Transcription
Living withCrohn’s Diseasea
What’s InsideUnderstanding your diagnosis. 1What is Crohn’s disease?. 2Will it ever go away?. 3A brief introduction to the gastrointestinal(GI) tract. 3Who gets Crohn’s disease?. 4The genetic connection. 5What causes Crohn’s disease?. 6No one knows the exact cause(s)of the disease. 6What are the signs and symptoms?. 6Beyond the intestine. 8Types of Crohn’s disease. 8Patterns of disease. 9Making the diagnosis. 10Questions to ask your doctor.11Treatment.13Managing your symptoms.16Other considerations .17Surgery.17Diet and Nutrition. 18Complementary and alternativetherapies. 21Stress and emotional factors. 21General health maintenance. 22Support. 23Hope for the future.25Knowledge and support are power!.26Glossary of terms. 30Understanding yourdiagnosisYour doctor has just told you that you haveCrohn’s disease. Now what? You probablyhave lots of questions. Some of the mostcommonly asked questions are: What is Crohn’s disease? Is there a cure for Crohn’s disease, and whatis the outlook (prognosis)? How did I get it? Will I be able to work, travel, or exercise? Should I be on a special diet? What are my treatment options? Will I need surgery? How will Crohn’s disease change my life,both now and in the future?The purpose of this brochure is to provide helpful answers to these questions, and to walk youthrough some key points about Crohn’s diseaseand what you may experience now and in thefuture. You won’t become an expert overnight,but you’ll learn more as time goes on. The moreinformed you are, the better you can manageyour disease and become an active member ofyour own healthcare team.The Crohn’s & Colitis Foundation provides information foreducational purposes only, which is current as of the printdate. We encourage you to review this educational material with your healthcare professional as this informationshould not replace the recommendations and advice ofyour doctor. The Foundation does not provide medicalor other healthcare opinions or services. The inclusionof another organization’s resources or referral to anotherorganization does not represent an endorsement ofa particular individual, group, company, or product.1
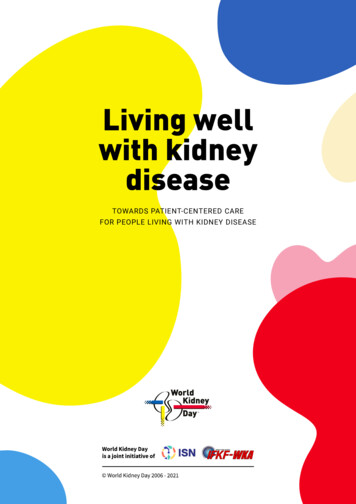
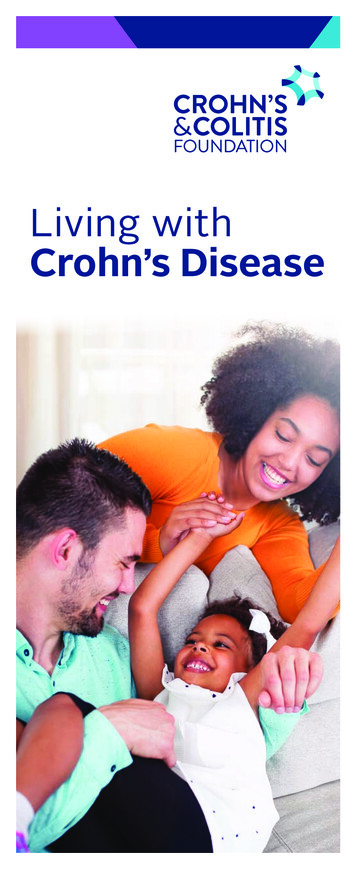
What is Crohn’s disease?colitis and Crohn’s disease, a condition calledindeterminate colitis.The disease is named after Dr. Burrill B. Crohn,who published a landmark paper with colleaguesDrs. Gordon Oppenheimer and Leon Ginzburgin 1932 that described what is known today asCrohn’s disease.Will it ever go away?Crohn’s disease (CD) belongs to a group ofconditions known as inflammatory boweldiseases (IBD). Crohn’s disease is a chronicinflammatory condition of the gastrointestinaltract. Symptoms include diarrhea (sometimesbloody), as well as crampy abdominal pain,nausea, fever, loss of appetite, weight loss,fatigue (tired, exhausted feeling), and, at times,rectal bleeding. When you have Crohn’sdisease, you will not have the same symptomsall of the time. In fact, sometimes you mayhave no symptoms at all. When you have nosymptoms, this is called clinical remission.When reading about inflammatory boweldiseases, you need to know that Crohn’s disease is not the same thing as ulcerative colitis,another type of IBD. The symptoms of thesetwo illnesses are quite similar, but the areasaffected in your body are different. Crohn’s disease may affect any part of the gastrointestinal(GI) tract, from the mouth to the anus, butulcerative colitis is limited to the colon—alsocalled the large intestine.CD most commonly affects the end of thesmall bowel (the ileum) and the beginningof the colon. Crohn’s disease can also affectthe entire thickness of the bowel wall, whileulcerative colitis only involves the innermostlining of the colon. Finally, in Crohn’s disease,the inflammation of the intestine can “skip”—leaving normal areas in between patches ofdiseased intestine. This does not occur inulcerative colitis. In only 10 percent of casesare there overlapping features of both ulcerative2No one knows exactly what causes Crohn’sdisease. Also, no one can predict how thedisease—once it is diagnosed—will affect aparticular person. Some people go for yearswithout having any symptoms, while othershave more frequent flare-ups, or attacks.However, one thing is certain: Crohn’s diseaseis a chronic condition.Chronic conditions are ongoing and long term.Studies show that people with Crohn’s diseaseusually have the same life expectancy as peoplewithout Crohn’s disease. It is important toremember that most people who have Crohn’sdisease lead full, happy, and productive lives.A brief introductionto the gastrointestinal(GI) tractMost of us aren’t very familiar with the GI tract,but it’s time you get acquainted.Here’s a quick overview: The GI tract (seefigure 1) actually starts at the mouth. It followsa twisting and turning course and ends, manyyards later, at the rectum. In between are anumber of organs that all play a part in processing and transporting food through the body.The first is the esophagus, a narrow tube thatconnects the mouth to the stomach. Foodpasses through the stomach and enters thesmall intestine. This is the section where mostof our nutrients are absorbed. The smallintestine leads to the colon, or large intestine,which connects to the rectum.3
