Transcription
2020 Guideline for the Management ofPatients With Valvular Heart DiseaseGUIDELINES MADE SIMPLEA Selection of Tables and FiguresAcc.org/GMSVHD
2020 Guideline for the Management of Patients WithValvular Heart DiseaseA Report of the American College of Cardiology/American Heart Association JointCommittee on Clinical Practice GuidelinesWriting Committee:Catherine M. Otto, MD, FACC, FAHA, Co-ChairRick A. Nishimura, MD, MACC, FAHA, Co-ChairRobert O. Bonow, MD, MS, MACC, FAHAChristopher McLeod, MBCHB, PhD, FAHABlase A. Carabello, MD, FACC, FAHAPatrick T. O’Gara, MD, MACC, FAHA†John P. Erwin III, MD, FACC, FAHAVera H. Rigolin, MD, FACC, FAHAFederico Gentile, MD, FACCThoralf M. Sundt III, MD, FACC, FAHAHani Jneid, MD, FACC, FAHAAnnemarie Thompson, MDEric V. Krieger, MD, FACCMichael Mack, MD, MACCChristopher TolyThe ACC/AHA Joint Committee on Clinical Practice Guidelines has commissioned this guideline tofocus on the diagnosis and management of adult patients with valvular heart disease (VHD). Theguideline recommends a combination of lifestyle modifications and medications that constitutecomponents of GDMT. For both GDMT and other recommended drug treatment regimens, thereader is advised to confirm dosages with product insert material and to carefully evaluate forcontraindications and drug–drug interactions.The following resource contains tables and figures from the 2020 Guideline for the Managementof Patients With Valvular Heart Disease. The resource is only an excerpt from the Guideline andthe full publication should be reviewed for more tables and figures as well as important context.CITATION: J AM Coll Cardiol. Dec 2020; DOI: 10.1016/j.jacc.2020.11.018.
2020 Guideline for the Management of Patients With ValvularHeart DiseaseTable of ContentsClass of Recommendation (COR)/ Level of Evidence (LOE) Table 4Master Abbreviation List 5Top 10 Take-Home Messages 6What is new in aortic stenosis 8Table 14. A Simplified Framework With Examples of Factors Favoring SAVR, TAVI,or Palliation Instead of Aortic Valve Intervention 8Figure 2. Timing of intervention for AS 10Figure 3. Choice of SAVR versus TAVI when AVR is indicated for valvular AS 11Table 13. Stages of AS 13What is new in mitral regurgitation 14Figure 8. Primary MR 14Figure 9. Secondary MR 15Table 18. Stages of Secondary MR 16What is new in anticoagulation 17Figure 1. Anticoagulation for AF in Patients With VHD. 183
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsClass of Recommendation (COR)/ Level of Evidence (LOE) Table(Updated May 2019)4
Back to Table of ContentsGUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseMaster Abbreviation ListAbbreviation Meaning/PhraseAbbreviationMeaning/PhraseAFatrial fibrillationMDTmultidisciplinary teamARaortic regurgitationMRmitral regurgitationASaortic stenosisMSmitral stenosisAVAaortic valve area circulationMVmitral valveAVAiAVA indexed to body surface areaMVRmitral valve replacementAVRaortic valve replacementNOACnon–vitamin K oral anticoagulantBAVbicuspid aortic valveNYHANew York Heart AssociationCABGcoronary artery bypass graftRCTrandomized controlled trialCADcoronary artery diseaseRVright ventricle (right ventricular)CORClass of RecommendationSAVRsurgical aortic valve replacementCVCComprehensive Valve CenterTAVIECGelectrocardiogramEROeffective regurgitant orificeESDend-systolic dimensionTFGDMTguideline-directed managementand therapytranscatheter aortic chocardiogram)transfemoralTRtricuspid regurgitationHFheart failureTTELAleft atrium (left atrial)VHDtransthoracic echocardiography(echocardiogram)valvular heart diseaseLOELevel of EvidenceViVvalve-in-valveLVleft ventricle (left ventricular)VKAvitamin K antagonistLVEDDleft ventricular end-diastolicdimensionLVEFleft ventricular ejection fractionLVESDleft ventricular end-systolicdimensionTEE5
