvaniain 1993. Before coming to the St. Louis Fed, he was an assistantprofessor in the Department of Agricultural Economics at KansasState University. His research interests include state and local publicfinance and public choice, public finance aspects of state lotteriesand gambling, and economic history.The views expressed here are those of the author and not necessarily those of theFederal Reserve Bank of St. Louis or the Federal Reserve System.The report is also available online atwww.stlouisfed.org/community/other pubs.html.
Table of ContentsI.IntroductionII.Overview of the 1918 Influenza PandemicPandemic Mortalities in the United StatesState and City Pandemic MortalitiesInfluenza Mortalities and RacePandemic Mortalities in Eighth Federal Reserve District StatesIII.7Economic Effects of the 1918 Influenza Pandemic919The 1918 Influenza Pandemic in the NewsLittle Rock, Ark.Memphis, Tenn.Survey of Economic ResearchSummaryIV.Implications for a Modern-day Pandemic21V.Final Thoughts22
AbstractThe possibility of a worldwide influenza pandemic inthe near future is of growing concern for many countriesaround the globe. Many predictions of the economicand social costs of a modern-day influenza pandemic arebased on the effects of the influenza pandemic of 1918.This report begins by providing a brief historical background on the 1918 influenza pandemic, a short-lived,but tragic event that has all but escaped the public’sconsciousness today.Detailed influenza mortality statistics for cities and states,including those in the Eighth Federal Reserve District, arepresented. These data provide insight into mortality differences based on race, income and place of residence. Next,anecdotal evidence on the economic effects of the 1918influenza are reported using newspaper articles publishedduring the pandemic. There is also a survey of economicresearch on the subject. The information presented in thisreport and information provided in two prominent publications on the 1918 influenza pandemic are then used toformulate a list of the likely economic effects of a modernday influenza pandemic.5
6
I. IntroductionThe possibility of a worldwide influenzapandemic (e.g., the avian flu) in the nearfuture is of growing concern for many countries around the globe. The World Bankestimates that a global influenza pandemicwould cost the world economy 800 billionand kill tens-of-millions of people.1 Researchers at the U.S. Centers for Disease Control andPrevention calculate that deaths in the UnitedStates could reach 207,000 and the initial costto the economy could approach 166 billion,or roughly 1.5 percent of the GDP.2 Longrun costs are expected to be much greater.The U.S. Department of Health and HumanServices paints a more dire picture—up to 1.9million dead in the United States and initialeconomic costs near 200 billion.3While researchers and public officials canonly speculate on the likelihood of a globalinfluenza pandemic, many of the worst-casescenario predictions for a current pandemicare based on the global influenza pandemicof 1918, which killed 675,000 people in theUnited States (nearly 0.8 percent of the 1910population) and 40 million people worldwidefrom the early spring of 1918 through the latespring of 1919.4 In all of recorded history,only the Black Death that occurred throughoutEurope from 1348-1351 is estimated to havekilled more people (roughly 60 million) over asimilar time period.5The years 1918 and 1919 were difficult notonly as a result of the influenza pandemic;these years also marked the height of U.S.involvement in World War I. Given the magnitude and the concurrence of both the influenza pandemic and World War I, one wouldexpect volumes of research on the economiceffects of each event. Although significantliterature on the economic consequences ofWorld War I does exist, the scope of researchon the economic effects of the 1918 influenzapandemic is scant at best. Most research hasfocused on the health and economic outcomesof descendants of pandemic survivors and themortality differences across socioeconomicclasses.6 Certainly an event that caused 40million worldwide deaths in a year should beclosely examined not only for its historicalsignificance, but also for what we can learn inthe unfortunate chance the world experiencesanother influenza pandemic.This report discusses some of the economiceffects of the 1918 influenza pandemic in theUnited States. The first sections of the reportpresent and discuss demographic differencesin pandemic mortalities. Were deaths higherin cities than in rural areas? Did deaths differ by race? Did deaths differ by income?Detailed influenza mortality data at variousgeographic and demographic levels at the timeof the pandemic are available. The presentation of numerous mortality data series allowsfor an almost unlimited number of comparisons and analyses that afford the reader theopportunity to study the available data andgenerate his own analyses and conclusions inaddition to those presented here.Evidence of the effects of the pandemic onbusiness and industry is obtained from newspaper articles printed during the pandemic,with most of the articles appearing in newspapers from