Transcription
Hypertension Management ProgramFor Primary Care ClinicsGetting Started ToolkitHelping primary care organizations plan & implement chronic disease prevention and managementstrategies for hypertension; an evidence-based approach designed to aid in the effective treatment ofhigh blood pressure
Table of Contents38 - 14415 - 20Why Address Hypertension?The Framework5The Hypertension Management Program6The Hypertension Management Initiative7Self-AssessmentHypertension Management Programming:Implementation Resources21Appendix A21Appendix BToolkit Introduction2
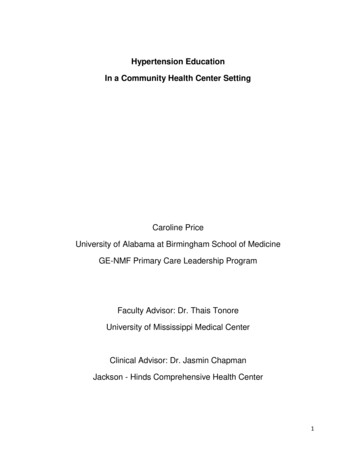
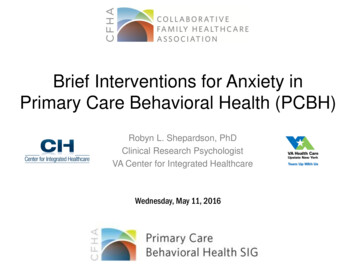
Why Address Hypertension?40%19%20%of Canadian Adults 25yrs have Hypertensionof global deaths caused byHypertensionof Canadians havepre-hypertension orelevated BP9.1 millionlives lost annually (2010)Cost of Treating Hypertension 13 Billion (2010) expected to reach 20 Billion annually by 202025%Global reduction in uncontrolledHypertension by 2025, agreementat World Health Assembly9 out of 10Canadians expected to developHypertension in normal lifespan3
The FrameworkDelivery System Design Interdisciplinary care teams with definedroles and responsibilities Innovative patient interactions Care planning, care paths and caremanagement Enhanced health promotion andprevention Outreach and population needs-basedcare and cultural sensitivityProvider Decision Support Evidence-based guidelines embedded intodaily practice Provider Education Access to specialist expertise Clinical care and client management tools Provider alerts and prompts Measurement, Evaluation, RoutineReporting and FeedbackSelf-management SupportsSelf-management Supports Clients are part of care team and engaged in shared decision making Client registries (e.g., client with diabetes Individuals empowered to be self-managers Electronic health records Self-management support services organized for clients Provider portals Shared clinical guidelines Client portals Follow-up Population health data4
The HypertensionManagement Program:With the introduction of Ontario’s Chronic Disease andManagement Framework, there was recognition that theway chronic disease is handled needed to change. In orderto provide patients with greater autonomy in taking a rolein managing their condition, education and collaborationon treatment is needed, allowing for effective ‘selfmanagement’. Patients empowered with knowledge andtools for self-management aid in preventing exasperationor progression of chronic conditions, enabling bettercontrol and health outcomes.The other aspect of the framework was addressing carein a more collaborative approach, with clinicians workingwith their allied health teams and administration to providecoordinated, proactive and progressive support bothmedically and to address the common, controllable lifestylerisks that contribute to chronic diseases.The Hypertension Management Program (HMP) began asa research study, called the Hypertension ManagementInitiative (HMI), led by the Heart & Stroke Foundation ofOntario, and Dr. Sheldon Tobe as the principal investigator.Launched in 2007, the HMI used an approach in line withOntario’s Chronic Disease and Management Framework.Following the results of this study, the HMI became theHypertension Management Program (HMP), fully funded bythe Ministry of Health and Long Term Care.Looking at the study, and results:“Hypertension, also referred to as the ‘silent killer’, is asignificant chronic health condition and is prevalent in 1out of 5 adult Canadians. Despite being the number onediagnosis listed for patient visits, a substantial proportionof people remain unaware of their hypertension or havenot achieved treatment targets. Data compiled by theHeart and Stroke Foundation of Ontario indicates thatconsumers do not take hypertension seriously, thatphysicians are not consistently applying clinical practiceguidelines related to diagnosis and treatment targets, thatpatients are not adhering to prevention and treatmentrecommendations and that physicians lack time and skillto counsel patients about needed lifestyle modifications.Clinical trials demonstrate the efficacy and safety of bloodpressure control and clinical practice recommendationsprovide guidance to achieve blood pressure targets.However, to achieve the benefits from blood pressurecontrol across the entire population, without expending aneven larger fraction of primary care physician’s time to themanagement of this chronic disease, a new paradigm isrequired.“The HMI focuses on what is acknowledged to be a criticalissue in high blood pressure – improving the managementof this chronic health condition by primary care providers(doctors, nurse practitioners, nurses and communitypharmacists) and patients.” [study protocol]The HMI implemented and evaluated a local systems changeeducational approach designed to enhance physician,nursing and pharmacist approaches to high blood pressuredetection, intervention and follow up measures, along withstrengthen patient communications and supports to enableself management.5