THE GASTROINTESTINAL(GI) TRACT11 Oral Cavity (mouth)2 Esophagus (throat)23 Liver4 Stomach345 Large Intestine/Colon6 Small Intestine57 Rectum68 Anus78Figure 1The principal function of the colon is to absorbexcess water and salts from waste material(what’s left after food has been digested). Italso stores solid waste, converting it to stool,and excretes it through the anus.When inflammation occurs, the primary functions are affected, including the absorption ofwater. As a result, diarrhea can be a very common symptom during flares of Crohn’s disease.Who gets Crohn’sdisease? While Crohn’s disease can affect those fromany ethnic background, it is more commonamong Caucasians. However, prevalence andincidence rates among Hispanics and Asianshave recently increased.5,6 Both Crohn’s disease and ulcerative colitis arediseases found mainly in developed countries,more commonly in urban areas rather thanrural ones, and more often in northern climates than southern ones. However, some ofthese disease patterns are gradually shifting.For example, the number of cases of IBD isincreasing in developing parts of the world,including China, India, and South America.6,7The genetic connectionResearchers have discovered that Crohn’s disease tends to run in families. In fact, the risk fordeveloping IBD is between 1.5 percent and 28percent for first-degree relatives of an affected person.8 While genetic background plays aclear role, environmental factors such as diet,smoking, lifestyle, pollutants, and others mayimpact onset, progression, and relapse of thedisease. As such, while family history has astrong association with increased risk of IBD, itis currently not possible to confidently predictwhich, if any, family members will developCrohn’s disease.9,10 On average, people are more frequentlydiagnosed with Crohn’s disease betweenthe ages of 20 and 30, although the diseasecan occur at any age and an increasedincidence of pediatric Crohn’s disease hasbeenreported globally.1-4 Males and females appear to beapproximately equal.145
What causes Crohn’sdisease?No one knows the exact cause(s)of the diseaseNothing that you did made you get Crohn’sdisease. You didn’t catch it from anyone. Itwasn’t something that you ate or drank thatbrought the symptoms on. Leading a stressfullifestyle didn’t cause it. So, above all, don’tblame yourself!What are some of the likely causes? Mostexperts think there is a multifactorialexplanation. This means that it takes anumber of factors working in combinationto bring about Crohn’s disease.More than 200 genes have now been associated with IBD, though their exact role is stillunder investigation. It’s likely that a personinherits one or more genes that make himor her more susceptible to Crohn’s disease.These genes then lead to an abnormal immuneresponse to some environmental triggers.Scientists have not yet unequivocally identified specific triggers but the bacteria in theintestine, part of our microbiome, are a leadingcandidate. Other environmental factors (diet,viruses, stress, smoking, etc.) likely play a roleas well. In a genetically susceptible individual,whatever the trigger is, it prompts the person’simmune system to “turn on” and launch anattack in the GI system. That is when the inflammation begins. Unfortunately, the immunesystem doesn’t “turn off,” so the inflammationcontinues, damaging the digestive tract andcausing the symptoms of Crohn’s disease.What are the signs and symptoms?As the intestinal lining becomes inflamed andulcerated (small and large sores), the smallbowel loses its ability to absorb nutrients. The6large intestine cannot absorb water efficiently.Both of these factors lead to a progressiveloosening of the stool—in other words, diarrhea.The damaged intestinal lining may begin producing excess mucus in the stool. Moreover,ulceration in the lining can also cause bleeding,leading to bloody stool. Eventually, that bloodloss may lead to a low red blood cell count,called anemia.Most people with Crohn’s disease experienceurgent bowel movements as well as crampyabdominal pain. These symptoms vary fromperson to person and may change over time.Together, these may result in loss of appetiteand subsequent weight loss. These symptoms,along with anemia, can also lead to fatigue.Children with Crohn’s disease may fail to