the Eighth Federal Reserve Districtcities of Little Rock, Ark., and Memphis, Tenn.Newspaper articles from the fall of 1918 wereused because of the almost complete absenceof economic data from the era, such as dataon income, employment, sales and wages.This absence of data, especially at local levels(e.g., city and county) is a likely reason for thescarcity of economic research on the subject,though several studies that have used availableeconomic data are reviewed here and nicelycomplement the information obtained fromnewspaper articles.Although the influenza pandemic occurrednearly 90 years ago in a world that was muchdifferent than today, the limited economic dataand more readily available mortality data fromthe time of the event can be used to make reasonable inferences about economic and socialconsequences of a modern-day pandemic.Despite technological advances in medicineand greater health coverage throughout the20th century, deaths from a modern-day influenza pandemic are also likely to be related torace, income and place of residence. Thus,the geographic and demographic differences7
in pandemic mortalities from 1918 can shedlight on the possible effects of a modern-daypandemic, a point that is taken up in the lastsection of the report.Overview of the1918 Influenza PandemicThe influenza pandemic in the United Statesoccurred in three waves during 1918 and1919.7 The first wave began in March 1918and lasted throughout the summer of 1918.The more devastating second and third waves(the second being the worst) occurred in thefall of 1918 and the spring of 1919. According to one researcher:“Spanish influenza moved across theUnited States in the same way as the pioneers had, for it followed their trails whichhad become railroads the pandemic startedalong the axis from Massachusetts to Virginia leaped the Appalachians positionedalong the inland waterways it jumped clearacross the plains and the Rockies to Los Angeles, San Francisco, and Seattle. Then, withsecure bases on both coasts.took its time toseep into every niche and corner of America.”88But the pandemic’s impact on communitiesand regions was not uniform across the country. For example, Pennsylvania, Maryland andColorado had the highest mortality rates, butthese states had very little in common. Arguments have been made that mortality rateswere lower in later-hit cities because officialsin these cities were able to take precautionsto minimize the impending influenza, suchas closing schools and churches and limitingcommerce. The virulence of the influenza,like a typical influenza, weakens over time, sothe influenza that struck on the West Coastwas somewhat weaker than when it struck theEast Coast. But these reasons cannot completely explain why some cities and regionsexperienced massive mortality rates whileothers were barely hit with the influenza.Much research has been conducted over thepast decades to provide insights into why thepandemic had such different effects on different regions of the country.9The global magnitude and spread of thepandemic was exacerbated by World War I,which itself is estimated to have killed roughly10 million civilians and 9 million troops.10Not only did the mass movement of troopsfrom around the world lead to the spread ofthe disease, tens of thousands of Allied andCentral Power troops died as a result of theinfluenza pandemic rather than combat.11Although combat deaths in World War I didincrease the mortality rates for participatingcountries, civilian mortality rates from theinfluenza pandemic of 1918 were typicallymuch higher. For the United States, estimatesof combat-related troop mortalities are aboutone-tenth that of civilian mortalities from the1918 influenza pandemic.Mortality rates from a typical influenza tendto be the greatest for the very young and thevery old. What made the 1918 influenzaunique was that mortality rates were the highest for the segment of the population aged18 to 40, and more so for males than femalesof this age group. In general, death was notcaused by the influenza virus itself, but by thebody’s immunological reaction to the virus.Individuals with the strongest immune systems were more likely to die than individualswith weaker immune systems.12 One sourcereports that out of 272,500 male influenzadeaths in 1918, nearly 49 percent were aged20 to 39, whereas only 18 percent were underage 5 and 13 percent were over age 50.13 Thefact that males aged 18 to 40 were the hardest hit by the influenza had serious economicconsequences for the families that had losttheir primary breadwinner. As discussed laterin the report, the significant loss of primeworking-age employees also had economicconsequences for businesses.Despite the severity of the pandemic, it isreasonable to say that the influenza of 1918has almost been forgotten as a tragic event inAmerican history. This is not good, as learningfrom past pandemics may be the only way toreasonably prepare for any future pandemics.Several factors may explain why the influenzapandemic of 1918 has not received a notableplace in U.S. history.14First, the pandemic occurred at the same