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsTop 10 Take-Home Messages (1 of 2)1Disease stages in patients with valvular heart disease should be classified (Stages A, B, C, and D) on thebasis of symptoms, valve anatomy, the severity of valve dysfunction, and the response of the ventricle andpulmonary circulation.2In the evaluation of a patient with valvular heart disease, history and physical examination findings shouldbe correlated with the results of noninvasive testing (i.e., ECG, chest x-ray, transthoracic echocardiogram).If there is discordance between the physical examination and initial noninvasive testing, consider further noninvasive(computed tomography, cardiac magnetic resonance imaging, stress testing) or invasive (transesophagealechocardiography, cardiac catheterization) testing to determine optimal treatment strategy.3For patients with valvular heart disease and atrial fibrillation (except for patients with rheumatic mitral stenosis or amechanical prosthesis), the decision to use oral anticoagulation to prevent thromboembolic events, with eithera vitamin K antagonist or a non–vitamin K antagonist anticoagulant, should be made in a shared decision-making processbased on the CHA2DS2-VASc score. Patients with rheumatic mitral stenosis or a mechanical prosthesis and atrial fibrillationshould have oral anticoagulation with a vitamin K antagonist.4All patients with severe valvular heart disease being considered for valve intervention should be evaluated by amultidisciplinary team, with either referral to or consultation with a Primary or Comprehensive Valve Center.5Treatment of severe aortic stenosis with either a transcatheter or surgical valve prosthesis should be basedprimarily on symptoms or reduced ventricular systolic function. Earlier intervention may be considered ifindicated by results of exercise testing, biomarkers, rapid progression, or the presence of very severe stenosis.“Top Ten Messages” is continued in the next page.6
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsTop 10 Take-Home Messages (2 of 2)6Indications for transcatheter aortic valve implantation are expanding as a result of multiple randomized trials oftranscatheter aortic valve implantation versus surgical aortic valve replacement. The choice of type of interventionfor a patient with severe aortic stenosis should be a shared decision-making process that considers the lifetime risks andbenefits associated with type of valve (mechanical versus bioprosthetic) and type of approach (transcatheter versus surgical).7Indications for intervention for valvular regurgitation are relief of symptoms and prevention of the irreversiblelong-term consequences of left ventricular volume overload. Thresholds for intervention now are lower than theywere previously because of more durable treatment options and lower procedural risks.8A mitral transcatheter edge-to-edge repair is of benefit to patients with severely symptomatic primarymitral regurgitation who are at high or prohibitive risk for surgery, as well as to a select subset of patientswith secondary mitral regurgitation who remain severely symptomatic despite guideline-directed management andtherapy for heart failure.9Patients presenting with severe symptomatic isolated tricuspid regurgitation, commonly associated withdevice leads and atrial fibrillation, may benefit from surgical intervention to reduce symptoms and recurrenthospitalizations if done before the onset of severe right ventricular dysfunction or end-organ damage to the liver and kidney.10Bioprosthetic valve dysfunction may occur because of either degeneration of the valve leaflets or valvethrombosis. Catheter-based treatment for prosthetic valve dysfunction is reasonable in selected patients forbioprosthetic leaflet degeneration or paravalvular leak in the absence of active infection.7
