Transcription
The North American Neuroendocrine Tumor SocietyConsensus Guidelines for Surveillance and Managementof Metastatic and/or Unresectable Pheochromocytomaand ParagangliomaLauren Fishbein, MD, PhD,* Jaydira Del Rivero, MD,† Tobias Else, MD,‡ James R. Howe, MD,§Sylvia L. Asa, MD, PhD, Debbie L. Cohen, MD,¶ Patricia L.M. Dahia, MD, PhD,# Douglas L. Fraker,MD,**Karyn A. Goodman, MD,†† Thomas A. Hope, MD,‡‡ Pamela L. Kunz, MD,§§ Kimberly Perez,MD, Nancy D. Perrier, MD,¶¶ Daniel A. Pryma, MD,## Mabel Ryder, MD,*** Aaron R. Sasson,MD,††† Michael C. Soulen, MD,‡‡‡ and Camilo Jimenez, MD§§§ABSTRACTThis manuscript is the result of the North AmericanNeroendocrine Tumor Society consensus conference onthe medical management and surveillance of metastaticand unresectable pheochromocytoma and paragangliomaheld on October 2 and 3, 2019. The panelists consistedof endocrinologists, medical oncologists, surgeons,radiologists/nuclear medicine physicians, nephrologists,pathologists, and radiation oncologists. The panelistsperformed a literature review on a series of questionsregarding the medical management of metastatic andunresectable pheochromocytoma and paraganglioma aswell as questions regarding surveillance after resection.The panelists voted on controversial topics, and finalrecommendations were sent to all panel members forfinal approval.Key Words: metastatic pheochromocytoma, metastaticparaganglioma, management, treatment, surveillance(Pancreas 2021;50: 469–493)Pheochromocytomas and paragangliomas (PPGLs) aretumors of the autonomic nervous system found within theadrenal medulla or extra-adrenal paraganglia, respectively.Pheochromocytoma (PCC) and paraganglioma (PGL) occurin 2 to 8 per millionpeople.1 Metastatic PPGL (mPPGL)occurs in up to 15% to 25% of people with primary PPGLand can have a long latency period. Pheochromocytomasand PGLs metastasize to the lymph nodes (80%), bones(71%), liver (50%), and lungs (50%).2 Metastatic diseasecan be diagnosed at the time of the primary tumordiscovery or even as long as 20 years later.3 People withmPPGL have a 5-year survival rate between 50% and70%,4–7 meaning for some individuals, living with mPPGLis a chronic condition, whereas others, unfortunately, willhave progressive disease with a subset of those havingrapidly progressing, very aggressive disease. Furthermore,in some patients, a primary PPGL may occur in a locationwhere surgical resection cannot be accomplished safelyand other therapies are required to control both hormonesecretion and tumor growth. Significant advances inthe diagnosis and treatment of mPPGL have occurredin the last few years, including improved somatostatinreceptor (SSTR)–based nuclear imaging, the first Foodand Drug Administration (FDA)– approved therapy formPPGL, and an increase in clinical trials. Here, we makeexpert recommendations on the diagnosis, management,treatment, and surveillance of metastatic and/orunresectable PPGL.1
From the *Division of Endocrinology, Metabolism,and Diabetes, Department of Medicine, University ofColorado Anschutz Medical Campus, Aurora, CO;†Developmental Therapeutics Branch, National CancerInstitute, National Institutes of Health, Bethesda,MD; ‡Division of Metabolism, Endocrinology, andDiabetes, Department of Internal Medicine, Universityof Michigan, Ann Arbor, MI; §Division of SurgicalOncology and Endocrine Surgery, Departmentof Surgery, University of Iowa Carver College ofMedicine, Iowa City, IA; Department of Pathology,University Hospitals Cleveland Medical Center andUniversity Health Network, Toronto, Case WesternReserve University, Cleveland, OH; ¶Renal Division,Department of Medicine, Perelman