time as World War I. The influenza strucksoldiers especially hard, given their living conditions and close contact with highly mobileunits. Much of the news from the day focusedon wartime events overseas and the currentstatus of America troops. Thus, the pandemicand World War I were almost seen as oneevent rather than two separate events. Second,diseases of the day like polio, smallpox andsyphilis were incurable and a permanent partof society. Influenza, by contrast, swept intocommunities, killed members of the population, and was gone. Finally, unlike polio andsmallpox, no famous people of the era diedfrom the influenza; thus there was no publicperception that even the politically powerfuland rich and famous were not immune fromthe virus.Although the influenza pandemic of 1918may be an event that has been relegated tothe shadows of American history, the eventhad significant economic effects. The fact thatmost of these effects were relatively short-liveddoes not make them less important to study,especially given the nonzero probability of afuture influenza pandemic.While not a primary focus of this report, theinfluenza pandemic of 1918 resulted in greathuman suffering in select areas, as increasingbody counts overwhelmed city and medical officials (partly exacerbated by personnel absences from the war). In some cities,like Philadelphia, bodies lay along the streetsand in morgues for days, similar to medievalEurope during the Black Death. In light of thepotential economic turmoil and human suffering, an understanding of state and federal government response to the 1918 pandemic mayalso provide some light into what, if anything,government at any level can do to prevent orminimize a modern-day pandemic.II. Pandemic Mortalities in theUnited StatesData on mortalities from the 1918 influenzapandemic are found in Mortality Statistics, anannual publication that is released by the U.S.Census.15 Mortalities resulting from hundredsof causes of death are listed (depending uponthe level of data aggregation), and are alsobroken down, in some cases, by age, race andsex. Data are available at the national, stateand municipal levels, and may be available byweek, month and year. In terms of coverage,“(a)ll death rates are based on total deaths,including deaths of non-residents, deathsin hospitals and institutions, and deaths ofsoldiers, sailors, and marines.”16 The mortalityrates used in this study represent deaths fromboth influenza and pneumonia in a given yearbecause “it is not believed to be best to studyseparately influenza and the various forms ofpneumonia.for doubtless many cases werereturned as influenza when the deaths werecaused by pneumonia and vice versa.”17Although Mortality Statistics provides aremarkable number of statistics, a major disadvantage of the earlier reports is that, in the1910s, data coverage is for 75 to 80 percentof the total population. This is because theU.S. Census acquired the mortality data froma registration area that consisted of a growinggroup of states over time. So, mortality datafor certain states are not consistently availableover time. For the purposes here, influenzamortality data for the 1910s are available forabout 30 states and encompass, on average,about 79.5 percent of the U.S. population. Acasual look at the states that did and did notreport mortality information does not revealany systematic differences across each group ofstates with regard to population, income andrace. So, the available mortality statistics areunlikely to provide a biased picture of influenza mortalities.The following sections report select influenza mortality data at various levels of dataaggregation (city and state), by race (white andnonwhite) and residence (urban versus rural).The abundance of mortality statistics makes itimpossible to use all existing data in a singlereport. However, the statistics used here doreveal some general mortality patterns thatprovide insights into which groups of peoplemay be most/least affected by a modern-daypandemic, as well as how influenza mortalitiesdiffered across cities and states.9
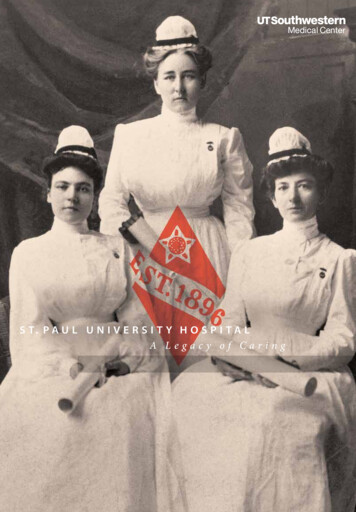
State and CityPandemic MortalitiesPandemic mortality rates (per 100,000) for27 states are shown in Table 1 for years 1918and 1919. The mortality rate for 1915 is alsoincluded, and the ratio of 1918 mortalities to1915 mortalities is shown to reveal the relativemagnitude of deaths in 1918 to a nonpandemic year. For the states shown in Table 1,Pennsylvania, Maryland and New Jersey hadthe highest mortality rates in 1918, whereasMichigan, Minnesota and Wisconsin had thelowest. The pandemic also lasted throughoutthe spring of 1919; so, the ranking of statesin 1918 does not reflect total mortalities ineach state for the entire pandemic (though therankings do remain similar).The ratio of the 1918 mortality rate and the1915 mortality rate ranges from a low of 3.2Table 1: Influenza Mortality Rates (per 100,000) for Select StatesState1910 pop.Area(sq. yRate1919MortalityRateRatio of1918 and1915 2.24119.6405.6178.53.425Notes: Mortality rates are from Mortality Statistics 1920 and include mortalities from influenza and pneumonia. Mortalities for South Carolina and Tennesseein 1915 are 1916 and 1917 figures, respectively.