Back to Table of ContentsGUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseWHAT IS NEW IN AORTIC STENOSISMajor Changes in Valvular Heart Disease Guideline RecommendationsAortic Stenosis20172020Surgical AR is recommended for symptomaticpatients with severe AS (Stage D) and asymptomaticpatients with severe AS (Stage C) who meet anindication for AVR when surgical risk is lowor intermediate.For symptomatic patients with severe AS whoare 80 years of age or for younger patients witha life expectancy 10 years and no anatomiccontraindication to transfemoral TAVI, transfemoralTAVI is recommended in preference to SAVR.COR 1, LOE B-NRCOR 1, LOE ATable 14. A Simplified Framework With Examples of Factors Favoring SAVR, TAVI, orPalliation Instead of Aortic Valve InterventionFavors SAVRAge/life expectancy* Valve anatomy Prosthetic valvepreference Concurrent cardiacconditions Favors TAVIFavors PalliationYounger age/longer lifeexpectancy BAVSubaortic (LV outflowtract) calcificationRheumatic valve diseaseSmall or large aorticannulus†Mechanical or surgicalbioprosthetic valvepreferredConcern for patient–prosthesis mismatch(annular enlargementmight be considered) Aortic dilation‡Severe primary MRSevere CAD requiringbypass graftingSeptal hypertrophyrequiring myectomyAF 8Older age/fewerexpected remainingyears of lifeCalcific AS of a trileafletvalveBioprosthetic valvepreferredFavorable ratio of lifeexpectancy to valvedurabilityTAVI provides larger valvearea than same sizeSAVRSevere calcification of the ascending aorta(“porcelain” aorta) Limited life expectancyIrreversible severe LVsystolic dysfunctionSevere MR attributableto annular calcification
Back to Table of ContentsGUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart Disease Noncardiacconditions Frailty Estimated procedural orsurgical risk ofSAVR or TAVIProcedure-specific impediments Goals of Careand patientpreferences andvalues Severe lung, liver, orrenal diseaseMobility issues (highprocedural risk withsternotomy) Symptoms likelyattributable tononcardiac conditionsSevere dementiaModerate to severeinvolvement of 2 otherorgan systemsNot frail or few frailtymeasures Frailty likely to improveafter TAVI Severe frailty unlikely toimprove after TAVISAVR risk lowTAVI risk high TAVI risk low to mediumSAVR risk high toprohibitive Prohibitive SAVR risk( 15%) or post-TAVI lifeexpectancy 1 yValve anatomy, annularsize, or low coronaryostial height precludesTAVIVascular access does notallow transfemoral TAVI Previous cardiac surgery with at-risk coronarygraftsPrevious chest irradiation Valve anatomy, annularsize, or coronary ostialheight precludes TAVIVascular access doesnot allow transfemoralTAVILess uncertainty aboutvalve durabilityAvoid repeat interventionLower risk of permanentpacerLife prolongationSymptom reliefImproved long-termexercise capacity and QOLAvoid vascularcomplicationsAccepts longer hospital stay,pain in recovery period Accepts uncertaintyabout valve durabilityand possible repeatinterventionHigher risk of permanentpacerLife prolongationSymptom reliefImproved exercisecapacity and QOLPrefers shorter hospitalstay, less postproceduralpain Life prolongation not animportant goalAvoid futile orunnecessary diagnosticor therapeuticproceduresAvoid procedural strokeriskAvoid possibility ofcardiac pacer*Expected remaining years of life can be estimated from U.S. Actuarial Life Expectancy