developor grow properly.Symptoms may range from mild to severe.Because Crohn’s disease is a chronic disease,patients will go through periods in which thedisease flares up (is active) and causes symptoms. In between flares, people may experience no symptoms at all. These disease-freeperiods (known as “remission”) can spanmonths or even years, although symptomstypically do return at some point.Inflammation may also cause fistulas to develop.A fistula is an abnormal connection that leadsfrom one loop of intestine to another, or thatconnects the intestine to the bladder, vagina,or skin. Fistulas occur most commonly aroundthe anal area. If this complication arises, youmay notice drainage of mucus, pus, or stoolfrom this opening.Other complications that may result fromchronic inflammation include strictures(narrowing of the intestine from scar tissue) orabscesses. An abscess is a collection of fluidoutside of the intestine that contains bacteria,intestinal fluid, and pus (white blood cells).7
Beyond the intestineIn addition to having symptoms in the GI tract,some people also may experience a variety ofsymptoms in other parts of the body associatedwith Crohn’s disease. Signs and symptoms ofthe disease may be evident in the: eyes (redness, pain, and/or changes in vision) mouth (sores) joints (swelling and pain) skin (tender bumps, painful ulcerations,and other sores/rashes) bones (osteoporosis) kidney (stones) liver (primary sclerosing cholangitis andcirrhosis)—a rare developmentAll of these are known as extraintestinalmanifestations of Crohn’s disease because theyoccur outside of the digestive system. In somepeople, these actually may be the first signs ofCrohn’s disease, appearing even years beforethe bowel symptoms. In others, they may coincide with a flare-up of intestinal symptoms.Types of Crohn’s diseaseThe symptoms and potential complications ofCrohn’s disease differ, depending on what partof the GI tract is affected. The following arefive types of Crohn’s disease: Crohn’s (granulomatous) colitis: Affects thecolon only. Gastroduodenal Crohn’s disease: Affectsthe stomach and duodenum (the first partof the small intestine). Ileitis: Affects the ileum. Ileocolitis: The most common form of Crohn’sdisease affecting the colon and terminal ileum(the last section of small intestine).8 Jejunoileitis: Produces patchy areas ofinflammation in the jejunum (upper halfof the small intestine).Patterns of disease Luminal Crohn’s disease (InflammatoryCrohn’s disease)Luminal Crohn’s disease refers to Crohn’sdisease causing inflammatory changes inthe lining, or wall, of the intestine. Approximately 55 percent of patients withluminal Crohn’s disease are symptom freeor in remission in any given year. Another 15 percent have low activity ofdisease, while about 30 percent experiencehigh activity. A patient with luminal Crohn’s disease, whoremains in remission for one year, has an 80percent chance of staying in remission foran additional year, while those experiencingactive disease in the past year have a 70percent chance of recurrent symptomaticflare during the next year. Fibrostenosing Crohn’s diseaseFibroste nosing Crohn’s disease is characterizedby strictures, or narrowing of the intestine,which can lead to bowel obstructions (blockages). This disease course in Crohn’s diseasevaries from person to person and from yearto year. It generally follows a pattern of flares(when symptoms occur and the conditionworsens) and remissions. This pattern is thechronic, relapsing course of Crohn’s disease. Penetrating Crohn’s diseaseAnother pattern is known as penetratingCrohn’s disease. This results in fistulae, whichare abnormal connections between theinflamed intestine and other parts of theintestine, bladder, skin, or vagina. Thesefistulae can also occur around the anus andare termed perianal. The outlook for this typeof Crohn’s disease depends on the locationand complexity of the fistulae.9
Most patients with Crohn’s disease have aninflammatory pattern early in their diseasecourse. However, many progress to fibrostenosing or penetrating disease over time.For more information about the managementof symptoms and complications related toCrohn’s disease, visit the Foundation’s websiteat www.crohnscolitisfoundation.org/brochures.Making the diagnosisThe path toward diagnosis begins by takinga complete patient and family medical history,including full details regarding symptoms.A physical examination is also performed.Since a number of other conditions can producethe same symptoms as Crohn’s disease, yourdoctor relies on various medical tests to ruleout other potential causes for your symptoms,such as infection. Tests may include: Stool tests: Used to exclude infection orto detect inflammation (fecal calprotectin). Blood tests: May detect the presence ofinflammation, abnormal