(Indiana and New York) to a high of 6.5 (Montana). This means that the 1918 influenzamortality rates in Indiana and New York were3.2 times greater than influenza mortality ratesin a nonpandemic year, whereas 1918 ratesin Montana were more than 6 times greaterthan a nonpandemic year. One caveat is thatan equal increase in mortalities for a lowpopulation state and a higher-population statewill result in a greater mortality ratio for thelower-population state because the increase inmortalities is a greater percentage of the lowstate’s population. Nevertheless, a comparisonof 1915 mortality rates with those in 1918 and1919 clearly reveals how much more severethe 1918 influenza was relative to influenza ina nonpandemic year.Also shown in Table 1 are state population,area and population density. It serves as aninteresting exercise to see if there is a relationship between mortalities and state population,size and population density. It is also worthexploring whether the relationships are different in a pandemic year versus a nonpandemicyear. Table 2 presents correlations (and theirstatistical significance) between state population, area and population density, and 1915mortality rates, 1918 mortalities rates and theratio of the two mortality rates.Table 2: Correlations of StateCharacteristics with Influenza Mortalities1915MortalityRate1918MortalityRateRatio of1918 and1915 RatesDensity(pop/sq. mi.)0.632*0.447*-0.097Area(sq. te:* denotes statistical significance at 5 percent or better. Correlations are based on the data in Table 1 (n 27).The correlations shown in Table 2 reveal thatmortality rates in 1915 were greater in moredensely populated states (0.632), but lower inlarger states (-0.566). State size had no significant correlation with 1918 mortality rates,but population density was correlated with1918 mortality rates (0.447). Note, however,that the correlation between mortality ratesand density is less for 1918 mortalities thanfor 1915 mortalities. This finding, in additionto the fewer significant correlations (albeit justone), suggest that state size and populationdensity had less influence on mortality ratesin 1918 than in 1915. Thus, as suggested byearlier research, the location of individuals wasless of a factor in dying from the 1918 influenza than from a nonpandemic influenza.18Furthermore, the ratio of mortality rates hadno relationship with state size, population orpopulation density, as seen in the last columnof Table 2.Mortality statistics for 49 cities are listed inTable 3. As seen in the state-level statistics,influenza mortalities in U.S. cities during thepandemic were three to five times higher, onaverage, than during a nonpandemic year(1915). There is slightly more variation in1918 mortality rates across cities (standarddeviation 182) than across states (standarddeviation 146). The cities with the highest1918 mortality rates (Pittsburgh, Scranton andPhiladelphia) are all located in Pennsylvania,and the cities with the lowest rates GrandRapids, Minneapolis and Toledo are all locatedin the Midwest.To get an idea of the influenza’s effect onrural areas versus urban areas, the average1918 mortality in all cities in a state (for whichmortality data were available) was calculatedand then divided by the state-level mortalityrate.19 These ratios are shown in Table 4. Aratio 1 suggests influenza deaths were, onaverage, greater in a state’s cities than in therural areas of the state, and vice versa for aratio 1. As seen in Table 4, most of the ratiosare 1, with some much 1 (Missouri, Kansas,Tennessee), thus revealing that cities in theirrespective state had higher mortality rates thanrural areas of the states. This finding supportsthe positive correlation between populationdensity and influenza mortalities shown inTable 2.11
