Transcription
TMforRapid Response Systems
RRSOverview What is the Rapid Response System? The Rapid Response System (RRS) is theoverarching structure that coordinates all teamsinvolved in a rapid response call What is TeamSTEPPS?Mod 1205.2 Page 2Page The Agency for Healthcare Research and Quality’scurriculum and materials for teaching teamwork toolsand strategies to healthcare professionals This module of TeamSTEPPS is for RRSTEAMSTEPPS 05.2
RRSOverview What is the Rapid Response Team?Mod 1305.2 Page 3Page RRS has several parts, one of them being theRapid Response Team (RRT) A RRT – known by some as the MedicalEmergency Team – is a team of clinicians whobring critical care expertise to the patient’s bedsideor wherever it is needed (IHI, 2007)TEAMSTEPPS 05.2
RRSWhy Should You Care? People die unnecessarily every day in our hospitals It is likely that each of you can provide an example of apatient who, in retrospect, should not have died duringhis or her hospitalization There are often clear early warning signs of deterioration Establishing a RRS is one of the Joint Commission’s2008 National Patient Safety Goals Teamwork is critical to successful rapid response The evidence suggests that RRS work!Mod 1405.2 Page 4PageTEAMSTEPPS 05.2
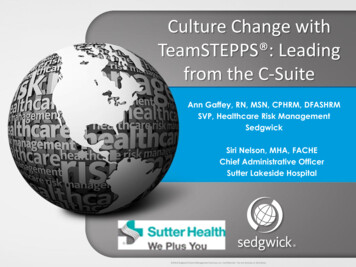
RRSDoes it Work?BeforeAfterNo. of cardiac arrests6322Deaths from cardiac arrest3716No. of days in ICU post arrest16333No. of days in hospital after arrest1363159Inpatient deaths302222Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of amedical emergency team. Medical Journal of Australia. 2003;179(6):283-287.Mod 1505.2 Page 5PageTEAMSTEPPS 05.2
RRSDoes the RRS Work? 50% reduction in non-ICU arrestsBuist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medicalemergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital:preliminary study. BMJ. 2002;324:387-390. Reduced post-operative emergency ICU transfers (58%)and deaths (37%)Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trial of effect of medical emergency teamon postoperative morbidity and mortality rates. Crit Care Med. 2004;32:916-921. Reduction in arrest prior to ICU transfer (4% vs. 30%)Goldhill DR, Worthington L, Mulcahy A, Tarling M, Sumner A. The patient-at-risk team: identifying andmanaging seriously ill ward patients. Anesthesia. 1999;54(9):853-860. 17% decrease in the incidence of cardiopulmonary arrests(6.5 vs. 5.4 per 1000 admissions)DeVita MA, Braithwaite RS, Mahidhara R, Stuart S, Foraida M, Simmons RL. Use of medical emergencyteam responses to reduce hospital cardiopulmonary arrests. Qual Saf Health Care. 2004;13(4):251-254.Mod 1605.2 Page 6PageTEAMSTEPPS 05.2
RRSNQF Safe Practices In 2003, the National Quality Forum (NQF) identified the RRS asa chief example of a team intervention serving the safe practiceelement of Team Training and Team Interventions RRSs are viewed as an ideal example of safe practices inteamwork meeting the objective of establishing a proactivesystemic approach to team-based care In 2006, the NQF updated their Safe Practicesrecommendations Mod 1705.2 Page 7PageNQF continues to endorse RRSs and concludes thatannually organizations should formally evaluate theopportunity for using rapid response systems to address theissues of deteriorating patients (NQF, 2006)TEAMSTEPPS 05.2
RRSJoint Commission2008 National Patient Safety Goal Goal 16: Improve recognition and response tochanges in a patient’s condition Mod 1805.2 Page 8Page16A. The organization selects a suitable method thatenables health care staff members to directly requestadditional assistance from a specially trainedindividual(s) when the patient’s condition appears to beworseningTEAMSTEPPS 05.2