antibodies, anemia,or nutritional/vitamin deficiencies. Colonoscopy and upper endoscopy: Usedto look at the lining of your gastrointestinaltract with a scope or a tube with a cameraand a light at the end. Biopsies can beobtained through these scopes. There isalso a special miniaturized camera that canbe swallowed by the patient and specificallyused to evaluate the small bowel. Bowel Imaging: Cross-sectional imagingrefers to the use of computerized tomography (CT) scanning or magnetic resonanceimaging (MRI) to evaluate the intestinal tractand surrounding structures for the presence10of inflammation or complications such asstrictures, fistulae, or abnormal fluid collections. The advantage of MRI is that it doesnot involve radiation exposure. However, itis usually more expensive than CT imaging.In some areas, ultrasonography, using soundwaves, can detect some of these changes aswell. Ultrasonography for Crohn’s disease isnot widely used in the U.S.For further information about diagnosingCrohn’s disease, please read our Diagnosingand Monitoring IBD brochure available ons to ask yourdoctorIt is important to establish good communications with your doctor. Patients will need toestablish a collaborative relationship with alltheir healthcare providers, especially theirgastroenterologist, to achieve the best longterm results.It is common to forget to ask some criticalquestions during your office visit. Here is a list ofquestions that may be helpful for your next visit: Could any condition other than my Crohn’sdisease be causing my symptoms? What tests do I need to have to get to theroot of my symptoms? Should I have these tests during the timeof a flare-up or on a routine basis? What parts of my GI tract are affected? How will I know if my medication needsto be adjusted? What happens if I miss taking a dose or if Istop taking my medication?11
TreatmentThere are very effective treatments availablethat may control your Crohn’s disease and evenplace it into remission. These treatments workby decreasing the abnormal inflammation inthe GI system. This permits the system to healand will then relieve symptoms of diarrhea,rectal bleeding, and abdominal pain. Approximately how long should it take to seesome results, or to find out that this may notbe the right medication for me? What are the side effects of the medication?What should I do if I notice them? What should I do if the symptoms return?Which symptoms are considered anemergency? If I cannot schedule a visit right away, arethere any over-the-counter medicationoptions that can assist with my prescribedmedication? If so, which ones? Should I change my diet or take nutritionalsupplements? If so, can you recommend a dietitian or any specific nutritional supplements? Do I need to make any other lifestyle changes? When should I come back for a follow-upappointment? What are my options if I can’t afford mymedications?The two basic goals of treatment are to achieveremission and, once that is accomplished, tomaintain remission. If remission cannot beestablished, then the next goal is to decreasethe severity of disease in order to improvethe patient’s quality of life. Some of the samemedications may be used to accomplish this,but they are given in different dosages and fordifferent lengths of time.There is no one size fits all treatment foreveryone with CD. The approach must betailored to the individual, because eachperson’s disease is different.Medical treatment can bring about remission,which can last for months to years. However,Crohn’s disease activity may flare up at timesfrom the reappearance of inflammation. A disease flare may also be triggered from a complication such as a fistula, stricture, or abscess.Flares of Crohn’s disease may indicate that achange in medication dose, frequency, or typeis needed.Physicians have been using some medicationsfor the treatment of Crohn’s disease for manyyears. Others are recent breakthroughs. Themost commonly prescribed fall into the following categories: Aminosalicylates: These include medicationsthat contain 5-aminosalicylic acid (5-ASA).These medications work by inhibiting certainpathways that produce substances that cause1213