Table 3: Influenza Mortality Rates (per 100,000) for Select CitiesCityAlbany, N.Y.Atlanta, Ga.1910 pop.1915Mortality Rate1918Mortality Rate1919Mortality 0154,839Ratio of 1918 and1915 Rates1918 RankBaltimore, Md.558,485207.1836.5230.64.07Birmingham, Ala.132,685158.1843.6319.15.36Boston, Mass.670,585214.6844.7256.33.95Bridgeport, Conn.102,054206.0825.4272.34.08Buffalo, N.Y.423,715168.7637.5206.23.828Cambridge, 6191.53.035Cincinnati, Ohio353,591163.4605.4253.23.729Cleveland, Ohio560,663155.1590.9260.53.830Columbus, Ohio181,511136.5451.9213.53.343Dayton, Ohio116,577142.7525.2154.63.733Denver, Colo.213,381184.8727.7228.53.915Detroit, Mich.465,766148.1413.4242.42.846Fall River, Mass.119,295213.5799.7216.83.79Grand Rapids, Mich.112,571100.0282.793.82.849Indianapolis, Ind.233,650146.7459.4240.63.142Jersey City, N.J.267,779211.2756.6317.03.613Kansas City, Mo.248,381176.1718.1301.14.117Los Angeles, Calif.319,19887.4484.5186.85.538Lowell, Mass.106,294191.3696.1198.43.619Memphis, Tenn.131,105179.3666.1340.63.724Milwaukee, Wis.373,857158.9474.1187.73.041Minneapolis, Minn.301,408121.6387.7169.43.248Nashville, Tenn.110,364179.9910.2301.05.14New Haven, Conn.133,605207.9768.0212.33.711New Orleans, 65.82.731Newark, N.J.347,469146.6680.4213.34.621Oakland, Calif.150,17498.6496.6238.25.036Omaha, Neb.124,096150.9660.8191.84.426Chicago, Ill.New York, N.Y.Paterson, 222.94.93Pittsburgh, Pa.533,905260.11243.6431.84.81Portland, Ore.207,21469.6448.2246.46.444Providence, R.I.224,326191.4737.4253.33.914Richmond, Va.127,628209.9661.0269.53.125Philadelphia, Pa.
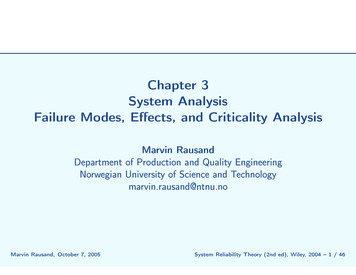
Table 3: Influenza Mortality Rates (per 100,000) for Select Cities1910 pop.1915Mortality Rate1918Mortality Rate1919Mortality RateRatio of 1918 and1915 RatesRochester, N.Y.218,149121.8522.7152.84.334San Francisco, Calif.416,912130.6647.7283.35.027Scranton, Pa.129,867223.7985.7247.54.42Seattle, Wash.237,19474.7425.5189.85.745Spokane, Wash.104,40291.9487.4210.75.337St. Louis, Mo.687,029156.7536.5202.33.432St. Paul, Minn.214,744127.8480.6145.93.839Syracuse, N.Y.137,249120.5704.6155.95.818Toledo, Ohio168,497126.8401.0181.93.247Washington, D.C.331,069189.8758.8225.94.012Worcester, Mass.145,986188.9727.1248.93.816City1918 RankNotes: Mortality rates are from Mortality Statistics 1920 and include mortalities from influenza and pneumonia. Mortalities for Dallas andHouston in 1915 are 1916 and 1917 figures, respectively.Table 4: City Influenza MortalitiesRelative to State Mortality Rate (1918)StateAverage of CitiesRelative to StateMichigan0.89Colorado0.95California1.01New na1.13New i1.32Kansas1.58Tennessee1.66Influenza Mortalities and RaceInfluenza mortalities by race are availablefor some cities in the United States, thoughthe racial breakdown is not as detailed as themodern-day mortality statistics. Mortalitystatistics for 1918 are provided on the basis ofwhite and nonwhite. Table 5 presents a breakdown of white and nonwhite mortality rates(per 100,000 for each racial group) for 14 U.S.cities. For each racial group, influenza mortality rates for 1915 are also included; so, acomparison can be made between a pandemicyear and a nonpandemic year.Looking at the first six columns of Table 5, itis evident that nonwhite mortalities from influenza are higher than white influenza mortalities in both pandemic and nonpandemic years(except for Kansas City in 1918). However,white influenza mortalities as a percentage ofnonwhite mortalities were less in 1915 than in1918. Thus, white influenza mortality rateswere typically less than nonwhite mortalityrates, but this difference decreased in the influenza pandemic of 1918. As a group, whiteswere struck relatively harder by the influenzapandemic than nonwhites. This is supportedby the last two columns of Table 5 that show1915 influenza mortality rates relative to 1918mortality rates for each racial group. Clearly,across the 14 cities listed, the relative differencein mortality rates for the two years is larger forwhites than it is for nonwhites.It is reasonable to assume that racial differences in influenza mortality rates are reflecting, to some degree, differences in population13