tables. The balance between expected patient longevity andvalve durability varies continuously across the age range, with more durable valves preferred for patients with a longer life expectancy. Bioprostheticvalve durability is finite (with shorter durability for younger patients), whereas mechanical valves are very durable but require lifelong anticoagulation.Long-term (20-y) data on outcomes with surgical bioprosthetic valves are available; robust data on transcatheter bioprosthetic valves extend only to5 y, leading to uncertainty about longer-term outcomes. The decision about valve type should be individualized on the basis of patient-specific factorsthat might affect expected longevity.†A large aortic annulus may not be suitable for currently available transcatheter valve sizes. With a small aortic annulus or aorta, a surgical annulus-enlarging procedure may be needed to allow placement of a larger prosthesis and avoid patient–prosthesis mismatch.‡Dilation of the aortic sinuses or ascending aorta may require concurrent surgical replacement, particularly in younger patients with a BAV.Modified from Burke CR, Kirkpatrick JN, Otto CM. Goals of care in patients with severe aortic stenosis. Eur Heart J. 2020;41:929-32.9
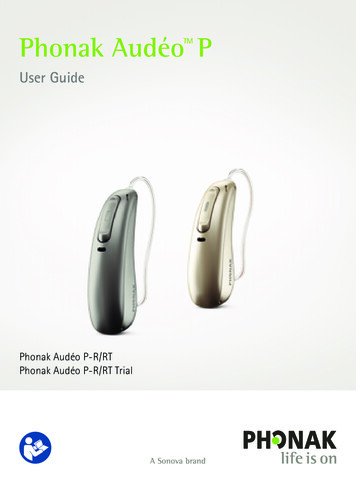
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseFigure 2. Timing of intervention for ASFor definition of stages see Table 13. Stages of AS on Page 12.10Back to Table of Contents
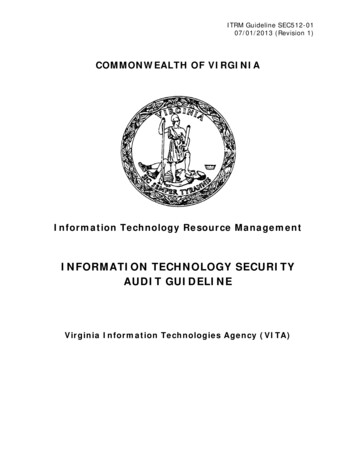
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseFigure 3. Choice of SAVR versus TAVI when AVR is indicated for valvular AS.*Approximate ages, based on U.S. Actuarial LifeExpectancy tables, are provided for guidance. Thebalance between expected patient longevity and valvedurability varies continuously across the age range,with more durable valves preferred for patients with alonger life expectancy. Bioprosthetic valve durabilityis finite (with shorter durability for younger patients),whereas mechanical valves are very durable butrequire lifelong anticoagulation. Long-term (20-year)data on outcomes with surgical bioprosthetic valves areavailable; robust data on transcatheter bioprostheticvalves extend to only 5 years, leading to uncertaintyabout longer-term outcomes. The decision about valvetype should be individualized on the basis of patientspecific factors that might affect expected longevity.†Placement of a transcatheter valve requires vascularanatomy that allows transfemoral delivery and theabsence of aortic root dilation that would requiresurgical replacement. Valvular anatomy must besuitable for placement of the specific prosthetic valve,including annulus size and shape, leaflet number andcalcification, and coronary ostial height.For definition of stages see Table 13. Stages of AS on Page 12.11Back to Table of Contents
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsTable 13. Stages of Aortic StenosisStageDefinitionValve AnatomyAAt risk of AS BProgressive AS Valve HemodynamicsBAV (or other congenital valveanomaly)Aortic valvesclerosisMild to moderate leafletcalcification/fibrosis of a bicuspid ortrileaflet valvewith somereduction insystolic motionorRheumatic valvechanges msAortic Vmax 2 m/s with Nonenormal leaflet motionNoneMild AS: aortic Vmax 2.0–2.9 m/s or mean P 20 mm HgModerate AS: aortic Vmax 3.0–3.9 m/s or mean P 20-39 mm HgEarly LV diastolicdysfunction maybe presentNormal LVEFNoneLV diastolicdysfunctionMild LVhypertrophyNormal LVEF C: Asymptomatic severe ASC1C2Asymptomaticsevere ASAsymptomaticsevere AS with LVsystolic dysfunctionSevere leaflet calcification/fibrosis or congenital stenosis withseverely reducedleaflet opening Aortic Vmax 4 m/s ormean P 40 mm HgAVA typically is 1.0cm2 (or AVAi 0.6 cm2/m2) but not required todefine severe ASVery severe AS is anaortic Vmax 5 m/s ormean P 60 mm Hg Aortic Vmax 4 m/s ormean P 40 mm HgAVA typically 1.0 cm2(or AVAi 0.6 cm2/m2)but not required todefine severe ASLVEF 50%Severe leafletcalcification/fibrosisor congenitalstenosis withseverely reducedleaflet opening 12 NoneExercise testingis reasonable toconfirm symptomstatusNone