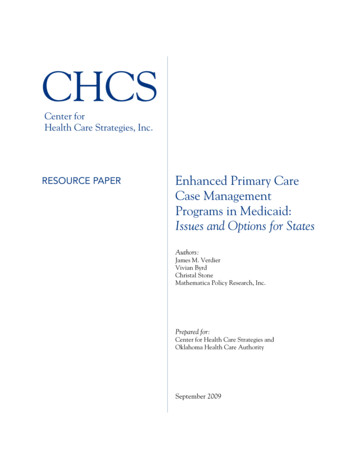
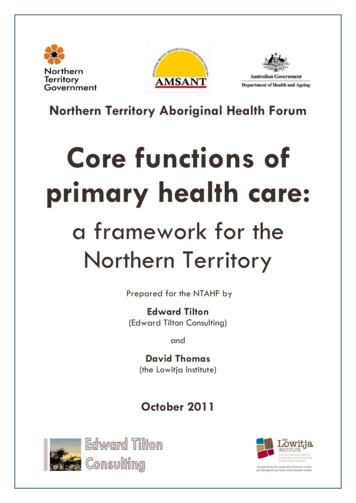
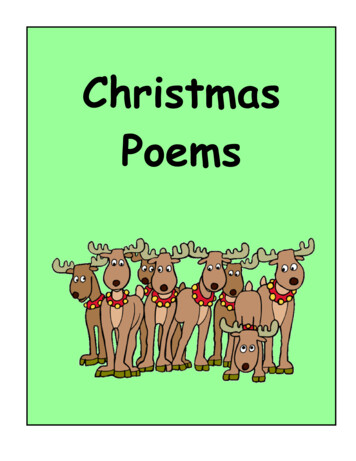
The Hypertension Management InitiativeThe StudyProvider Education 200ProvidersPatient Education &Self-ManagementTools to collectinformation, measureand monitor outcomes 3600PatientsCost & OutcomesEffective, evidencebased care 33,000PatientVisitsStudy OutcomesMean BP 6.4/3.8mmHg over allHypertension pts.Mean BP34.6/20.8 mmHgfor pts. with thehighest baseline BP41% pts.Controlled totargetProviderknowledge andconfidenceCommunication:interprofessional &patient/provider6
About this Toolkit:4.The Hypertension Management Programming Toolkit(toolkit) helps primary care organizations assess wherethey are with respect to hypertension management,and provides practical resources for implementingreal change to meet chronic disease prevention andmanagement approaches to support their patients. Builton the knowledge of the HMI study and years of the HMPrunning as a funded program, this toolkit enables broaderaudiences to advance their approach to hypertensionmanagement.Patients are part of the care team, theyare provided with information to let themknow what their condition is, how theycan play a role in its management, what toexpect in their care, and where to reachout for support (patients are at the centreof the care team)5.Organization has, or is willing toimplement a system to measure theclinical processes and patient outcomesfor hypertension management/hypertension patients, celebrate thesuccesses while taking action to makeimprovements based on these results (keyperformance indicators, and qualityimprovement plans)6.Structures, spaces and equipment providethe ability to measure, monitor andsupport patients (accuracy, comfort)Guiding principals:1.2.3.Commitment to collaborative, proactive,guidelines based chronic disease care forpatients is included in the organizationsstrategic plan, operating plan, corporategoals/objectives and/or quality improvementplans (team is supported in this approach)Organization is open to providing &encouraging ongoing education and/ortraining for hypertension diagnosis andcare, along with motiviational interviewingtechniques to support patient selfmanagement (team knowledge is acquiredand maintained)The approach to hypertension managementis interprofessional, with interdisciplinarycare teams whose roles and responsibilitiesare defined, evidence based best practicecare is embedded into daily practice (teamapproach, with tools at point of care)This Hypertension Management Programming Toolkitcontains:a. Self Assessment tool – Questions guided by the 6principals to identify strengths and opportunitiesb. Implementation Resources – Tools & Tips to informaction plans and enable clinical teams7
Hypertension Management Programming Self-Assessment ToolThis Self-Assessment Tool is a way for primary careorganizations to identify strengths in chronic diseaseprevention and management along with opportunities forprovision of evidence based chronic disease care, includinghypertension management.How to Prepare:99 Select who will conduct the assessment; it is preferablethat the assessor(s) include organizatinal leadership inclinical programming or quality improvement/reporting,along with clinical management of patients withhypertension or elevated blood pressure (e.g. a programcoordinator and a clinician)Ensure assessor(s) have access to:a. Staff in clinical care areas who provide care forhypertension patientsb. Guiding documents (such as organizational policies,plans, directives, guidelines, care pathways, etc.)c. Staff training/education (such as job profiles, educationplans)Print the Self-Assessment Tool, document the assessmenton the printed tool. Use the results of the assessment andany notes to help inform and create action plans for initialimplementation and beyond.99 Create a list of all areas/units/staff that provide care forhypertension patients8
