Transcription
6/17/2021CPT SPINAL FUSIONVanessa Youmans, MA, RHIA, CCS, CPCDirector, Outpatient & ProFee ServicesYES HIM Consulting, Inc.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYDISCLAIMERA l l r e s p o n s e s , a d v i c e , a n d e d u c a t i o n a l m a t e r i a l s a r e d e s i g n e d t o p r o v i d e a c c u r a t e c o d i n g i n f o rm a t i o n . E v e r y e f f o rth a s b e e n m a d e t o e n s u r e a c c u ra c y. H o w e v e r, e a c h h e a l t h ca r e p r o v i d e r, c o n su l t i n g c o m p a n y, o r i n d i v i d u a l c o n t ra c t o ri s r e s p o n si b l e f o r c o r r e ct c o d i n g & b i l l i n g a n d a s s u m e s a l l r i s k a n d l i a b i l i t y i n c o n n e c t i o n w i t h t h e u s e o f t h ei n f o r m a t i o n . Y E S H I M C o n s u l t i n g , I n c . i s n o t l i a b l e f o r a n y d i r e c t , i n d i re c t , s p e c i a l , c o n s e q u e n t i a l , o r o t h e r d a m a g e so r e c o n o m i c l o s s a r i s i n g f r o m u s e o f t h e i n f o r m a t i o n p r o v i d e d . Th e r e i s n o r e p r e s e n t a t i o n , w a r ra n t y, o r g u a ra n t e et h a t a n y r e s p o n s e , a d v i c e , o r p r o v i d e d m a t e ri a l i s e r r o r -f r e e .AH A C o d i n g C l i n i c i s c o p yr i g h t e d s o o n l y h i g h l i g h t s , e xa m p l e s , o r e xc e r p t s a r e p r e s e n t e d o r m e n t i o n e d f o re d u c a t i o n a l p u r p o s e s . W e e n c o u r a g e a l l h e a l t h ca r e f a c i l i t i e s , c o n s u l t i n g c o m p a n i e s , o r i n d i vi d u a l c o n t r a c t o rs t os u b s c r i b e t o A H A C o d i n g C l i n i c o r t o h a v e f u l l a c c e s s t o A H A C o d i n g C l i n i c t h r o u g h y o u r e n c o d e r o r C A C v e n d o r.Yo u a r e e n c o u ra g e d t o r e s e a r c h a n y e xa m p l e s p r e s e n t e d i n t h e f u l l v e r s i o n o f A H A C o d i n g C l i n i c .C P T C o p y r i g h t 2 0 2 1 A m e ri c a n M e d i c a l A s s o c i a t i o n . A l l r i g h t s r e s e r v e d . C P T i s a r e g i st e re d t r a d e m a r k o f t h eA m e r i c a n M e d i ca l A s s o c i a t i o n . . T h e A M A a s s u m e s n o l i a b i l i t y f o r t h e d a t a c o n t a i n e d h e r e i n . C P T c o d e s a n d AM AC P T As s i s t a n t a r e c o p yr i g h t e d s o o n l y h i g h l i g h t s , e xa m p l e s, o r e xc e r p t s a r e p r e s e n t e d o r m e n t i o n e d f o r e d u c a t i o n a lp u r p o se s . W e e n c o u r a g e a l l h e a l t h c a re f a c i l i t i e s , c o n s u l t i n g c o m p a n i e s, o r i n d i v i d u a l c o n t r a c t o r s t o a c c e s s A M A C P Tc o d e b o o k s o r t o h a v e f u l l a c c e s s t o A M A C P T c o d e s a n d A M A C P T A s s i s t a n t t h r o u g h y o u r e n c o d e r o r C A C v e n d o r.Yo u a r e e n c o u ra g e d t o r e s e a r c h a n y e xa m p l e s p r e s e n t e d i n t h e f u l l v e r s i o n o f A M A C P T c o d e b o o k s a n d / o r A M A C P TAssistant.C o p y r i g h t 2 0 2 1 b y Y E S H I M C o n s u l t i n g , I n c . A l l r i g h t s r e s e rv e d . N o p a r t o f t h i s p r e s e n t a t i o n m a y b e r e p r o d u c e d i na n y f o r m w h a t s o e ve r w i t h o u t p e r m i s si o n f r o m Y E S H I M C o n s u l t i n g , I n c .YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY1