RRSImplementation When implementing RRS, the Institute for HealthcareImprovement (IHI) recommends: Engaging senior leadership Identifying key staff for RRTs Establishing alert criteria and a mechanism for calling the RRT Educating staff about alert criteria and protocol Using a structured documentation tool Establishing feedback mechanisms Measuring effectiveness RRS can be customized to meet your institutions’ needsand resourcesMod 1905.2 Page 9PageTEAMSTEPPS 05.2
RRSRRS StructureMod 110Page05.2 Page 10TEAMSTEPPS 05.2
RRSActivator(s) Activators can be:Mod 111Page05.2 Page 11 Floor staff A technician The patient A family member Specialists Anyone sensing the acutedeteriorationTEAMSTEPPS 05.2
RRSResponder(s) Responders come to the bedsideand assess the patient’s situation Responders determine patientdisposition, which could include: Transferring the patient to anothercritical care unit (e.g., ICU or CCU)A handoff back to the primarynurse/primary physicianRevising the treatment plan Activators may becomeResponders and assist instabilizing the patientMod 112Page05.2 Page 12TEAMSTEPPS 05.2
RRSActivators & Responders Activator(s) are responsible for calling the Responder(s) ifa patient meets the calling criteria Responders must reinforce the Activator(s) for calling:“Why did you call?” vs. “Thank you for calling. What is the situation?”Remember: There are no “bad calls”!Mod 113Page05.2 Page 13TEAMSTEPPS 05.2
RRSSupport:Quality Improvement & Administration The Quality Improvement (QI)Team supports Activators andResponders by reviewing RRSevents and evaluating data forthe purpose of improving RRSprocesses The Administration Team ofthe RRS brings organizationalresources, support, andleadership to the entire RRSand ensures that changes inprocesses are implementedif necessaryMod 114Page05.2 Page 14TEAMSTEPPS 05.2
RRSLet’s Watch the RRS in ActionMod 115Page05.2 Page 15TEAMSTEPPS 05.2
RRSTeamwork & RRS The RRS has all these barriers to effective care:ConflictLack of tation of cuesLack of role clarityInconsistency in team membershipLack of timeLack of information sharingMod 116Page05.2 Page 16TEAMSTEPPS 05.2
RRSNecessary Teamwork SkillsMod 117Page05.2 Page 17TEAMSTEPPS 05.2
RRSInter-Team Knowledge Supports effective transitions in carebetween units Is a prerequisite for transition support(or “boundary spanning”) Consists of understanding the roles andresponsibilities of each team within the RRSMod 118Page05.2 Page 18TEAMSTEPPS 05.2
RRSInter-Team KnowledgeActivator needs ICU requires Administrationrequires Patient needs Respondersneed ICU requires In the RRS, inter-teamTeamwork Activators must knowtlity enua mQ oveTEAMSTEPPS 05.2prMod 119Page05.2 Page 19Imthe roles andresponsibilities ofResponders andvice versaivsserndpoestcAortaRknowledge means allRRS members possessa shared understandingof the roles andresponsibilities of allother membersmdAniottrasiin
RRSTransition Support(“Boundary Spanning”) Requires inter-team knowledge Combines monitoring transitions in care andproviding backup behavior when needed Provides role support Mod 120Page05.2 Page 20Example: Activator becoming ResponderTEAMSTEPPS 05.2
RRSTransition Support(“Boundary Spanning”) Manage dataserndpoestivcARrsoat Monitor transitions Educate staff onsituation and roles Ensure data recordingprtlity enua mQ oveImMod 121Page05.2 Page 21mdAniottrasiinTEAMSTEPPS 05.2 Assist in roleorientation
RRSExample of One RRS Activators call Responders using a pager Who are the Responders?Mod 122Page05.2 Page 22 ICU Physician ICU Charge Nurse Nurse Practitioner (if available) RRS coordinator Transportation service For Pediatric Unit, chaplain’s office,security, and respiratory therapist are also includedTEAMSTEPPS 05.2