Self-AssessmentPrincipal 1: Commitment to collaborative, proactive,guidelines based on chronic disease care for patients isincluded in the organizations strategic plan, operating plan,corporate goals/objectives and/or quality improvement plans(team is supported in this approach) Chronic disease prevention and management skills/qualifications are incorporated into human resourceprocesses where applicable (e.g. such as hiring practicesand performance)Select all support statements that apply:Select all commitment statements that apply: Hypertension management is not currently anorganizational priority Our organization is currently implementing atleast one chronic disease program or guidelinesbased hypertension management goal (e.g. QualityImprovement Plan or QIP) Our organization has a standing committee/teamthat implements chronic disease programs and/orimprovement work on an ongoing basis There is a member of the senior leadership team that isresponsible for chronic disease program committees/teams Our organization has NOT YET reviewed guidingdocuments (e.g. policies, standards, procedures,care pathways, etc.) to ensure they fully support acollaborative approach to chronic disease preventionand management Our organization has reviewed SOME guiding documentsand/or is actively reviewing / updating guidingdocuments to support evidence based collaborativechronic disease prevention and management Our organization has guiding documents in place thatsupport collaborative approaches to evidence basedchronic disease prevention and management (e.g.medical directives, care pathways, etc.) A coordinated plan or strategy for chronic diseasemanagement is in place, which aligns / prioritizes acollaborative approach to chronic disease preventionand management Our organization’s senior leadership team receivesregular reports on chronic disease programs andimprovement work and actively monitors the work toensure it aligns with the strategic goals/priorities of theorganization and patient population9
Self-AssessmentPrincipal 2: Our organization is open to providing &encouraging ongoing education and/or training forhypertension diagnosis and care, along with motivationalinterviewing techniques to support patient self management(team knowledge is acquired and maintained)We provide (directly or sponsored) training to all staff onchronic disease prevention and management (e.g. generalawareness on chronic diseases, common risk factors,programs in place, speaking to patients)Select the statement that best applies: We do not provide this training This training is optional This training is provided one time (e.g. all staff atorientation) This training is provided on an ongoing basis (e.g.refreshed periodically)We provide (directly or sponsored) training for healthcareproviders on clinical topics and supporting mechanismsfor collaborative chronic disease management (e.g. bestpractice guidelines for care such as Hypertension Canadaguidelines, C-CHANGE; supportive mechanisms such asmotivational interviewing, choices and change, etc.)Select the statement that best applies: We do not provide this training This training is optional This training is provided one time (e.g. all staff atorientation) This training is provided on an ongoing basis (e.g.refreshed periodically)Note: For this section, training may be locally done/directlydone in the organization, or sponsored through educationplans, conference funding, etc.10
Self-AssessmentPrincipal 3: The approach to hypertension management isinterprofessional, with interdisciplinary care teams whoseroles and responsibilities are defined, evidence basedbest practice care is embedded into daily practice (teamapproach, with tools at point of care)Interprofessional / interdisciplinary / community rolesSelect the statement(s) that best apply:We have a process in place which assures seamlesstransitions between care delivery team members (e.g.escallation, referrals, etc.) for: None of our patient needs Some of our patient needs Most of our patient needs All of our patient needs Our organization has assessed our internal care deliveryteam for chronic disease management (assessed:identified the skills of individuals to support care) Our organization has addressed gaps within the internalcare delivery team for chronic disease management(addressed: closed gaps through training, tools, medicaldirectives, community partnerships, external referrals, etc.) Our organization has aligned the internal care deliveryteam for chronic disease management (aligned:individuals are actively engaged in different aspects ofpatient care in line with their skills, scope of practice,role descriptions, etc.)11
Self-AssessmentPrincipal 4: Patients are part of the care team, they areprovided with information to let them know what theircondition is, how they can play a role in its management,what to expect in their care, and where to reach out forsupport (patients are at the centre of the care team)Patient Self-ManagementSelect the statement(s) that best apply:Care plans, goals and expected results o
nursing and pharmacist approaches to high blood pressure detection, intervention and follow up measures, along with strengthen patient communications and supports to enable self management. 6 The Hypertension Management Initiative Study Outcomes 41% pts. Controlled to target Mean BP 34.6/20.8 mmHg for pts. with the highest baseline BP Mean BP 6.4/3.8 mmHg over all Hypertension pts.