School of Medicineat the University of Pennsylvania, Philadelphia, PA;#Division of Hematology and Medical Oncology,Department of Medicine, University of Texas HealthSan Antonio, San Antonio, TX; **Division of Endocrineand Oncologic Surgery, Department of Surgery,University of Pennsylvania and Abramson CancerCenter, Philadelphia, PA; ††Department of RadiationOncology, Icahn School of Medicine at Mount Sinai,New York, NY; ‡‡Department of Radiology andBiomedical Imaging, University of California SanFrancisco, San Francisco, CA; §§Division of Oncology,Department of Medicine, Yale School of Medicine,New Haven, CT; Department of Medical Oncology,Dana-Farber Cancer Institute, Harvard Medical School,Boston, MA; ¶¶Division of Surgery, Departmentof Surgical Oncology, The University of Texas MDAnderson Cancer Center, Houston, TX; ##Departmentof Radiology and Abramson Cancer Center, PerelmanSchool of Medicine at the University of Pennsylvania,Philadelphia, PA; ***Endocrine Oncology Tumor Group,Division of Medical Oncology, Mayo Clinic, Rochester,MN; †††Division of Surgical Oncology, Department ofSurgery, Stony Brook University Medical Center, StonyBrook, NY; ‡‡‡Department of Radiology, University ofPennsylvania, Philadelphia, PA; and §§§Departmentof Endocrine Neoplasia and Hormonal Disorders,The University of Texas MD Anderson Cancer Center,Houston, TX.T.E. discloses consulting on an advisory board for HRA Pharma and Corcept Therapeutics, andparticipates in institutional contracted clinicalstudy for Merck and Co, Inc, Corcept Therapeutics,and Strongbridge Biopharma. J.R.H. disclosesNational Institutes of Health grant fundingunrelated to this project and royalties for abook on endocrine surgery unrelated to thisproject. S.L.A. discloses board membership forLeica Biosystems, consults for PathAI, and hasreceived speaker payment from Med LearningGroup. P.L.M.D. discloses support to travel toNorth American Neuroendocrine Tumor Society,is a full-time faculty member at the Universityof Texas Health San Antonio, and received grantfunding for other projects from the NationalInstitutes of Health and Alex’s Lemonade StandFoundation. T.A.H. discloses consulting for Ipsenand pending grant from Advanced AcceleratorApplications. P.L.K. discloses consulting forAdvanced Accelerator Applications and Ipsenand has grants from Advanced AcceleratorApplications, Ipsen, Brahms (Thermo FisherScientific), Lexicon Pharmaceuticals, and Xencor.K.P. discloses serving one time on an advisoryboard panel for Celgene and Eisai, both unrelatedto this manuscript. D.A.P. discloses consultinghonoraria from Siemens, Progenics, Bayer, Ipsen,Fusion, 511 Pharma, and Actinium, and receivingresearch funding from Siemens, Fusion, NordicNanovector, 511 Pharma, and Progenics. A.R.S.discloses being part owner of a start-up calledSanguine Diagnostics and Therapeutics and alsolecturing for Novartis pending. M.C.S. disclosesconsulting fees from Guerbet LLC, Genentech,and Instylla, and grant funding from Guerbet LLCand Boston Scientific. The other authors declareno conflict of interest.Copyright 2021 Wolters Kluwer Health, Inc. All rightsreserved. DOI: 10.1097/MPA.0000000000001792Address correspondence to: Lauren Fishbein, MD, PhD, Division of Endocrinology, Metabolism, andDiabetes, Department of Medicine, Universityof Colorado Anschutz Medical Campus, 12801E 17th Ave, MS 8106, Aurora, CO 80045 (e‐mail:lauren.fishbein@cuanschutz.edu).2
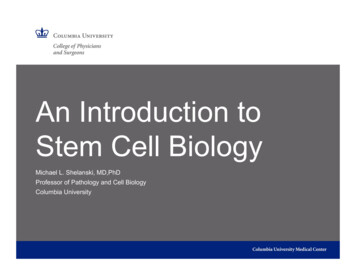
