Transcription
Pathophysiology ofHypertension andHypertension ManagementTexas Hypertension Conference 2017Olethia E. Chisolm, MD FACPSeptember 22, 2017
Disclosure to Learner Requirement of LearnerParticipants requesting continuing education contact hours or a certificate of attendancemust 1. register for the event, 2. attend the entire session, and 3. complete evaluationbefore leaving the conference Commercial SupportThis educational activity received no commercial support Disclosure of Financial Conflict of InterestThe speaker and planning committee have no relevant financial relationships to disclose Off Label UseThere will be no discussion of off‐label use during this presentation Non‐Endorsement StatementAccredited status does not imply endorsement by Department of State Health Services ‐Continuing Education Services, Texas Medical Association, or American NursesCredentialing Center of any commercial products displayed in conjunction with an activity
BackgroundEpidemiologyCost Burden
High Blood Pressure Prevalence Adults 20Years Stratified by Age/SexNational Health and Nutrition Examination Survey: 2007–2012Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Age-Adjusted Trends for High Blood PressurePrevalence Adults 20 years Stratified byAge/Race/Ethnicity/SexNational Health and Nutrition Examination Survey: 1988–1994, 1999–2006, and 2007–2012Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
High Blood Pressure Stratified by AgeAwareness/Treatment/Control of Blood PressureNational Health and Nutrition Examination Survey: 2007– 2012Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Percentage Breakdown of Deaths Attributable toCardiovascular DiseaseUnited States 2011Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Cardiovascular Disease (CVD) Deaths VersusCancer Deaths by AgeUnited States 2011Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Direct and Indirect Costs of CardiovascularDisease (CVD) and Stroke (in billions of dollars)United States 2011Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
The 23 Leading Diagnoses for Direct HealthExpenditures (in billions of dollars)United States 2011Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Projected Total Costs of Cardiovascular Disease(CVD), 2015 to 2030 (in billions of dollars)United States 2012Dariush Mozaffarian et al. Circulation. 2015;131:e29-e322Copyright American Heart Association, Inc. All rights reserved
Age-Specific Prevalence of Hypertension in USAdultsNHANES 1999–2004Wilbert S. Aronow et al. Circulation. 2011;123:2434-2506Copyright American Heart Association, Inc. All rights reserved
PathophysiologyEssential HypertensionSecondary Hypertension
Conceptual Framework for CardiovascularAdaptations to Arterial Stiffening that Occur withAgingWilbert S. Aronow et al. Circulation. 2011;123:2434-2506Copyright American Heart Association, Inc. All rights reserved
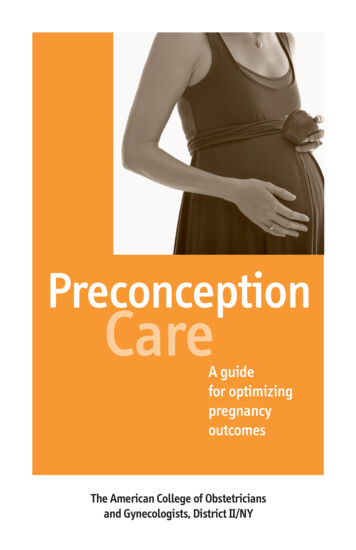
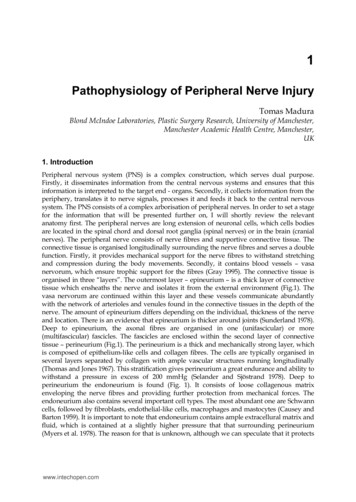
CV and renal continuum:RAAS as a mediator of pathophysiologyAtherothrombosis& progressive CVDTissue injury (MI, stroke,renal insufficiency, PAD)Early tissue dysfunctionOxidative & mechanical stressinflammationPathologicalremodelingRAASTarget organ damageVasoconstriction/Na/H2Oretention (High BP)Risk factorsESRD end-stage renal diseaseEnd-organ failure(CHF, ESRD)DeathAdapted from Dzau V et al. Circulation. 2006;114:2850-70.
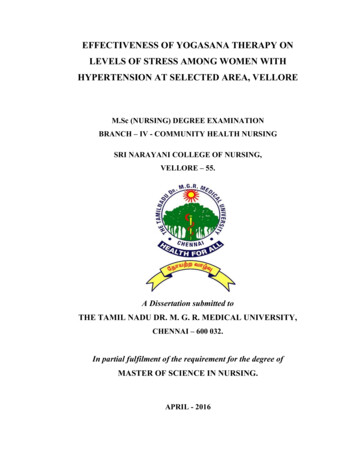
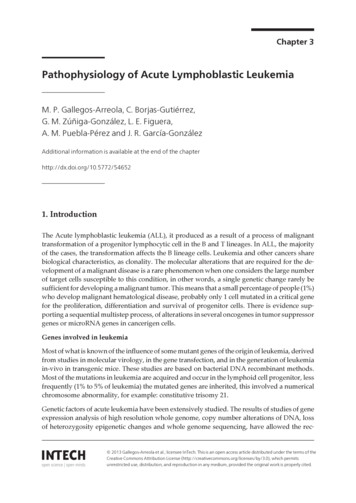
RAAS overview: Key targetsAngiotensinogen (1-14)Cathepsin DToninsTissue RAASReninBradykininAngiotensin I (1-10)ChymaseACEAngiotensin II (1-8)Negative feedback via AT1-REPACE2Angiotensin (1-7)AT1-RAT2-RSubstance PAT1-7-RAldosteroneACEKININASE IIAMP-BAMP-NAngiotensin IV (3-8)Inactive nativepathwaysAdapted from Staessen JA et al. Lancet. 2006;368:1449-56.