inflammation. They can work in the liningof the GI tract to decrease inflammation.They are thought to be effective in treatingmild-to-moderate flares of Crohn’s disease,and useful as a maintenance treatment inpreventing relapses of the disease. Aminosalicylates work best in the colon and are notparticularly effective if the disease is limitedto the small intestine. These are often givenorally in the form of delayed release tabletsto target the colon, or rectally as enemas orsuppositories. Corticosteroids: These medications affectthe body’s ability to launch and maintain aninflammatory process. In addition, they workto keep the immune system in check. Corticosteroids are used in people with moderateto-severe Crohn’s disease. Budesonide, acorticosteroid released primarily at the endof the small bowel (distal/terminal ileum), isused for the treatment of mild-to-moderateCrohn’s disease. Corticosteroids are effectivefor short-term control of disease activity;however, they are not recommended forlong-term or maintenance use because oftheir side effects. If you cannot come offsteroids without a relapse of symptoms, yourdoctor may need to add some other medications to help manage your disease. Becauseof their effect on the adrenal glands, steroidscannot be stopped abruptly.in people who haven’t responded to othermedications and may take several weeks tomonths to begin working. Biologic therapies: These are protein-basedtherapies made from living organisms, eitherhuman or animal. These medications areantibodies that stop certain proteins in thebody from causing inflammation. They arecurrently offered in an injectable form, orthrough intravenous infusion (through theveins). There are also biologic medicationsknown as biosimilars. Biosimilars are designed to be similar, near identical copies ofanother already approved biologic therapy,known as an originator drug or referenceproduct. They have the same safety andeffectiveness, and are taken in the same wayas the originator drugs. Antibiotics: Antibiotics may be used wheninfections—such as abscesses—occur inCrohn’s disease. They can also be helpful withfistulas around the anal canal and vagina.Future Therapies: Research advances havecontributed to breakthroughs in the development of newer medical options for the treatment of IBD. Further developments may leadto expanding how currently approved medications are used in other diseases, includingCrohn’s disease. Immunomodulators: This class of medications controls or suppresses the body’s immune system response, therefore decreasinginflammatory activity. Immunomodulators aregenerally used in people for whom aminosalicylates haven’t been effective or have beenonly partially effective. Some immunomodulators are added to make other medications,such as biologics, work better by preventingthe antibody formation to biologic medications. They may be useful in reducing oreliminating the need for corticosteroids. Theymay also be effective in maintaining remissionThere are many therapies currently underinvestigation—for a current, up-to-date listof all FDA-approved medications for Crohn’sdisease, please visit the Foundation’s online IBD1415
Medication guide: www.ibdmedicationguide.org.Additional information is available in our Understanding IBD Medications and Side Effectsbrochure at www.crohnscolitisfoundation.org/brochures.Managing your symptomsThe best way to control Crohn’s disease isby taking medications as prescribed by yourdoctor or other healthcare professional.However, medications may not immediatelyget rid of all the symptoms that you are experiencing. You may continue to have occasionaldiarrhea, cramping, nausea, and fever.Even when there are no symptoms, or justminimal ones, it may still seem like a nuisanceto be on a steady regimen of medication.Remember, though, that taking maintenancemedication can significantly reduce the risk offlares in Crohn’s disease. In between flares, mostpeople feel quite well and are free of symptoms.Talk to your doctor about which over-thecounter (OTC) medications you can taketo help relieve those symptoms. These mayinclude diphenoxylate-atropine (Lomotil )or loperamide (Imodium ) taken as neededto control diarrhea. Most anti-gas productsand digestive aids may also be safe to use,but you should ask your doctor about thesefirst. To reduce fever or ease joint pain,speak with your healthcare provider abouttaking acetaminophen (Tylenol ) rather thannonsteroidal anti-inflammatory drugs (NSAIDs)such as aspirin, ibuprofen (Advil , Motrin ),and naproxen (Aleve ). NSAIDs may irritateyour digestive system. Many over-the-countermedications can have adverse effects on theCrohn’s disease itself or interact with someof the medications prescribed to treat your16Crohn’s disease. The safest way to handleover-the-counter medications is to follow theguidelines and instructions of your doctor andpharmacist.For further information about managingthe symptoms of Crohn’s disease, pleaseread our Managing Flares and Other IBDSymptoms brochure available atwww.crohnscolitisfoundation.org/brochures.Other considerationsSurgeryMany individuals with Crohn’s disease respondwell to medical treatment and never need toundergo surgery. However, between 66 and 75percent of people will require surgery at somepoint during their lives. The overall goal ofsurgery in Crohn’s disease is to conserve boweland return the individual to the best possiblequality of life.Surgery may become necessary when medicaltherapies no