Pancreas Volume 50, Number 4, April 2021Fishbein et alMATERIALS AND METHODSMATERIALS AND METHODSThe expert panel for the North American NeuroendocrineThe expert panel for the North American Neuroendocrine TuTumorSocietymPPGLguidelinesconsisted18mor SocietymPPGLguidelinesconsistedof 18 ogists,4medicalcluding 3 endocrinologists, 4 medical oncologists, 4 surgeons, 2radiologists/nuclearmedicinephysicians, 1 nephrologist,1 patholooncologists,4 surgeons,2 diologist,1radiationoncologist,and1 endophysicians, 1 nephrologist, 1 pathologist, 1 interventionalcrine cancer researcher. The panelists met in person in Octoberradiologist,1 radiationoncologist,and 1ofendocrine2019 and debatedall topicsthrough a seriesshort presentationscancerresearcher.Thepanelistsmetin personin Octoberthat reviewed the key literature. After the toaddressareasofcontroversy2019 and debated all topics through a series of shortand/or those withlimiteddata. idelines,literature.afterAftertheany abstentions, we defined “consensus” as no more than 1 signedtional vote and “significant majority” as 75% agreement or greater.toaddressareas ofand/or thosewith limitedThefull documentandcontroversythe recommendationsin the al.data. For these guidelines, after excluding any abstentions,we defined “consensus” as no more than 1 oppositionalvote and “significant majority”as 75% agreement orRESULTSgreater. The full document and the recommendationsinInheritedthe documentwere circulatedto the panelists forPredispositionto PPGLfinal approval.Up to 40% of PPGL arise in patients with germline pathogenic variants in at least 1 of 12 well-studied susceptibility genesleading to predisposition syndromes (Table 1).8 The classic cancerRESULTSpredisposition syndromes associated with PPGL are NeurofibroInheritedPredispositionto PPGLmatosis type1 (NF1), MultipleEndocrine Neoplasia type 2Upto 40%andof PPGLin patientswith germline(MEN2),von ariseHippel–Lindau(VHL)disease caused bygermline pathogenicin NF1,and VHL, respectively.pathogenicvariantsvariantsin at least1 ofRET,12 well-studiedThese syndromes most often are associated with secreting unilatsusceptibility genes leading to predisposition syndromeseral or bilateralPCC. Metastatic disease is rare in patients with8(Tableclassic ociatedPPGL.Although PPGLtumors rare in patientsNF1,can occur in typeup to112% ofNF1-associatedPPGL.9 HereditarySyndrome(NF1),Multiple EndocrineNeoplasiaPGL-PCCtype 2 (MEN2),and iscaused by pathogenic germline variants in the Succinate Dehydrovon Hippel–Lindau (VHL) disease caused by germlinegenase Subunit (SDHx) genes (SDHA, SDHB, SDHC, SDHD, andpathogenicvariantsin NF1,RET, andVHL,respectively.SDHAF2), andcombined,the SDHxgenesaccountfor the largestThese syndromes most often are associated with secretinggroup of hereditary PPGL. Pathogenic germline variants in any ofunilateralbilateralPCC. toMetastaticdiseaseis rareinthese genesorarepredisposedPPGL GL.Althoughpenetrancewithbasedon theandgeneand a smaller butincreasedrisk ofclear cellrenal cell(RCC) withand gastrointestinalstromalPPGLtumorsare carcinomarare in patientsNF1, mPPGL can10,11MetastaticPPGLisrareinSDHC-,tumors.9 SDHD-, andoccur in up to 12% of NF1-associated PPGL. HereditarySDHAF2-associated PPGL, but the risk is higher with SDHB12 pathogenic germlinePGL-PCCand SDHA (12% by the age(25%–50%Syndromeby the age isof caused60 years)by13 Succinate Dehydrogenase Subunit (SDHx)variantsin theof 70 years).There are other susceptibility genes that are significantly (SDHA,less frequentlymutatedin patientswith PPGLincludinggenesSDHB, SDHC,SDHD,and encombined, the SDHx genes account for the largestproposedgroupas susceptibility genes, including MDH2, PHD1, PHD2, nany ofSLC25A11, GOT2, DLST, and DNMT3A (as well as EPAS1/HIF2A14–22thesegenesare predisposedtorarityPPGLofwithvaryingage-withas somaticmosaic).Given thePPGLassociated23all