6/17/2021Webinar ObjectivesCPT CODING – SPINAL FUSIONSpinal Anatomy and Disease Process ReviewSpinal Arthrodesis ProcedureSpinal Fusion Case Studies – Cervical and ThoracicSpinal Fusion Case Studies – Lumbar and Spinal DeformityYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYSPINAL ANATOMY &DISEASE PROCESSREVIEWhttps://www.istockphoto.com/YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY2
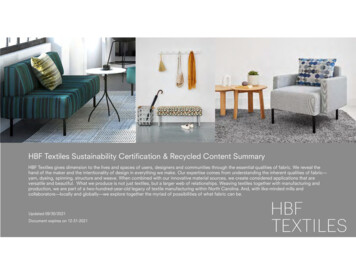
6/17/2021REVIEW: ANATOMY OF THE SPINECervical – C1-C7Thoracic – T1-T12Lumbar – L1-L5Sacral – S1-S5https://en.wikipedia.org/wiki/File:Gray 111 Vertebral column-coloured.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYREVIEW: ANATOMY OF THE SPINEhttps://en.wikipedia.org/wiki/File:718 Vertebra-en.svgYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY3
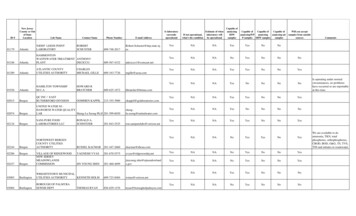
6/17/2021DIAGNOSES FOR ARTHRODESIS Disc Disorders Degenerative Disc Disease Spinal Disc Herniationhttps://en.wikipedia.org/wiki/Spinal disc herniation#/media/File:Herniated Disc.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYDIAGNOSES FOR ARTHRODESIS Spinal StenosisSpondylolisthesisVertebral inal Stenosis.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY4
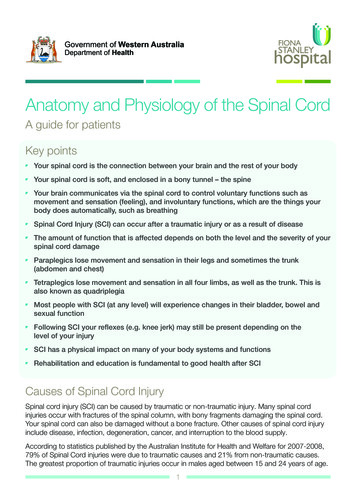
6/17/2021DIAGNOSES FOR ARTHRODESIS Scoliosis Kyphosishttps://en.wikipedia.org/wiki/File:Blausen 0785 Scoliosis01.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYSPINAL FUSION - ARTHRODESISPermanently join together two or more bones in the spineso there is no movement between themhttps://en.wikipedia.org/wiki/File:Blausen 0446 HarringtonRods.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY5
6/17/2021INTERBODY FUSIONThe part of the spine where the disk is present, e:ACDF oblique annotated english.svgYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYFrom the Front: Anterior – Example:Anterior Lumbar Interbody Fusion (ALIF)APPROACHESFOR SPINALFUSIONYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYFrom the Back: Posterior – Example:Posterior Lumbar Interbody Fusion (PLIF)Transforaminal: Posterior and throughthe side – Example:Transforaminal Lateral Interbody Fusion(TLIF)From the Side: Lateral – Example:Direct Lateral Interbody Fusion (DLIF) &Extreme Interbody Fusion (XLIF)6
6/17/2021BONE GRAFT FOR SPINAL FUSIONBone Graft Used to Form Fusion: Autograft – from the patient Allograft – from another patient Synthetic – en 0096 BoneGraft.pngYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYINSTRUCTIONS & INTERBODY FUSION DEVICESFixation Devices: Rods, Screws, Plates Stabilize while bone heals and growsInterbody Fusion Devices: Packed with bone grafthttps://en.wikipedia.org/wiki/File:Roe LWS Spondylodese L5-S1 seitlich.jpghttps://www.bing.com/images/search?q imgurl%3ahttp%3a%2f%2feorthopod.com.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY7
6/17/2021REFERENCES The American Academy of Orthopaedic Surgeons:“Spinal Fusion Terms and Glossary - OrthoInfo - AAOS.” OrthoInfo, sary/. Spine-Health:Paul McAfee, MD. “Indications for Spinal Fusion.” Spine, Spine-Health, tions-spinal-fusion. “Spinal Fusion.” Wikipedia, Wikimedia Foundation, 7 May 2021, en.wikipedia.org/wiki/Spinal kipedia.org/wiki/File:Gray 111 - Vertebral ile:718 l disc herniation#/media/File:Herniated Disc.pnghttps://en.wikipedia.org/wiki/File:Spinal usen 0785 Scoliosis 01.pnghttps://en.wikipedia.org/wiki/File:Blausen 0446 le:ACDF oblique annotated sen 0096 e LWS Spondylodese L5-S1 seitlich.jpghttps://www.bing.com/images/search?q ult%2ffiles%2fimages%2flumbar fusion cage surgery03.jpg&view detailv2&iss sbi&rtpu %2fsearch%3fq%3dwikipedia cages for spinal surgery&FORM IEQNAIYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYSPINALARTHRODESISPROCEDURECPT CODES &GUIDELINEShttps://www.canva.com/YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY8