RRSExample of One RRS (continued) Training Includes direct teaching modules on rapid responseand practice using Situation-Background-AssessmentRecommendation (SBAR) Online training modules Single-discipline training sessions Data Collection includes reporting:Mod 123Page05.2 Page 23 Who called the response team and what criteria were used? Who responded and in what timeframe? What was done for the patient? What are the top 5 diagnoses seen in the RRS?TEAMSTEPPS 05.2
RRSExample of Another RRS Activators call Responders usingan overhead page and a pager Family members areconsidered Activators Responders include:Mod 124Page05.2 Page 24 Nursing staff Respiratory care staff ICU staffTEAMSTEPPS 05.2
RRSExample of Another RRS (continued) Training In-class sessions Simulation center Interdisciplinary training in same location Data collectionMod 125Page05.2 Page 25 Event debriefing Task-oriented checklist by rolesTEAMSTEPPS 05.2
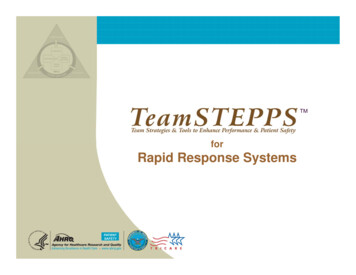
RRSExample of Another RRS (continued)Nursing TasksCompleted?1. Check the patient’s pulse.;2. Obtain vital signs. 3. Place the pulse oximeter. 4. Assess patient’s IVs. Respiratory Therapist TasksMod 126Page05.2 Page 26Completed?1. Assess the airway. 2. Count the respiratory rate. 3. Assist ventilation. 4. Check the patient’s pupils. TEAMSTEPPS 05.2
RRSExercise I:Let’s Identify Your RRS StructureThink about the four components of the RRS:Activators, Responders, QI and Administrative Who are the Activators? What are the alert criteria? How are Responders called?What do Activators do onceResponders arrive? Mod 127Page05.2 Page 27Who are the Responders? How many Responders arrive to a call? What is each person’s role?TEAMSTEPPS 05.2
RRSExercise I (continued):Let’s Identify Your RRS Structure What are the common challenges facing your RRS? Are there challenges during:Mod 128Page05.2 Page 28 Patient deterioration? System activation? Patient handoffs? Patient treatment? Evaluation of the response team?TEAMSTEPPS 05.2
RRSRRS ExecutionMod 129Page05.2 Page 29TEAMSTEPPS 05.2
RRSDetectionTools/StrategiesHUDDLESTEPActivator seessigns of acutedeteriorationbefore ECTIONMod 130Page05.2 Page 30TEAMSTEPPS 05.2
RRSDetection: STEP AssessmentUse your institution’sdetection criteria forRRS activationIs it time toactivate theRRS?Mod 131Page05.2 Page 31TEAMSTEPPS 05.2
RRSWhere can Detection occur? Detection can occur from a variety ofsources or concernsMod 132Page05.2 Page 32TEAMSTEPPS 05.2
RRSRRS ActivationCommunicationTools/StrategiesSBARMod 133Page05.2 Page 33TEAMSTEPPS 05.2
RRSRRS Activation: SBAR SBAR provides a framework for team members toeffectively communicate information to one another Communicate the following information: Situation―What is going on with the patient? Background―What is the clinical backgroundor context? Assessment―What do I think the problem is? Recommendation/Request―What would Irecommend/request?Remember to introduce yourself Mod 134Page05.2 Page 34TEAMSTEPPS 05.2
RRSResponse, Assessment & eRespondersanalyzepatient condition;attempt tostabilizeRESPONSE,ASSESSMENT &STABILIZATIONMod 135Page05.2 Page 35Leadership,SituationMonitoring,Mutual Support,Communication,& Inter-TeamKnowledgeRESPONSE,ASSESSMENT &STABILIZATIONTEAMSTEPPS 05.2Tools/Strategies:CommunicationCheck-backCall OutTools/Strategies:Mutual SupportTask AssistanceCUS
RRSResponse, Assessment & StabilizationHuddleDevisecontingencies forsending thepatient to the ICUor other ancillaryunits.Devisecontingencies fora handoff back tothe general carearea (i.e., keepingthe patient incurrent location).Mod 136Page05.2 Page 36TEAMSTEPPS 05.2
RRSResponse, Assessment & StabilizationCUS WordsMod 137Page05.2 Page 37TEAMSTEPPS 05.2
RRSPatient ARI PASS theBATONMod 138Page05.2 Page 38TEAMSTEPPS 05.2