of thesegenes, the trueriskonof mPPGLis lessunderstood.relatedpenetrancebasedthe geneandwella smallerbutOf patientsmPPGL,approximately40% to45%andwillincreasedrisk ofwithclearcell renalcell carcinoma(RCC)have a known heritable pathogenic variant. The most commonly ed gene with stromalmPPGL isSDHB (over 40%of mPPGLcases),isin SDHC-,andwithSDHAF2-associatedPPGL,butraremPPGLcan beSDHD-,associatedsporadic tumors andwith any24,25of thesusceptibilitygenesalbeitat a lowerbuttheotherrisk ishigher withSDHB(25%–50%byrates.the age Theknowledgeof theandgermlinevariant,thereof,13willof60 years)12SDHApathogenic(12% by theage orof lack70 years).have implications for surveillance of the patient and identificationThereothersusceptibilitygenesthatare significantlyof theirareat-riskfamilymembers. If thepatientcarriesa susceptibilitylessmutatedpatientsPPGL includinggenefrequentlypathogenic variant,theyinmaybe at riskwithfor developingadditionalmalignanciesMAX,or otherthereforerequiringTMEM127,andconditions,FH. Additionalgeneshaveongoingbeen monitoring, and theirblood relatives shouldoffered site-specificgeneticproposedas susceptibilitygenes,beincludingMDH2, PHD1,testing. If the blood relative tests positive for the known familial pathPHD2,GOT2,shouldDLST, beandscreenedDNMT3Afor(aslifewellogenic KIF1B,variant,SLC25A11,that individualfor14–22asEPAS1/HIF2A as tumorssomaticmosaic).Given theguidelines,rarity ofsyndrome-associatedbasedon syndrome-specific26–29which associatedare outside thescopemanuscript.PPGLwithallofofthisthesegenes, the true risk ofmPPGL is less well understood.23RecommendationWe recommendthat allpatients with40%primaryPPGLOf patientswith mPPGL,approximatelyto 45%willormPPGLhave clinicalgermlinegenetic variant.testing andhavea knownheritablepathogenicTherecommendmostfamily cascade testing if the patient carries a susceptibility genecommonlyassociatedgene with mPPGL is SDHB (overpathogenic variant(consensus).TABLE 1. Inherited Genetics of PPGLGeneSyndromeRisk of PPGLPrimary PPGL LocationRisk of mPPGLOther Associated FeaturesPCC (rare casereports of PGL) 12%Neurofibromas, Lisch nodules,café au lait spots, opticgliomas, skeletal dysplasiaRCC (clear cell type), pancreaticNETs, hemangioblastomasof the CNS including retinaMedullary thyroid cancer,primary hyperparathyroidismRCC (clear cell type), GISTNF1Neurofibromatosistype 11%–13%VHLvon Hippel–Lindausyndrome20%PCC (bilateral) (rarecase reports of PGL) 5%RETMultiple EndocrineNeoplasia type 2Hereditary PGL-PCCsyndromeHereditary PGL-PCCsyndromeHereditary PGL-PCCsyndromeHereditary PGL-PCCsyndromeHereditary PGL-PCCsyndrome50% 5%SDHA: 10%PCC (bilateral) (rarecase reports of PGL)SDHA: PGL, PCCSDHA: 12%SDHB: 25%SDHB: PGL, HNGPL, PCCSDHB: 25%–50% RCC (clear cell type), GISTSDHASDHBSDHC: HNPGL (unifocal),thoracic PGLSDHDSDHD: 45%SDHD: HNPGL (multifocal),PGL, PCCSDHAF2SDHAF2: low SDHAF2: HNPGL(multifocal)TMEM127LowPCC, PGL less commonMAXUnknownPCCFHHereditary leiomyomatosis LowPGLand RCC syndromeSDHCSDHC: lowSDHC: 5%RCC (clear cell type), GISTSDHD: 5%–8% RCC (clear cell type), GISTSDHAF2: lowRCC (clear cell type), GIST 5%UnclearMay be highRCCRCC (papillary type), cutaneousleiomyomas, uterine fibroidsGIST indicates gastrointestinal stromal tumor.470www.pancreasjournal.com 2021 Wolters Kluwer Health, Inc. All rights reserved.Copyright 2021 Wolters Kluwer Health, Inc. All rights reserved.3