6/17/2021CPT CODES & GUIDELINESArthrodesis(AKA Spinal Fusion):surgery to permanently jointogether two or more bones inthe spine so there is nomovement between them.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYARTHRODESIS –CODED SEPARATELYBONE GRAFTING PROCEDURES 20930-20938 Add-on codes If more than one type, code for each type - once per each operativesession * Examples: 20930 morselized allograft or placement of osteopromotive material forspinal surgery 20936 autograft for spine surgery obtained from the same incision local(for example ribs, spinous process, laminar fragments)BONE MARROW ASPIRATION FOR BONE GRAFTING –SPINAL SURGERY 20939*CPT Assistant, April 2012YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY9
6/17/2021ARTHRODESIS –CODED SEPARATELYSPINAL INSTRUMENTATION Non-segmental – 22840 Posterior - can span several segments* Segmental – 22842-22847 Posterior – 22842-22844 Anterior – 22845-22847Photo courtesy of TruCode*CPT Assistant, January 2011YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYSegmental InstrumentationPhoto courtesy of TruCodeYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY10
6/17/2021Vertebral Interspace – non-bonycomponent between 2 adjacent vertebralbodiesINTERSPACESANDSEGMENTSVertebral Segment – single completevertebral bone with its associated articularprocesses and laminaeExample Fusion of L3-L5: 2 interspaces – between L3 and L4,and L4 and L5 3 segments – L3, L4, L5YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYARTHRODESIS –CODED SEPARATELY Interbody and Intervertebral biomechanical devices- example syntheticcage, mesh 22853 - device placed into a discectomy defect for purposes of spinalfusion, each interspace 22854 - device placed into a corpectomy defect for purposes of spinalfusion, each contiguous defect 22859 - device placed into a discectomy or corpectomy defect withoutspinal fusion, each contiguous defect Codes include instrumentation necessary for device anchoring asapplicable – posterior or anterior instrumentation to stabilize spinalsegment(s) separately reportable*CPT Assistant, March 2017Photo courtesy of TruCodeYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY11
6/17/2021Includes minimal discectomy to prepareinterspace – other than ITY22532 - thoracic22533 - lumbar22534 - each additional segment,thoracic or lumbarYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYARTHRODESIS APPROACHANTERIOR ORANTEROLATERAL Photo courtesy of TruCode22548 - C1-C222551 - Cervical below C2 - includes decompression22552 - Add-on code for 2255122554 - Cervical below C2 - other than decompression, singleinterspace22556 - single interspace - thoracic22558 - single interspace - lumbar22585 - add-on code for 22554, 22556, 22558See image on page 136 for anterior approach for lumbar fusionYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY12
6/17/2021ARTHRODESIS – POSTERIOR, POSTEROLATERALOR LATERAL TRANSVERSE PROCESS TECHNIQUEPOSTERIOR ORPOSTEROLATERL22590-22614 22590 - posteriorcraniocervical 22595 - posteriorC1-C2 22600 - posterior orposterolateral below C2 22610 - posterior orposterolateral thoracic 22612 - posterior orposterolateral lumbarPosterior interbodytechnique – includinglaminectomy and/ordiscectomy (otherthan fordecompression,lumbar -22630 and 22632Combined posterioror posterolateral withposterior interbodytechnique includinglaminectomy and/ordiscectomy (otherthan