RRSPatient Disposition Disposition can refer to a number of decisions,including:Mod 139Page05.2 Page 39 Transferring the patient to another unit A handoff back to the primary nurse/primaryphysician (i.e., patient stays in same location) A handoff to a specialized team (cardiac team,code team, stroke team, etc) A revised plan of careTEAMSTEPPS 05.2
RRSRRS Transition: I PASS the BATONMod 140Page05.2 Page 40TEAMSTEPPS 05.2
RRSRRS min & QIComponentsevaluateperformanceand assessdata for tionEVALUATIONEVALUATIONMod 141Page05.2 Page 41TEAMSTEPPS 05.2DebriefsSensemakingChecklist
RRSEvaluation: Debriefs Debriefs occur right after theevent and are conducted bythe Responders Debriefs should address:Mod 142Page05.2 Page 42 Roles Responsibilities Tasks Emphasis on transitions incare Achievement of patientstabilizationTEAMSTEPPS 05.2
RRSSystem Evaluation: SensemakingSensemaking Review Sheet1. How did the Activators and Responders react tothis situation?2. When looking at the “big picture,” are there any patterns or trends?Mod 143Page05.2 Page 43TEAMSTEPPS 05.2
RRSSystem Evaluation: SensemakingTools Proactive approaches Failure Modes andEffects Analysis (FMEA)Probabilistic RiskAssessment (PRA) Reactive approaches Root Cause Analysis(RCA)IntegratedSensemaking Approach What can go wrong? What are the consequences? How do things go wrong? How likely are they? What went wrong? Why did it go wrong?Mod 144Page05.2 Page 44TEAMSTEPPS 05.2
RRSLet’s look back at our exampleMod 145Page05.2 Page 45TEAMSTEPPS 05.2
RRSExercise II: RRS Execution Using the scenario provided, identify the five phasesof the RRS and what tools and/or strategies wereused during each phase Detection Activation Response, Assessment, and Stabilization Disposition EvaluationMod 146Page05.2 Page 46TEAMSTEPPS 05.2
RRSExercise III Let’s see if we can identify the tools needed orused in each example Scenario 1 Scenario 2 Scenario 3 Scenario 4 Scenario 5Mod 147Page05.2 Page 47TEAMSTEPPS 05.2
RRSScenario 1The nurse called the RRT to a patient who exhibited a reducedrespiratory rate. The team was paged via overhead page. Withinseveral minutes, team members arrived at the patient’s room; however,the respiratory therapist did not arrive. After a second overhead pageand other calls, the respiratory therapist arrived, stating that he couldnot arrive sooner due to duties in the ICU. This critical team memberdid not ascribe importance to the rapid response call and failed toprovide a critical skill during a rapid response event. As a result, therewas a delay in the assessment of the patient’s airway and interventionpending arrival of the response respiratory therapist.Mod 148Page05.2 Page 48TEAMSTEPPS 05.2
RRSScenario 2The RRT was called for a patient who had a risk of respiratory failure. Thepatient was intubated and transferred to a higher level of care. Response teammembers and the nurse who called the team completed a Call EvaluationForm. The response team members noted that some supplies, such asnonrebreather masks and an intubation kit, were not readily available on thefloor, which resulted in a delay. This delay could have impacted the patient,and it also affected the team members’ ability to return to their patientassignments. The patient’s nurse noted on the form that the response teamseemed agitated by the lack of supplies and the delay. The evaluation formswere sent via interdepartmental mail to the quality department as indicated onthe form. The forms were not collated or reviewed for several weeks. Theanalyst responsible felt that most of the reports prepared in the past were notused by or of interest to management. Several times the agenda item for RRSupdates had been removed from the Quality Council’s meeting agenda due toan expectation that the “Rapid Response System is running fine.”Mod 149Page05.2 Page 49TEAMSTEPPS 05.2