40% of mPPGL cases), but mPPGL can be associated withsporadic tumors and with any of the other susceptibilitygenes albeit at a lower rates.24,25 The knowledge ofthe germline pathogenic variant, or lack thereof, willhave implications for surveillance of the patient andidentification of their at-risk family members. If the patientcarries a susceptibility gene pathogenic variant, they maybe at risk for developing additional malignancies or otherconditions, therefore requiring ongoing monitoring, andtheir blood relatives should be offered site-specific genetictesting. If the blood relative tests positive for the knownfamilial pathogenic variant, that individual should bescreened for life for syndrome-associated tumors based onsyndrome-specific guidelines, which are outside the scopeof this manuscript.26–29RecommendationWe recommend that all patients with primary PPGLor mPPGL have clinical germline genetic testing andrecommend family cascade testing if the patient carries asusceptibility gene pathogenic variant (consensus).DEFINITION OF METASTATIC PCC/PGLThe definition of mPPGL is the identification of tumorspread to a location that does not normally haveparaganglionic tissue.1 Only 3 such sites have beenproven to definitively qualify as having no paraganglionictissue, including bone, brain, and lymph node; however,metastatic disease can involve any organ.Primary PGLs can occur almost anywhere in the body.The distinction between multifocal primary PPGLand metastatic spread of a PPGL is important foroptimal patient management. Patients with hereditarypredisposition to PPGL are likely to have multifocalprimary tumors, and risk for metastatic disease variesdepending on the gene. For example, SDHD pathogenicvariant carriers have high incidence of multifocal primaryPPGL, which are usually multiple head and neck PGLs(HNPGLs) but can be anywhere along the parasympatheticand sympathetic chain from skull base to pelvis, andlow risk for metastatic disease.10 As such, patients withmultifocal primary tumors can often be managed withsurgical resection, local therapy, or active observation.When the multifocal disease is within organs such as lungor liver, it may be more difficult to distinguish primary frommetastatic disease.30 Interestingly, for academic purposes,the extent or burden of disease does not determine if thelesions are metastatic or multifocal. Instead, there aresome other factors that might help distinguish the two.For example, those with multifocal disease and sporadicPPGL (where there is no known hereditary predispositiongene pathogenic variant) are more likely to have metastaticdisease. In addition, primary pulmonary PGLs tend tobe found centrally, whereas a peripheral lesion is morelikely to be metastatic; similarly, primary paraganglias inthe liver are most commonly found in or near the hilumof the liver.31 In addition, there are some morphologicmarkers that may be helpful in the distinction (seepathology discussion later). However, for clinical care,although the location within the organ and molecularand histopathologic markers may be useful to distinguishbetween multifocal and metastatic disease in theselocations, this distinction may not matter, especially whenthe disease is unresectable (recommendation: significantmajority). For clinical care purposes, any evidence of PPGLtumor to nonprimary tumor sites can be considered asmetastatic disease (recommendation: significant majority).In some cases, recurrence in the surgical bed can occurafter resection of a PPGL. Most often, this is because oftumor spillage or incomplete resection with regrowthof residual tumor. However, especially in patients withgermline predisposition to these lesions, it is alsopossible that it represents new disease arising in nearbyparaganglia or residual adrenal tissue. This explainswhy recurrence seems to be more common in patientswith MEN2 or VHL.32–36 Regrowth or recurrence in thesurgical bed should