fordecompression,lumbar - 22633 and 22634YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYADD-ON CODES ARTHRODESIS – POSTERIOR,POSTEROLATERAL OR LATERAL TRANSVERSE PROCESSTECHNIQUE226142263222634Each additionalvertebral segment used in conjunctionwith 22600, 22610,22612, 22630 or22633 whenperformed on adifferent levelEach additionalinterspace - posteriorinterbody fusion used in conjunctionwith 22612, 22630,22633 whenperformed on adifferent levelEach additionalinterspace andsegment - use with22633 for combinedposterior orposterolateral withposterior interbodyYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY13
6/17/2021ARTHRODESIS FORSPINE DEFORMITYFOR EXAMPLE, SCOLIOSIS OR KYPHOSISCODED SEPARATELY: Bone Graft InstrumentationBASED ON APPROACH AND NUMBER OF SEGMENTS 22800-22804 - posterior 22808-22812 - anteriorYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYMODIFIERS – PROFEE BILLING62 TWO SURGEONS – EACH SURGEON REPORTS 62 Not appended to bone graft or instrumentation codes51 MULTIPLE PROCEDURES When arthrodesis is performed in addition to another procedure, such asfracture care, vertebral corpectomy 51 modifier is added to arthrodesiscode Does not apply to add-on codes, for example 22585 (anterior interbodyarthrodesis) each additional interspaceYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY14
6/17/2021REFERENCES CPT 2019 Professional Edition. American Medical Association, 2019. CPT Assistant Online - American Medical Association. sp?product id prod270004&navAction push. January 2011, April 2012, April 2016,March com/images/search?view detailV2&ccid pSbeJS56&id FB7789E4BE2B9375C4C7C8696043DD057D9F7AC1&thid OIP.pSbeJS56PY1eKEqJxAgJrwHaJK&mediaurl -2019-professionaledition-ama-9.jpg&exph 835&expw 675&q cpt assistant 2019&simid 608029722830900178&selectedIndex 0YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCASE STUDIESCERVICAL ANDTHORACIC FUSIONhttps://www.canva.com/YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY15
6/17/2021REVIEWING SPINAL FUSION CASESWhat part of thespine was involved?What was theapproach?What specificprocedures wereperformed and forwhat reason(s)?What type ofinstrumentation?What type of bonegrafts? Cervical, Thoracic, Lumbar? Sacral? Combined? Anterior? Posterior? Lateral extracavity? Spinal stenosis, disc disorders, spinal deformity? Discectomy, arthrodesis, decompression, corpectomy, combination? Non-segmental, segmental-posterior or anterior Autograft, allograft?YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCERVICAL FUSION CASEPREOPERATIVE DIAGNOSES: C2-3 dynamic instability, worsening neck painPOSTOPERATIVE DIAGNOSES: SamePROCEDURE PERFORMED:1. C2 to C4 posterior cervical segmental arthrodesis.2. Posterior cervical instrumentation with C2 pars screws, as well as C3 and C4 lateral mass screws, using the StrykerOASYS system.3. Use of BIO4 allograft.4. Harvest of local bone autograft from spinous processes.5. Bone marrow aspiration from right superior posterior iliac crest via separate stab incision.6. Use and interpretation of neurophysiologic monitoring.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY16
