Transcription
Crohn’s Disease &Ulcerative Colitis:A Guide for Parents
What’s Inside?IBD: The basics2Signs and symptoms3Beyond the intestines5Who gets IBD?6Causes of IBD7Diagnosis8TreatmentPrescription medicationOver-the-counter medicationNutrition therapySurgery1010131314Lifestyle modificationsDiet and nutritionDaily activities161617Emotional and social support23Living life26Hope for the future28About CCFAInside back coverYou recently learned that yourchild has Crohn’s disease orulcerative colitis. Now you’retaking an important step:learning about these conditions, how they’re treated,and how your child can learnto live with IBD.The purpose of this brochureis to start you on that educational path—to inform you ofsome key points about Crohn’sdisease and ulcerative colitis,and what you may expect.You won’t become an expertovernight, but gradually you’lllearn more. And the more youknow, the better you’ll beable to become an advocatefor your child. Most important:You’ll be an active member ofyour child’s healthcare team.1
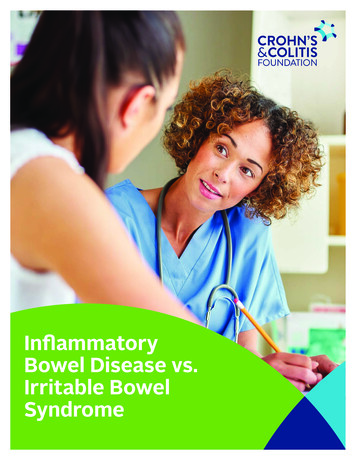
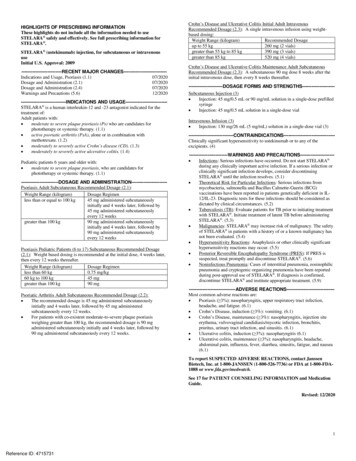
IBD: The basicsIt is important to note, first andforemost, that inflammatorybowel diseases (IBD), specifically Crohn’s disease andulcerative colitis, are chronicbut treatable conditions.Doctors and scientists are working hard to findthe causes of and the cure for IBD. Despite thechallenges of living with a chronic disease, yourchild can have a normal, happy, productive life.While there is not yet a cure for these diseases,appropriate therapy can control the chronic inflammation that is a hallmark of IBD. This willhelp achieve long-term treatment goals, including elimination of chronic gastrointestinalsymptoms, restoration of growth, and a normalquality of life.Crohn’s disease and ulcerative colitis are thetwo most common types of inflammatory boweldiseases. While these conditions produce similar symptoms and use similar therapies, theyare not the same.In ulcerative colitis, only the colon is affected;of the multiple layers of the intestinal wall, onlythe innermost lining of the colon, the mucosa,becomes inflamed in ulcerative colitis patients.Ulcerative colitis also spreads proximally, meaningit starts from the rectum and can spread continuously to the rest of the large intestine (colon).Crohn’s disease, on the other hand, may affectany part of the gastrointestinal (GI) tract, fromthe lips to the anus. Unlike ulcerative colitis,Crohn’s can skip large segments of bowel beforereappearing in others. The areas most often affected, however, are the lower part of the smallintestine (ileum) and the large intestine (colon).Also, in Crohn’s patients, the inflammation doesn’t stop at the mucosa (tissue lining) and mayburrow through the thickness of the bowel wall.Signs and symptomsORAL EINTESTINETERMINALILEUMCECUMAPPENDIXPatients may have one or more symptoms,including:RECTUMANUSFigure 12Despite the differencesbetween Crohn’s diseaseand ulcerative colitis, bothcause similar symptomswhen active—all brought onby chronic inflammation.persistent diarrheaabdominal pain and/or cramps3
fecal urgencyintestinal bleedingfeverweight lossWhile these symptoms are the same in childrenand adults, children also may be affected by adelay in growth and sexual maturation. In fact,a significant number of pediatric IBD patientsare diagnosed after reporting growth delays.This primarily affects Crohn’s patients becauseof the direct effects on bone growth and decreased absorption of nutrients. However, itcan affect all pediatric IBD patients if abdominal pain or other symptoms result in reducedappetite.It is important to understand that these symptoms can vary significantly from patient topatient and do not have to be persistent. Suchsymptoms are only present when IBD is activeand can be eliminated by inducing and maintaining remission and avoiding flare-ups (activesymptoms) of the disease. Symptoms mayappear suddenly and severely and may seemto be triggered by stress or a viral or bacterialillness; they may also build slowly over time.You can learn more about signs and symptomsthrough the following brochures offered onlineat www.ccfa.org:Living with Crohn’s DiseaseLiving with Ulcerative ColitisBeyond the intestinesIn addition to having symptomsin the GI tract, some peoplealso may experience a varietyof symptoms in other parts ofthe body associated with IBD.Signs and symptoms of the disease may beevident in:eyes (redness, pain, and itchiness)mouth (sores)joints (swelling and pain)skin (tender bumps, painful ulcerations,and other sores/rashes)bones (osteoporosis)kidney (stones)liver (primary sclerosing cholangitis, hepatitis,and cirrhosis)—a rare developmentAll of these are known as extraintestinal manifestations of IBD because they occur outside of theintestine. In some people, these actually maybe the first signs of Crohn’s disease, appearingeven years before the bowel symptoms. In others, they may occur right before a flare-up ofthe disease.Managing Flares and other IBD Symptoms45