RRSScenario 3A family member noticed the patient seemed lethargic and confused. The family memberalerted the nurse about these concerns. The nurse assured the family member that she wouldcheck on the patient. An hour later, the family member reminded the nurse, who thenassessed the patient. The nurse checked the patient’s vital signs. She did not note anyspecific change in clinical status, though she agreed that the patient seemed lethargic. At thefamily member’s urging, the nurse contacted the physician, but the conversation focused onthe family member’s insistence that the nurse call the physician rather than conveying aspecific description of the patient’s condition. Based on the unclear assessment, the physiciandid not have specific instructions. The physician recommended additional monitoring.Another nurse on the floor suggested calling the RRT, which she heard had helped with thistype of situation on another floor. The first nurse missed the training about the new RRS,which was not discussed in staff meetings. Based on her colleague’s recommendation, thenurse called the RRT via the operator. The overhead page stated the unit where assistancewas needed but not the patient’s room number. The operator forgot to take down all of theusual information because he missed lunch and was distracted. The team arrived on the floorbut had to wait to be directed to the appropriate room. Once there, the RRT received a briefoverview from the nurse, who left the room shortly afterward. The responders conducted anassessment of the patient and identified that the patient was overmedicated.Mod 150Page05.2 Page 50TEAMSTEPPS 05.2
RRSScenario 4The RRT was called to the outpatient (OP) area for a report of a patientwith a seizure. The usual or expected set of supplies was not available forthe team in the OP area. The RRT arrived and assessed the patient. Aspart of the assessment, the team ordered a stat lab. The lab technicianworking with the OP area had not heard of the RRS and refused to facilitatea stat lab because he was unfamiliar with having this need in an OP area.The RRT members were frustrated but did not challenge the lab technician.The patient was taken to the Emergency Department.Mod 151Page05.2 Page 51TEAMSTEPPS 05.2
RRSScenario 5A night nurse noted that a patient who had been on the unit for 2 days seemedmore tired than usual. Although the patient was usually responsive andanimated, she did not seem as responsive during the evening shift. Afterchecking on her twice, the nurse noted that the patient seemed weak andconfused. The nurse called the physician at 3 a.m. and described the patient’sgeneral status change as being “not quite right” but did not provide a detailedreport or recommendation. The physician, frustrated, did not ask probingquestions about the patient. The physician noted that it was 3 a.m., mentionedthat perhaps the patient was tired, and instructed the nurse to monitor thepatient. The next morning, the physician came in to do rounds and could notfind a complete update from the previous evening. Upon assessing the patient,the physician ordered a stat MRI to rule out stroke.The nurse experienced anxiety due to deterioration of patient status andinability to communicate with the physician. The physician was frustrated bynot clearly receiving all of the relevant patient information during the firstphysician-nurse communication. The patient’s stroke remained unidentifiedduring evening shift.Mod 152Page05.2 Page 52TEAMSTEPPS 05.2
TEAMSTEPPS 05.2 Mod 1 05.2 Page 12Page 12 RRS Responder(s) Responders come to the bedside and assess the patient's situation Responders determine patient