6/17/2021CERVICAL FUSION CASE (CONTINUED)INDICATIONS: This 59-year-old female has been experiencing worsening neck pain and was diagnosed with C2-3anterolisthesis with evidence of dynamic instability Posterior cervical instrumented fusion was recommended to stabilizeher cervical spine. The risks, benefits, and alternatives to surgery were reviewed at length with the patient and spouse.Risks include but are not limited to bleeding, infection, need for future procedures including extension of fusion;pseudoarthrosis, failure of implants, permanent neurologic deficit such as numbness, weakness; wound problems,medical complications, and even stroke, coma, paralysis, and death. The patient acknowledged these risks, allquestions were answered, and she asked to proceed.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCERVICAL FUSION CASE (CONTINUED)DESCRIPTION OF PROCEDURE: The patient was brought to the operating room where she was intubated andsedated by the Anesthesia team without incident. Neurophysiologic monitoring was set up, and she was then flipped tothe prone position with her head secured in a 3-point Mayfield device. Post-flip neurophysiologic data remained stable.Intraoperative fluoroscopy was used to mark the appropriate level for the skin incision. The skin was sterilely preppedand draped in standard fashion. A final timeout was performed to verify the correct patient, procedure, and surgical site.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY17
6/17/2021CERVICAL FUSION CASE (CONTINUED)A 15-blade was used to make a midline posterior cervical incision from approximately C2 to C4. The Bovieelectrocautery continued the soft tissue dissection down to the posterior cervical fascia. The dissection then continued inthe midline avascular plane down to the C2 to C4 spinous processes. A subperiosteal dissection was performed toexpose the C2 through C4 lamina and lateral masses. A Penfield 1 dissector was used to continue the dissection toexpose bilateral C2 pars. Care was taken not to disrupt the C1-2 or C4-5 facet joints.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCERVICAL FUSION CASE (CONTINUED)Intraoperative fluoroscopy was used to confirm the appropriate starting point along C2 for the C2 pars screws. A pilothole was made with the high-speed drill. Screw trajectories were drilled under direct fluoroscopic guidance, as well aswith direct visual confirmation of the medial border of the pars. The screw trajectories were tapped and a ball-tip probeconfirmed no breaches. A 3.5 x 18 mm biased-angle screw was placed on the right, while a 3.5 x 16 mm biased-anglescrew was placed on the left.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY18
6/17/2021CERVICAL FUSION CASE (CONTINUED)Attention was then turned towards the C3 and C4 lateral mass screws. Of note, the patient had particularly small lateralmasses, which thereby necessitated extending the fusion down to C4 in order to ensure a greater purchase.Intraoperative fluoroscopy was again used to confirm appropriate starting points. The high-speed drill was used tocreate pilot holes in bilateral C3 and C4 lateral masses. A hand-twist drill was then used to drill the screw trajectoriesaccording to the Magerl technique. The trajectories were tapped and the ball-tip probe again ensured no breaches.Then, 3.5 x 10 mm biased-angle screws were placed bilaterally at C3 and, on the left at C4, a 3.5 x 14 mm biased-anglescrew was placed on the right at C4 and was left somewhat proud, as this lateral mass was quite deeper whencompared C3.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCERVICAL FUSION CASE (CONTINUED)Next, 40 mm titanium alloy rods were placed within the tulip heads, where they were secured with cap screws. AP andlateral x-rays confirmed appropriate positioning of all screws and the cap screws were then final tightened.A stab incision was made over the right posterior superior iliac crest with a 15 blade. A Jamshidi needle was tapped intoplace in order to aspirate approximately 5 mL of bone marrow aspirate. The bone marrow aspirate was combined with 5mL of BIO4 allograft, as well as bone which had been morselized from the C2 through C4 spinous processes. TheJamshidi needle was removed in its entirety and the stab incision was covered with Dermabond.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY19