not be identified as mPPGL. However,management of recurrence can be just as complex as formetastatic disease, particularly when a lesion is deemedsurgically unresectable.PATHOLOGY OF METASTATIC PCC/PGLThe histologic morphology of PPGL that will give riseto metastasis is usually similar to that of nonmetastaticlesions. These tumors are composed of solid nests ofround to oval cells that are known as “zellballen.” Theintervening stroma is usually highly vascular. The tumorcells have abundant granular amphophilic or basophiliccytoplasm; in some tumors, the cells are more elongatedand almost spindle shaped. Some tumors have uniquemorphology: tumors associated with VHL disease havemore prominent clear cytoplasm and stromal edema,37and those associated with SDHx disease may have moreprominent and abundant granular eosinophilic cytoplasm.The nuclei vary from uniform with vesicular chromatin toatypical with hyperchromasia; mitoses are generally scarceand necrosis is not usually a feature of these tumors.The PPGL tumor cells have reactivity for neuroendocrinemarkers including nuclear INSM1 and cytoplasmicsynaptophysin and chromogranin, but unlike epithelialneuroendocrine tumors (NETs), they are negative forkeratins. Pheochromocytomas and PGLs usually express4
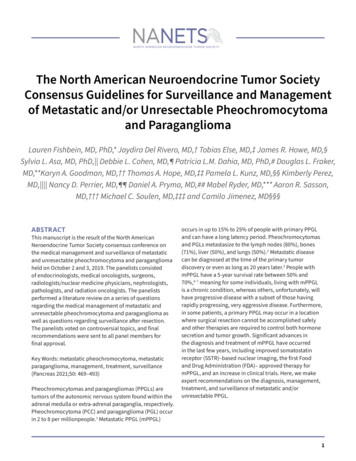
Pancreas Volume 50, Number 4, April 2021Fishbein et altyrosine hydroxylase, if from sympathetic chain, andNeither PASS nor GAPP incorporates molecular data, suchnuclearGATA3, and there is a network of scattered S100as SDHB germline pathogenic variants, which is an important cor45positivecells.A recent third proposal attemptedrelate of sustentacularmetastatic behavior.to address this by combining the PASS and GAPP scores with46SDHB immunohistochemistry,lossof SDHBImmunohistochemistrycan bebecauseused tosupporttheimmunoreactivity suggests a mutation in any one of the SDHx genes.diagnosisof mPPGL versus multifocal primary disease,However, this system has not yet been clinically validated, and italthoughtherearethatno firmcriteria.Both primary andis important to noteSDHBimmunohistochemistrycan be in47congruent intumorssome cases.Giventhis, therewas no consensus thatmetastaticstainforINSM1,synaptophysin,SDHB immunohistochemistryshould be routinelydoneon allchromogranin,and tyrosine hydroxylase,as wellas nuclearPPGL pathology specimens. In North America, clinical geneticGATA3. However, primary tumors usually have numeroustesting almost always is covered by medical insurance and is moresustentacularcells that stain intenselyfor S100reliable than immunohistochemistry.If clinicalgeneticprotein,testing forSDHB pathogenicvariantscannotbe donelackfor thesesome highlyreason,whereasmetastaticfoci edasanalternative.specialized and unique structural stromal cells thatIn summary, the pathology of mPPGLs is poorly documented.theoretically should not travel with the tumor cells toThe literature is confoundedby mostly retrospective studies with38metastaticfoci.time,short follow-upwhich can be problematic given the long latency for developing metastatic disease in many patients. Furtherreportsto considerpossibilityof multifocalItmore,is illprimary disease in patients with genetic predisposition to the develgive rise to metastatic disease from ones that will notopment of these tumors. Prospective studies are needed to assessmetastasize.The abilityto predictscoringmetastasisfromsome of the proposedhistopathologicsystems,and the future may requirea combinationof histopathologyknowledgeexaminationof aprimary tumoris genepathogenicvariantsandsomaticsingle marker has been shown to predict the developmentgenetic results, the latter of