Who gets IBD?Causes of IBDApproximately 1.4 millionAmericans have either Crohn’sdisease or ulcerative colitis.No one knows for sure whatcauses Crohn’s disease orulcerative colitis, but expertsbelieve there may be severalfactors that work togetherto lead to the developmentof the diseases, including:That number is almost evenly split between thetwo conditions. Here are some quick facts andfigures:More than 1.4 million Americans have IBD.One in ten IBD patients are under the age of 18.On average, people are more frequently diagnosed with Crohn’s disease or ulcerativecolitis between the ages of 15 and 25, although the disease can occur at any age.Males and females appear to be equallyaffected.While IBD can affect those from any ethnicbackground, Caucasians develop it more thanother groups. It is especially prevalent amongthe Eastern European Jewish population.Genes—Studies have shown that 5.2 percentto 22.5 percent of affected individuals mayhave a first-degree relative (i.e., parents/child,siblings) with one of these diseases. Yourgenes clearly play a role, although no specificpattern of inheritance has yet been identified.This means that right now there is no way topredict which, if any, family members maydevelop IBD. A number of genes have beenidentified as possibly playing a role.Environmental elements—Viruses, bacteria,and other factors have been studied withno conclusive results. Researchers are nowfocusing on microscopic elements.Inappropriate immune reactions—Scientistscontinue to study whether a glitch in patients’immune systems—perhaps launched by anenvironmental prompt—may result in the bodyattacking itself.While researchers continue to study possiblecauses, some have been ruled out, includingtension, anxiety, personality traits, or dietaryfactors. Also, the diseases are not consideredto be contagious.67
DiagnosisYour child’s diagnosis ofCrohn’s disease or ulcerativecolitis likely occurred following a few tests.In addition to a thorough medical history andphysical examination, children may undergoa combination of blood tests, barium x-rays,magnetic resonance imaging (MRI), andendoscopy of the upper and lower GI tract. Ingeneral, physicians will begin by prescribingthe least invasive tests, progressing to moreinvasive testing until a diagnosis is obtained.This is especially true in pediatric patients.Blood tests are done to check for a low redcell count (anemia) or high white cell count(inflammation). Other blood tests may beperformed to look for evidence of inflammation in the intestine and elsewhere. Morerecently, various antibody tests have beendiscovered that can show the altered GIimmune process in some people with IBD.Barium x-rays and MRI include the upper GIand small bowel series, which helps to visualize areas of the intestines that are out ofreach of endoscopies (see next bullet).Sometimes, a video capsule may be used toinspect the bowel wall as well. (The lower GIseries, or barium enema, has been replacedby colonoscopy.) During the small bowel series, your child swallows a chalky liquid containing barium or a similar material that coatsthe upper intestinal tract so it will show upon an x-ray or MRI. Areas of swelling, narrowing, or other signs of intestinal inflammationcan be identified with these imaging techniques. X-rays, MRIs, and other imagingtests will be used wisely to limit your child’slifetime exposure to radiation.8Endoscopy is a test that involves insertinga lighted viewing tube through either themouth into the upper intestine (upper endoscopy) or through the anus into the colon(colonoscopy). The physician performing theexam can also remove tiny pieces of tissue(biopsies) from the intestines, which arelater examined for microscopic signs of thediseases. During the endoscopy, your child’sdoctor may also insert a video capsule, whichtakes pictures of the inside of the smallintestine. These pictures can show areas ofsoreness, ulceration, or bleeding that maynot be detectable by other methods. Generally, these tests are performed on childrenwho are sedated. A new form of endoscopy,called the pill endoscopy, does not involveanesthesia. Instead, a patient swallows asmall pill-shaped camera, which takes about50,000 pictures as it travels through the intestines; the images are captured on a devicestored in a belt that the child wears for a day.The camera pill is excreted in the child’s stool.Without appropriate testing, IBD can be difficultto diagnose, because Crohn’s disease andulcerative colitis may look like other conditions.One example of this is irritable bowel syndrome,or IBS. IBS shares many symptoms of IBD, including abdominal pain and diarrhea. However,IBS is a functional bowel disorder, meaning themuscles of the intestines react improperly, eithermoving the bowel contents too quickly or too9