Table 5: Influenza Mortality Rate By Race and City, 1915 and 19181CityBirmingham, Ala.2345678White Mortality Rate1918NonwhiteMortalityRate 1918White,% ofNonwhite1918WhiteMortality Rate1915NonwhiteMortalityRate1915White,% ofNonwhite1915White1915, % ofWhite1918Nonwhite1915, %of 0.4%Atlanta, olis, Ind.440.6615.271.6%132.9264.550.2%30.2%43.0%Kansas City, ille, Ky.1,012.31,015.599.7%111.2369.630.1%11.0%36.4%New Orleans, more, is, ille, las,* n,* k, , ton, lity rates for Dallas and Houston are for 1916 and 1917, respectively, not 1915.Table 6: Location and Race, 1890-1990YearWhite as a Percentof U.S. Urban PopulationNonwhite as a Percent ofU.S. Urban PopulationPercent of White PopulationThat Is UrbanPercent of Nonwhite PopulationThat Is 8%23.12%72.02%88.21%Note: Population data are from Historical Statistics of the United States, U.S. Census.14density (as seen in Table 2) and geography (asseen in Table 4). To confirm this hypothesis,data on white and nonwhite population, aswell as rural and urban place of residence, weregathered for several decennial Census years.These data are shown in Table 6.In 1910, the great majority of the urbanpopulation (having a higher population densitythan rural areas) in the United States waswhite (over 90 percent). This can explain whywhites as a group had a much larger increase ininfluenza mortalities during the pandemic thandid nonwhites.What does this imply if an influenza pandemic struck today? The last two columns ofTable 6 reveal that the nonwhite population inthe United States has become much more urban(27 percent in 1910 and 88 percent in 1990)compared with the white population (49 percentin 1910 and 72 percent in 1990). However,
the fact that both racial groups are becomingmore urban does not bode well for either groupbecause population density will certainly be asignificant determinant of mortality. A modernday pandemic may result in greater nonwhitemortality rates because a greater percentage ofthe nonwhite population in the United Stateslives in urban areas.Of course, race and place of residence (andpopulation density) are not the only factorsthat are likely to influence mortality rates.Access to health care is likely to be critical(assuming health professionals themselvesare not decimated by the pandemic). So, itstands to reason that mortality rates in urbanareas may be somewhat mitigated given therelatively greater access to health care than inrural areas. Ability to pay, which relates toincome, may also be important. Urban areas,on average, tend to have greater incomes, butthis is an average and ignores those individualswith low incomes in urban areas who cannotafford health care. The ability of free clinicsand emergency rooms to remain open duringa pandemic will be crucial to the treatment oflower-income individuals. The final sectionof this report discusses the implications fora modern-day pandemic and will expand onthese points.Pandemic Mortalities in EighthFederal Reserve District StatesData on mortalities from 1915 to 1920 forcities located in Eighth Federal Reserve DistrictStates are shown in Table 7. The first columnof data contains mortality rates per 100,000population (from Mortality Statistics 1920).These data are also shown in Figure 1. Thenumber of deaths (found by multiplying therate in the first column by city population) isshown in the second column. The third column contains “normal” influenza deaths andwas calculated by subtracting the number ofexcess deaths in each year from the total number of deaths shown in column 2 (see notes toTa
Central Power troops died as a result of the influenza pandemic rather than combat.11 Although combat deaths in World War I did increase the mortality rates for participating countries, civilian mortality rates from the influenza pandemic of 1918 were typically much higher. For the United States, estimates