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsD: Symptomatic severe ASD1Symptomatic severe Severe leaflethigh-gradient AScalcification/fibrosisor congenitalstenosis withseverely reducedleaflet opening Aortic Vmax 4 m/s ormean P 40 mm HgAVA typically 1.0 cm2(or AVAi 0.6 cm2/m2)but may be larger withmixed AS/AR LV diastolicdysfunctionLV hypertrophyPulmonaryhypertensionmay be present D2D3Symptomatic severelow-flow, lowgradient AS withreduced LVEFSymptomatic severelow-gradient ASwith normal LVEF orparadoxical low-flowsevere ASSevere leafletcalcification/fibrosiswith severelyreduced leafletmotion Severe leafletcalcification/fibrosiswith severelyreduced leafletmotion Exertionaldyspnea,decreasedexercise tolerance,or HFExertionalanginaExertionalsyncope orpresyncopeAVA 1.0 cm2 with resting aortic Vmax 4m/s or mean P 40 mm Hg Dobutamine stressechocardiographyshows AVA 1.0 cm2with Vmax 4 m/s at anyflow rateLV diastolicdysfunctionLV hypertrophyLVEF 50% HFAnginaSyncope orpresyncope Increased LVrelative wallthicknessSmall LVchamber withlow strokevolumeRestrictivediastolic fillingLVEF 50% HFAnginaSyncope orpresyncopeAVA 1.0 cm2 (indexedAVA 0.6 cm2/m2) withan aortic Vmax 4 m/sor mean P 40 mmHg ANDStroke volume index 35 mL/m2Measured when patientis normotensive(systolic blood pressure 140 mm Hg)13
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsWHAT IS NEW IN MITRAL REGURGITATIONMajor Changes in Valvular Heart Disease Guideline RecommendationsMitral regurgitation20172020In patients with chronic severe secondary MRrelated to LV systolic dysfunction (LVEF 50%) whohave persistent severe symptoms (NYHA classII, III, or IV) while on optimal GDMT for HF (StageD), transcatheter edge-to-edge mitral valve (TEER)repair is reasonable in patients with appropriateanatomy as defined on TEE and with LVEF between20% and 50%, LVESD 70 mm, and pulmonaryartery systolic pressure 70 mm Hg.No equivalent 2017 recommendation.COR 2a, LOE B-RFigure 8.Primary MR.For definition of stages see Table 18. Stages of Secondary MR on Page 16.*See Prosthetic Valve section (11.1.2) for choice of mitral valve replacement if mitral valve repair is not possible.14
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseFigure 9. Secondary MR.For definition of stages see Table 18. Stages of Secondary MR on page X.*Chordal-sparing MV replacement may be reasonable to choose over downsized annuloplasty repair.15Back to Table of Contents
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsTable 18. Stages of Secondary MR.StageDefinitionValve AnatomyValve HemodynamicsHemodynamicConsequencesAAt risk of MR Normal valveleaflets, chords,and annulus in apatient with CADor cardiomyopathy No MR jet or smallcentral jet area 20%LA on DopplerSmall vena contracta 0.30 cm BProgressiveMR CAsymptomaticsevere MR DSymptomaticsevere MR Regional wall motion abnormalities withmild tethering of mitral leafletAnnular dilationwith mild loss ofcentral coaptationof the mitral leafletsERO 0.40 cm2†Regurgitant volume 60 mLRegurgitant fraction 50%Regional wall motion abnormalities and/or LV dilation with severe tethering ofmitral leafletAnnular dilationwith severe loss ofcentral coaptationof the mitral leafletsERO 0.40 cm2†Regurgitant volume 