TreatmentLifestyle Modification
Special PopulationsTreatment of Hypertension in Patients With Coronary Artery Disease
Summary of BP GoalsBP Goal, mm Hg 140/90 130/80Abdominal Aortic Aneurysm(AAA)Blood Pressure (BP)Heart Failure (HF)Ischemic Attack (TIA)ConditionClass/Level of ardial infarction,stroke or TIA, carotid arterydisease, PAD, AAAIIb/BAcute Coronary Syndrome (ASC)Coronary Artery Disease (CAD)Peripheral Arterial Disease (PAD)TransientCirculation 2015;131:e435-e470
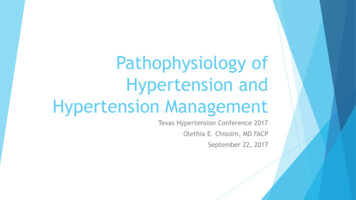
Pharmacological Treatment of Hypertension in theManagement of Ischemic Heart DiseaseACEI 212222‖21‖Non-DHPDHP CCBCCBHydralazine/IsosorbideDinitrate2ACEI indicates angiotensin-converting enzyme inhibitor; ACS, acute coronary syndrome; ARB, angiotensin receptor blocker; CCB, calcium channelblocker; DHP, dihydropyridine; HF, heart failure; 1, drug of choice; and 2, “add-on,” alternative drug, or special indications. * Especially if prior myocardial infarction, left ventricular systolic dysfunction, diabetes mellitus, or proteinuric chronic kidney disease is present. † Chlorthalidone is preferred. Loop diuretic should be used in the presence of HF (New York Heart Association class III or IV) or chronic kidney diseasewith glomerular filtration rate 30 mL·min 1·1.73 m 2. Caution should be exercised in HF with preserved ejection fraction. ‡ If β-blocker is contraindicated, a non-DHP CCB can be substituted, but not if left ventricular dysfunction or HF is present. Caution should beexercised if combining a non-DHP CCB with a β-blockerCirculation:2015;131:e435-e470
Recommendations: The 140/90-mm Hg BP target is reasonable for the secondary prevention ofcardiovascular events in patients with hypertension and CAD (Class IIa; Level ofEvidence B). A lower target BP ( 130/80 mm Hg) may be appropriate in some individuals withCAD, previous MI, stroke or transient ischemic attack, or CAD risk equivalents(carotid artery disease, PAD, abdominal aortic aneurysm) (Class IIb; Level ofEvidence B). In patients with an elevated DBP and CAD with evidence of myocardial ischemia,the BP should be lowered slowly, and caution is advised in inducing decreases inDBP to 60 mm Hg in any patient with diabetes mellitus or who is 60 years of age.In older hypertensive individuals with wide pulse pressures, lowering SBP may causevery low DBP values ( 60 mm Hg). This should alert the clinician to assess carefullyany untoward signs or symptoms, especially those resulting from myocardialischemia (Class IIa; Level of Evidence C).Circulation. 2015;131:e435-e470
Special PopulationsTreatment of Hypertension in Patients With Heart Failure
Recommendation for PreventionClyde W. Yancy et al. Circulation. 2017;136:e137-e161Copyright American Heart Association, Inc. All rights reserved
Recommendation for Hypertension in StageHFrEFClyde W. Yancy et al. Circulation. 2017;136:e137-e161Copyright American Heart Association, Inc. All rights reserved
Recommendation for Hypertension in StageHFpEFClyde W. Yancy et al. Circulation. 2017;136:e137-e161Copyright American Heart Association, Inc. All rights reserved
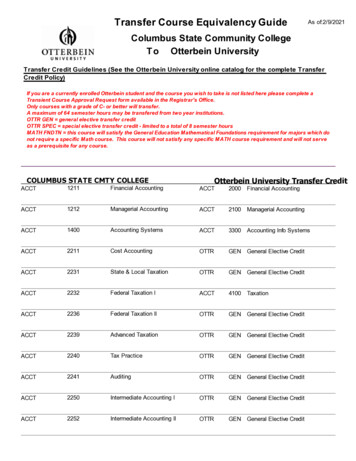
Beckett NS et al. N Engl J Med 2008;358:1887-1898
Beckett NS et al. N Engl J Med 2008;358:1887-1898
Conclusion Evidence based data concludes the use of antihypertensivetreatment with indapamide (sustained release), with or withoutperindopril, is beneficial for hypertensive persons 80 years of age
* Especially if prior myocardial infarction, left ventricular systolic dysfunction, diabetes mellitus, or proteinuric chronic kidney disease is present. † Chlorthalidone is preferred. Loop diuretic should be used in the presence of HF (New York Heart Association class III or IV) or chronic kidney disease