slowly. IBS does not involve inflammation,however. Because there are no physical signsof IBS, it is usually diagnosed after ruling outother conditions, including Crohn’s and colitis.In some individuals, it is difficult to determinewhether their IBD is Crohn’s disease or ulcerative colitis—even after extensive testing. Veryrarely, people are given the diagnosis of “indeterminate colitis.” Such uncertainty is morecommon in the youngest patients—those underfive years old at the time of diagnosis.For in-depth information on diagnostic tests,please see the Diagnosing IBD fact sheetavailable on www.ccfa.org.TreatmentBecause Crohn’s disease andulcerative colitis are considered chronic, meaning thatthey can flare up after aninitial remission, the goal oftreatment is to achieve andmaintain remission.These treatments can include medication,surgery, or nutritional therapies.Prescription medicationWhile there is no medical cure for IBD, there area number of drug therapies that can help yourchild. It is important to understand that just asthe disease impacts each patient differently,medication regimens change from person toperson, sometimes from flare to flare. For example, one individual may have few symptoms andmay respond well to mild drug therapy during10one flare but may require different, stronger medication during a more severe or prolonged flare.Broadly speaking, five different categories oftreatments are used in IBD, both for childrenand adults. These treatments include:Aminosalicylates: These include aspirin-likecompounds that contain 5-aminosalicylate acid(5-ASA) and are used to treat mild-to-moderatedisease or to maintain remission. These drugs,which can be given either orally or rectally,reduce inflammation in the intestine, similarto the way aspirin works against inflammationin other parts of the body such as the joints(arthritis). Possible side effects of aminosalicylates may include diarrhea, headaches, andnausea.Corticosteroids: These medications affect thebody’s ability to launch and maintain an inflammatory process. In addition, they work to suppress the immune system. Corticosteroids areused for children with moderate-to-severe IBD.Administered orally, rectally, or intravenously(through a vein), steroids are effective for shortterm control of flare-ups but are not recommended to maintain remission in children dueto undesirable long-term side effects, includingstunted growth. Some side effects of corticosteroids include weight gain, insomnia, moodswings, osteoporosis, scalp hair loss or facialhair growth, acne, appearance of stretchmarks, and increased susceptibility of infectionand bruising.Immunomodulators: This class of medicationsreduces the activity of the body’s immune system so that it cannot cause ongoing inflammation. Usually given orally, immunomodulatorsgenerally are used in the majority of childrenwith IBD, especially when aminosalicylates andcorticosteroids haven’t been effective or havebeen only partially effective. They may be useful in reducing or eliminating dependency oncorticosteroids and are frequently used tomaintain remission. Immunomodulators may11
Over-the-counter (OTC) medicationcause nausea, a decrease in white and redblood cell counts, and inflammation of the pancreas (pancreatitis) or liver (hepatitis); there isan increased susceptibility to infection relatedto use of these medications. Also, there is asmall increase in the absolute risk of developing certain cancers, such as non-melanomaskin cancers and lymphoma. However, the benefits of long-term remission should be weighedagainst these risks. Your child’s doctor can helpyou to understand the probability of the risksas well as the benefits of the medications.Antibiotics: Certain antibiotics may be used wheninfections, such as abscesses, occur in IBD.Biologic therapies: The newest class of therapiesto be used in IBD are proteins that selectivelytarget key cells in the inflammatory cycle, thusshort-circuiting the process. These therapiesare used to control moderate-to-severe diseaseand to maintain remission. These medicationsare administered by injection or intravenous infusion on a schedule that varies from weekly toevery few months, depending on the individualand the medication.As with all medications, you should know therisks and benefits of these medications anddiscuss any concerns with your child’s doctor.For more information about medications andtheir side effects, download the brochureUnderstanding IBD Medications and Side Effectsfrom www.ccfa.org.12Prescription medications reduce intestinal inflammation and form the core of IBD treatment.Even so, these important prescription medications may not eliminate all of your child’s symptoms. Naturally, you may want your child totake over-the-counter medications in an effortto make him or her feel better. Before doing so,speak with your child’s doctor, or other healthcare professional. Sometimes your child’ssymptoms can indicate a worsening of theinflammation that may require a change inprescription IBD medication or other courseof treatment.Nutrition therapyOptimal nutrition is a goal for well-being anddevelopment in all children, but in those withIBD, this may be difficult to achieve without intervention. Nutrition therapy may be as simpleas regular visits with a