60 mL‡Regurgitant fraction 50%Regional wall motion abnormalities and/or LV dilation with severe tethering ofmitral leafletAnnular dilationwith severe loss ofcentral coaptationof the mitral leafletsERO 0.40 cm2†Regurgitant volume 60 mL‡Regurgitant fraction 50% Normal or mildly dilated LV size withfixed (infarction)or inducible(ischemia) regionalwall motionabnormalitiesPrimary myocardialdisease with LVdilation and systolicdysfunctionRegional wall motionabnormalities withreduced LV systolicfunctionLV dilation andsystolic dysfunctionattributableto primarymyocardial diseaseSymptomsattributableto coronaryischemia or HFmay be presentthat respond torevascularizationand appropriatemedical therapyRegional wall motionabnormalities withreduced LV systolicfunctionLV dilation andsystolic dysfunctionattributableto primarymyocardial diseaseSymptomsattributableto coronaryischemia or HFmay be presentthat respond torevascularizationand appropriatemedical therapyRegional wall motionabnormalities withreduced LV systolicfunctionLV dilation andsystolic dysfunction attributable toprimary myocardial diseaseHF symptomsattributable to MRpersist even afterrevascularizationand optimizationof medical therapyDecreased exercisetoleranceExertional dyspnea*Several valve hemodynamic criteria are provided for assessment of MR severity, but not all criteria for each category will be present ineach patient. Categorization of MR severity as mild, moderate, or severe depends on data quality and integration of these parameters inconjunction with other clinical evidence.†The measurement of the proximal isovelocity surface area by 2D TTE in patients with secondary MR underestimates the true ERO becauseof the crescentic shape of the proximal convergence.‡May be lower in low-flow states.16SymptomsSymptomsattributableto coronaryischemia or HFmay be presentthat respond torevascularizationand appropriatemedical therapy
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of ContentsWHAT IS NEW IN ANTICOAGULATIONMajor Changes in Valvular Heart Disease Guideline RecommendationsAnticoagulation for AF in patients with VHD20172020It is reasonable to use a DOAC as an alternative to a VKA inpatients with AF and native aortic valve disease, tricuspidvalve disease, or MR and a CHA2DS2-VASc score of 2 orgreater.For patients with AF and native valve heart disease(except rheumatic mitral stenosis) or who receiveda bioprosthetic valve 3 months ago, a non–vitaminK oral anticoagulant is an effective alternative toVKA anticoagulation and should be administered onthe basis of the patient’s CHA2DS2-VASc score.COR 2a, LOE C-LDCOR 1, LOE AFor patients with new-onset AF 3 months aftersurgical or transcatheter bioprosthetic valvereplacement, anticoagulation with a VKA isreasonable.No equivalent 2017 recommendation.COR 2a, LOE B-NRIn patients with mechanical heart valves with orwithout AF who require long-term anticoagulationwith VKA to prevent valve thrombosis, NOACs arenot recommended.No equivalent 2017 recommendation.COR 3: Harm, LOE B-R17
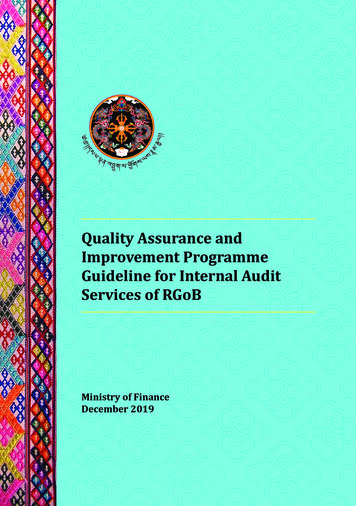
GUIDELINES MADE SIMPLEVHD 2020 Guideline for the Management of Patients With Valvular Heart DiseaseBack to Table of Contents18 2020 American College of Cardiology B20180Figure 1. Anticoagulation for AF in Patients With VHD.
GUIDELINES MADE SIMPLE VHD 2020 uideline fo the Management of atients ith alvular eart isease 6 Back to Table of Contents "Top Ten Messages" is continued in the next page. Top 10 Take-Home Messages (1 of 2) Disease stages in patients with valvular heart disease should be classified (Stages A, B, C, and D) on the basis of symptoms, valve anatomy, the severity of valve dysfunction, and the .