which are not yet used routinely in theof metastatic disease. In other NETs, the Ki-67 proliferationclinical setting (see section Tumor-Associated (Somatic) Genetics).index can be used to characterize the aggressive potentialClinicalof rshowever, thewithPPGL is notandSurvival39known. In The Cancer Genome Atlas study, Ki-67 proteinAs outlined previously, PPGL is classified into eithernonmetastasized and metastasized tumors, but histologic featuresexpression by immunohistochemistry was performed onare not reliable indicators. However, predicting the likelihood ofametastaticsubset of62 primary PPGL cases and correlated with thedisease remains an important question when encounterpresenceofmetastaticdisease,follow-uping patients witha primaryPPGL butas itlong-termwill stronglyinfluencepatientsurvival, initialclinicaland40 presurgical(eg,atwasunavailablefor mostcases.Therefore, evaluationit is xtentofmetasthis time if Ki-67 index is predictive of aggressive diseasetasis), as well as follow-up care. Prognostic parameters regarding(recommendation:consensus). No definitive studies insurvival of patients with mPPGL can provide important informaPPGLexist,andtherefore,a recommendationforofcutoffstion, particularly when decidingon the aggressivenesstherapy,ofwhichindexrangescannotfrom anbeactiveobservation approach to surgical reKi-67made.section to antineoplastic therapy.The rationale for determining metastatic potential before surSeveral studies have proposed histopathologiccriteriagery is that it might influence the surgical approach.48 The of metastasis could make a surgery either more inclusive, includingmetastasectomy,or less(Tableaggressive,focusingon debulking.metastaticdisease2), butthe resultshave nceonbeen controversial. The Pheochromocytomatheof decisionthewhether, and to what degree, to conduct postsurgical evaluation forAdrenal Gland Scaled Score (PASS) is a system based onthe presence of metastasis, and on how closely a patient will need toarchitecturecellulartomorphology,necrosis,be followed. Itandis importantkeep in mind, invasion,however, thatthe majorityproliferation,of PPGL do notmetastasize,a full imagingandwherea score andlesstherefore,than 4 supposedlyevaluation,such as awithstagingprocedure,spread.is neither41 necessarynor jusisnot associatedmetastaticThis scoringtified for every single patient with primary PPGL.system has limitations. First, it was designed specificallyPresurgical tumor characteristics that make metastatic disforPCCsareandwastumornot validatedforforPGLs.Second,easeadrenalmore likelylargesize ( 5 cmPCCs, 4 cm42large vessel invasion,extra-adrenallocation, anditforisPGLs),subjectgrossto interobservervariabilityand, therefore,43,49germlinepredispositionan SDHB pathogenicvariant.Alhasnot provento be withreproducible.Third, thereare somethough these characteristics are not statistically significant inintuitive inconsistencies. For example, all tumors arepredicting biological behavior in all retrospective analyses, the majoreithergradedas monotonouswhen theconfernucleia areblandity of studiessuggestthat these of SDHB pathogenichoodmetastatic tumors.ornotofmonotonouswhenthey havepleomorphicnuclei.variants havepleomorphisman overall increasedrisk a worsetumor,ease of approximately 25% to 50%,12 yet it must be noted that lessthan half of individuals with mPPGL have an SDHB pathogenicTABLE 2. Histopathologic Criteria to Predict Risk of Developing Metastatic DiseaseScoring SystemPASS (Range, 0–20)GAPP (Range, 0–10)ArchitectureLarge nests or diffusegrowth2CytologyHigh cellularityCellular monotonySpindle cellsNuclear pleomorphismNuclear hyperchromasiaVesselsTumor capsule (if