nutritionist to ensure dietary goals are being met. The nutritionist mayprescribe higher calorie and protein foods andliquid supplements. Because IBD, especiallyCrohn’s disease, may improve with nutritionalsupport, it may be necessary to provide nutrition by delivering a nutrient-rich liquid formuladirectly into the stomach or small bowel.Known as enteral nutrition, this type of feedingis given overnight through a tube, most commonly from the nose to the stomach. This iscalled a nasogastric (NG) tube. This methodensures that patients receive nutrition whilesleeping. In the morning, they remove the tubeand go to work or school and generally pursuetheir normal activities. In this way, patientsreceive all the nutrition they need and are freeto eat normally—or not—throughout the day.Enteral feedings can also be given through agastrostomy tube (G-tube). A gastrostomy is asurgically created opening through the abdominal wall, leading directly into the stomach. Thefeeding tube is passed through this opening.The feedings are most commonly givenovernight, but they can also be given intermittently throughout the day. Some patients prefer13
this approach because it avoids the discomfortof passing a tube down through the nose.Total parenteral nutrition (TPN) is deliveredthrough a catheter placed into a large bloodvessel, usually one in the chest. Although itbypasses the intestine and thereby allows thebowel to rest, parenteral nutrition may createmore complications than enteral nutrition. It isalso more expensive than the other methods ofnutritional support and requires more specialized training to use.To find more information on nutrition and IBD,be sure to download the brochure Diet andNutrition from www.ccfa.org.SurgeryNo parent ever wants to have their child undergosurgery. In the treatment of IBD, all medicalefforts are aimed at preserving the intestines,especially in children.But there are circumstances when surgery isthe best option or the only alternative. In fact,many Crohn’s patients and a significant percentage of ulcerative colitis patients will reacha point where surgery is the best intervention.The reasons for surgery include:unsuccessful medical control of the diseaselife-threatening colon conditions knownas fulminant colitis and toxic megacolonfistulas and abscesses that are uncontrolledor not healed by medicationstrictures and obstructions, especially thosecaused by scar tissueIn ulcerative colitis, the condition is cured withthe surgical removal of the colon and the liningof the remainder of the rectum, which is not thecase in Crohn’s disease. In many cases, a pouchcan be reconstructed. There is no cure forCrohn’s and the disease may reoccur at the siteof the surgery. In Crohn’s surgery, however, thepatients usually feel much better after the diseased segment of intestines is removed and maybe able to reduce their medications as a result.It is also important to note that newer, minimallyinvasive surgical techniques help patients toheal faster, allowing them to return to their normal activities more quickly.There are a number of surgeries that areperformed in specific circumstances in IBDpatients. To learn more about these surgeries,please download the following fact sheetson www.ccfa.org:perforation of the intestinesSurgery for Ulcerative Colitiscolorectal cancer or risk of itSurgery for Crohn’s Disease1415
Lifestyle modificationsWith IBD, there may be someadjustments you need to helpyour child make, includingaltering his or her diet as necessary or preparing them fordaily activities.Diet and nutritionEvery child needs good nutrition to help him orher grow and develop. While most children withIBD require relatively little or no change in diet,there may be times when modifying the dietcan be helpful, particularly when their diseaseis active. A few different diets may be recommended during different times by your child’sphysician, including a diet with no lactose (asugar found in milk and milk-based products)or a diet with low amounts of insoluble fiber.powders, liquids, and wafers—may representanother therapeutic option for adults with IBD,particularly in helping to maintain remission.Before adding these to your child’s regimen,you should ask your child’s doctor about thesesupplements as he or she may specify specificsupplements for your child.Two things you should remain vigilant aboutare your child’s weight and growth rate. Sinceweight loss is a symptom of a flare-up, any lossin weight should be reported to your child’sphysician. Similarly, growth may slow or ceaseduring periods of disease activity. If you child’sgrowth seems to slow considerably (wears thesame size clothing for more than a year, seemssmaller than other children of the same age, etc.),bring this to the attention of the child’s doctor.For more information, visit www.ccfa.orgto review the material below:Diet and NutritionLiving with Crohn’s DiseaseLiving with Ulcerative ColitisGeneral Healthcare MaintenanceSome children with IBD may become deficientin certain vitamins and minerals (includingvitamin D, B-12, and C; folic acid; iron; calcium;zinc; and magnesium), which may be supplemented. Children with IBD may have troubletolerating iron taken orally; your child’s doctormay prescribe intravenous iron in special cases.Other supplements your child’s doctor mightrecommend are known as probiotics and prebiotics. Probiotics are “good” bacteria that restorebalance to the enteric microflora—bacteria thatlive in everybody’s intestine. Prebiotics arenon-digestible food ingredients that providenutrients to allow beneficial bacteria in thegut to multiply. They also stimulate the growthof probiotics. Mounting evidence suggests theuse of probiotics—available in capsules,16Your child should continue to see a pediatricianto help monitor their physical development andmake sure they are up to date with vaccinations,including annual flu vaccines. Make sure thisphysician is fully informed about your child’smedications, as children on immunosuppressive or biologic therapies should not receivelive virus vaccines.Daily activitiesNow that your child has a disease that causesa greater reliance on the bathroom, you shouldplan for more time in any activity schedule forbathroom breaks. You may also want to encourage your child to review bathroom locationsin malls, playgrounds, movie theaters, or other17
regularly used areas outside of your home.Doing so can help your child feel more incontrol about their condition.Children with IBD may have a greater relianceon bathrooms and thus need open bathroompasses or access.Some states have created laws that allow accessto “employee only” restrooms in businessesopen to the public. Call your local CCFA chapterto see if your state has passed the RestroomAccess Act. If so, make sure your child has therequired physician’s note describing your child’sneed for immediate bathroom access any timehe or she ventures out. During times of flareups, it may also help to pack a spare change ofclothing and some moist wipes in a backpackfor your child to carry.Certain medications may need to be takenduring the school day.SchoolBecause children spend most of their wakinghours in school, adults who tend to your childat school should be told about your child’sillness for several reasons, including:IBD may lead to more frequent absences orhospitalizations; make-up work and othereducational needs may need to be addressed.Plan to establish a Section 504 plan or individualized education program (IEP) for yourchild. Section 504 of the Rehabilitation Act of1973 provides that disabled students cannotbe denied benefits of any public program including education. Within an IEP, your childcan benefit from special “accommodations”that help to improve the quality of his or hereducational experience and ensure socialinteraction with other students. (See “Schoolaccommodations,” page 20.)Requesting a meeting with administrators andteachers to discuss the illness and your child’sneeds is a proactive way of dealing with potential future issues caused by IBD.While informing the administrators and teachersabout your child’s needs is necessary, yourchild may feel embarrassed about letting others know. Because it may be important to himor her, let your child decide with whom andwhen to share that information with others.Access other related resources that maybe helpful to you at www.ccfa.org:A Guide for Kids and TeenagersA Guide for Teachers and Other SchoolPersonnelPete Learns All About Crohn’s and ColitisIBD & Me Activity Book1819
School accommodationsIf your child is falling behind in school, orrequires special accommodations to maintaintheir academic performance, he or she maybenefit from a 504 plan or an individualizededucation program (IEP). Two federal laws,Section 504 of the Rehabilitation Act of 1973and the Individuals with Disabilities EducationAct, provide protection for public school studentswith disabilities. Although both laws apply tostudents with disabilities, not all students withdisabilities qualify for the protections of bothlaws. Each law has specific eligibility requirements and guidelines for services.504 Plan: This comes from Section 504 of theRehabilitation Act of 1973. This act requiresrecipients of federal education funding toprovide children with disabilities appropriateeducational services designed to meet theindividual needs of such students, to thesame extent as the needs of students withoutdisabilities are met. A 504 plan spells out themodifications and accommodations that willbe needed for these students to have anopportunity to perform at the same level astheir peers, and might include such thingsas blood sugar monitoring, an extra set oftextbooks, or home instruction. A Section504 plan involves an evaluation of the child’sdisability as well as his or her academic abilities and specific provisions to help the childreach his or her academic potential.Individuals with Disabilities Education Act(IDEA): First passed as the Education for allHandicapped Children Act in 1974 and mostrecently amended in 2004, the act governshow states and agencies