longer control the disease or totreat complications. For penetrating disease,surgery may be required to repair a fistula ordrain an abscess. In most cases, the diseasedsegment of bowel is removed. This is called aresection. Usually, the two ends of healthybowel are then joined together in a procedurecalled an anastomosis. While resection andanastomosis may allow many symptom-freeyears, this surgery is not considered a cure forCrohn’s disease because the disease frequentlyrecurs at or near the site of repair.A stoma may be required when surgery is recommended for Crohn’s disease. After surgeonsremove the diseased bowel, they may need tore-route the intestine to the skin and attach anexternal pouch. If the small bowel is used, it iscalled an ileostomy. If the large bowel (colon)17
is used, it is termed a colostomy. A stoma maybe required if the amount of disease and/orinflammation is so severe that an immediateanastomosis is not safe. A colostomy is alsorequired if the rectum is removed. In some instances, the stoma may be temporary and canbe closed in several months once the severeinflammation and/or infection is controlled.For further information on surgery and Crohn’sdisease, please read our Surgery for Crohn’sDisease and Ulcerative Colitis brochureavailable at www.crohnscolitisfoundation.org/brochures.Diet and NutritionOnce the disease has developed, payingattention to your diet may help you reducesymptoms, replace lost nutrients, and promotehealing. Keeping a food diary can be a big help.It allows you to see the connection betweenwhat you eat and the symptoms that mayfollow. If certain foods are causing digestiveproblems, then try to avoid them.There is no single diet or eating plan that willwork for everyone with Crohn’s disease.Dietary recommendations must be tailoredspecifically for you—depending on what part ofyour intestine is affected and what symptomsyou have. Crohn’s disease varies from personto person and even changes within the sameperson over time. What worked for your friendmay not work for you, and even what workedfor you last year may not work for you now.There may be times when modifying your dietcan be helpful, particularly during a flare. Somediets may be recommended at different timesby your physician, including: Low-salt diet—Used during corticosteroidtherapy to reduce water retention. Low-fiber diet—Used to avoid blockages inCrohn’s disease patients with strictures andto avoid stimulating bowel movements in CD. Low-fat diet—Typically recommended duringa flare in Crohn’s disease when fat absorptionmay become an issue. Lactose-free diet—For those who have anintolerance to dairy products. High-calorie diet—For those who experienceweight loss or growth delay. Other diets—There are many other diet plansthat have been tried or suggested for management of Crohn’s disease. These includegluten-free diet, low FODMAP diet, SpecificCarbohydrate Diet, and the Mediterraneandiet. While an individual may benefit from sucha diet, there is no strong evidence to supportrecommending these for broad use at this time.Some patients with IBD may become deficientin certain vitamins and minerals (includingvitamin B-12, folic acid, vitamin C, vitamin D, iron,calcium, zinc, and magnesium) or have troubleingesting enough food to meet their caloricneeds. Your healthcare provider can identify and1819
correct these deficiencies through vitamin andnutritional supplements.Although no specific foods worsen the underlying inflammation of Crohn’s disease, certainones may tend to aggravate the symptoms.Here are some helpful tips: Reduce the amount of greasy or fried foods inyour diet, which may cause diarrhea and gas. Eat smaller meals at more frequent intervals. If you are lactose intolerant, limit the amountof dairy products in your diet. If you are notlactose intolerant, dairy products do not needto be limited. Avoid carbonated beverages if excessive gasis a problem. Restrict caffeine when severe diarrheaoccurs, as caffeine can act as a laxative. Bland, soft foods may be easier to toleratethan spicy foods, although not always. Restricting your intake of certain high-fiberfoods such as nuts, seeds, and raw vegetablesmay decrease your symptoms, especiallyif you have a narrowed segment of bowel.Maintaining proper nutrition is important inthe management of Crohn’s disease. Abdominal pain and fever can cause loss of appetiteand weight loss. Diarrhea can rob the body offluids, minerals, and electrolytes. These are nutrients in the body that must remain in properbalance for the body to function properly.hydra
Living with Crohn’s Disease. 1 Understanding your . diagnosis Your doctor has just told you that you have . Crohn’s disease. Now what? You probably . How will Crohn’s disease change my life, both now and in the future? The purpose of this brochure is to pro