present)Periadrenal adipose tissueFocal or confluent necrosis 3/10 High-power fieldsAtypical mitoses22211112222InvasionNecrosisMitosesKi-67 labeling indexCatecholamine typeSummary score interpretationPotential for clinicallymalignant behavior 4ZellballenLarge irregular nestsPseudorosettesLow cellularity ( 150 cells/10 mm2)0110Moderate cellularity (150–250 cells/10 mm2)1High cellularity ( 250 cells/10 mm2)Vascular or capsular21Comedo necrosis2 1%1%–3% 3%Epinephrine type (E or E NE)Norepinephrine type (NE or NE DA)Nonfunctioning typeWell-differentiatedModerately differentiatedPoorly differentiated0120100–23–67–10E, epinephrine; NE, norepinephrine; DA, dopamine.472www.pancreasjournal.com 2021 Wolters Kluwer Health, Inc. All rights reserved.Copyright 2021 Wolters Kluwer Health, Inc. All rights reserved.5
yet profound pleomorphism receives a lower score thanmonotony (1 vs 2 points), the latter of which is a feature ofthe majority of tumors.The Grading System for Adrenal Pheochromocytomaand Paraganglioma (GAPP) was designed to also includeextra-adrenal tumors to overcome 1 limitation ofPASS.43 In addition to histologic and cytologic features,it incorporates the degree of tumor cell proliferationusing immunohistochemistry for the Ki-67 antigen thatis expressed in replicating nuclei, and it has the addedadvantage of determining the catecholamine profile.This grading system classifies tumors as score of 0 to10; well-differentiated tumors have a score of 2 or less,moderately differentiated tumors are scored 3 to 6, andpoorly differentiated tumors have scores of 7 or greater.43The risk of metastasis correlates with score, and the timeto metastasis inversely correlates with score, consistentin a separate retrospective cohort study.44 However, themorphologic feature points also have a lack of clarityregarding definitions. Furthermore, the system has not yetbeen clinically validated in prospective studies.Neither PASS nor GAPP incorporates molecular data,such as SDHB germline pathogenic variants, which is animportant correlate of metastatic behavior.45 A recent thirdproposal attempted to address this by combining the PASSand GAPP scores with SDHB immunohistochemistry,46because loss of SDHB immunoreactivity suggests amutation in any one of the SDHx genes. However, thissystem has not yet been clinically validated, and it isimportant to note that SDHB immunohistochemistry canbe in-congruent in some cases.47 Given this, there wasno consensus that SDHB immunohistochemistry shouldbe routinely done on all PPGL pathology specimens. InNorth America, clinical genetic testing almost always iscovered by medical insurance and is more reliable thanimmunohistochemistry. If clinical genetic testing forSDHB pathogenic variants cannot be done for somereason, SDHB immunohistochemistry can be consideredas an alternative.In summary, the pathology of mPPGLs is poorlydocumented. The literature is confounded by mostlyretrospective studies with short follow-up time, whichcan be problematic given the long latency for developingmetastatic disease in many patients. Furthermore, manyreports fail to consider the possibility of multifocalprimary disease in patients with genetic predispositionto the development of these tumors. Prospectivestudies are needed to assess some of the proposedhistopathologic scoring systems, and the future ma
School of Medicine at the University of Pennsylvania, Philadelphia, PA; ***Endocrine Oncology Tumor Group, Division of Medical Oncology, Mayo Clinic, Rochester, MN; †††Division of Surgical Oncology, Department of Surgery, Stony Brook University Medical Center, Stony Brook, NY; ‡‡‡Department of Radiology, University of