provide certain educational services to children with disabilities,including children with health impairmentslike IBD. For students with disabilities whorequire specialized instruction, the IDEA controls the procedural requirements. The IDEAprocess is more involved than that requiredunder Section 504. One of the provisions of20the act requires schools that receive publicfunding to create an IEP for each child coveredby the plan, ensuring that the unique needsof the child are met in the least restrictiveenvironment. The “individualized” part of IEPmeans that the plan has to be tailored specifically to your child's special needs. IDEAcovers children with disabilities from birthto age 21.Informal (verbal arrangement with a teacher)and formal accommodations (items coveredunder a 504 plan or IEP) for a child may helpthem reach and maintain their academic potential. Here are some formal and informal sampleaccommodations that may be helpful for yourchild. Accommodations should be requestedas soon as possible, preferably in the beginning of the school year, so that there is time tomake necessary arrangements and formalizeplans. Remember: even if your child is perfectlyhealthy at the start of a school year, they maystill need some of the accommodations belowin the course of the year. It is always best toplan ahead! These are some potential accommodations—others may be added to meet theneeds of your child.Unlimited bathroom pass: Students withactive disease symptoms may need to use thebathroom many times per day—often urgentlyin order to avoid fecal incontinence. Studentand teacher should work out an appropriatebathroom signal to help avoid drawing attention to the student’s frequent bathroombreaks.“Stop the clock” testing: When taking anexam, the student may need to take a breakdue to pain or bowel urgency. Their test timewill be extended by the amount of time thatthe student is away from the exam.Ability to hydrate: Frequent bowel movementsand medication contribute to loss of fluids.Students should be allowed to carry and drinkfluids throughout the day.21
Supply bag: Student will be permitted tocarry and eat small snacks, candy (to treatdry mouth), wet wipes, and other suppliesthroughout the day and use as needed.Tests and project limits: Medications andactive disease symptoms may contribute tosleep deprivation and fatigue. As a result, thenumber of tests and projects can be limitedto one to two per day. Test and project deadlines can also be extended without penalty.Rest period: School nurse will provide a location as needed for students to lie down, or aprivate place to change clothes.School absence: After a specified numberof days absent from school, the student willreceive in-home or hospital tutoring.Alternate Seating: To accommodate easyaccess to classroom exits, the student’s seatmay be changed.Medications: The student, parent, and nursewill meet to discuss and establish a medication schedule.Tutoring and support: If the student is absentfor more than “x” days from school, he/shewill have an opportunity to make up or getassistance with assignments. Students will beallowed to have an extra set of books at home.Extra-curricular programs: The student willbe allowed to participate in programs andevents without penalty due to absenteeism.Physical education class: The student shouldbe allowed to self-monitor his/her energylevel to determine if he or she can participatein physical activities. The physical educationteacher will notify their parents if there is ongoing non-participation in gym class.To learn more about school accommodations,please call our IRC at 888-694-8872.22Physical activitiesYoung people with IBD should be as active aspossible. Outside of the physical benefits, including building stronger muscles and bones,these activities provide an outlet for stress andcan help build confidence.Generally, there is no reason not to participatein sports, dance, or other physical activities,even if the disease is flaring up. But some modifications may be necessary if strenuous activities cause fatigue or aggravate abdominal pain,arthritis, or other symptoms. You and your childshould also be vigilant about maintainingproper hydration.Furthermore, prolonged high-dose steroid therapy may make bones more susceptible to fractureduring contact sports, such as football andwrestling. In these instances, a modified exerciseprogram may be advisable.Emotional and socialsupportThe diagnosis of a chronic illness can be a tough blow foranyone, but for children, itcan be especially hard to bear.Still developing a sense of themselves bothemotionally and physically, young people nowmust face an extra hurdle of chronic illness,which can pose a threat to a child’s sense ofwell-being and secur
exam can also remove tiny pieces of tissue (biopsies) from the intestines, which are later examined for microscopic signs of the diseases. During the endoscopy, your child’s doctor may also insert a video capsule, which takes pictures of the inside of the small intestine. These pictures can