6/17/2021CERVICAL FUSION CASE (CONTINUED)The facet joints and lateral masses were decorticated with a high-speed drill. BIO4 allograft was then packed into agreatly expanded left C2-3 facet joint after its cartilaginous surface had been disrupted. The remaining BIO4 andautograft were then packed laterally adjacent to the rod, as well as over the previously decorticated lamina from C2 toC4. The wound was irrigated with copious amounts of antibiotic-containing solution. Exquisite hemostasis wasachieved with the bipolar. The wound was then closed in layers using 0 Vicryl for the muscle and fascia, followed by 2-0Vicryl for the subcutaneous tissue, 3-0 Vicryl for the dermis, and lastly a running 3-0 nylon on the skin. All counts werecorrect x2 at the conclusion of the procedure. No apparent complication was noted. The neurophysiologic monitoringremained stable throughout the entire case.The patient was extubated in the operating room and transported to the recovery area in stable condition.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYREVIEW THE DOCUMENTATIONWHAT PART OF THE SPINE WAS INVOLVED? CervicalWHAT WAS THE APPROACH? PosteriorWHAT SPECIFIC PROCEDURES WERE PERFORMEDAND FOR WHAT REASON(S)? Cervical arthrodesis for worsening neck painWHAT TYPE OF INSTRUMENTATION? Segmental-posteriorWHAT TYPE OF BONE GRAFTS? Local bone graft from spinous process and aspiration from iliac crest,BIO4 allograftYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY20
6/17/2021CERVICAL FUSION CASE CODES1. C2 to C4 posterior cervical segmental arthrodesis22600Posterior fusion single level below C2 segment (C2-C3) 22614 Posterior fusion additional vertebral segment (C3-C4)2. Posterior cervical instrumentation with C2 pars screws, as well as C3 and C4 lateral mass screws, using theStryker OASYS system. 22842 Posterior segmental instrumentation 3-6 vertebral segments (C2-C4)3. Use of BIO4 allograft.4. Harvest of local bone autograft from spinous processes.5. Bone marrow aspiration from right superior posterior iliac crest via separate stab incision 20930 Allograft, morselized, for spine surgery only 20936 Autograft for spine surgery same incision - includes harvest, local 20939-RTBone marrow aspiration for bone grafting for spine surgery - separate incisionYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYTHORACIC FUSION CASEDIAGNOSIS: Pathology showed metastatic epidural adenocarcinoma, unknown primaryPROCEDURES PERFORMED:1. Spinal neuronavigation with Stealth Medtronic neuronavigation.2. Spinal instrumentation with pedicle screws and rods bilaterally at the level of T7, T8, T9, T10, a total of 4 levels ofthoracic instrumentation.3. Laminectomy for resection of spinal epidural tumor at the level of T7, 8, 9, and 10, a total of 4 levels, laminectomyfor tumor resection.4. Bilateral posterolateral arthrodesis with high-speed drill, decortication, and allograft morcellized at the level of T7-T8,T8-T9, T9-T10, a total of 3 levels, bilateral posterolateral arthrodesis.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY21
6/17/2021THORACIC FUSION CASE (CONTINUED)DESCRIPTION OF PROCEDURE: Patient was induced under general anesthesia, and an endotracheal tube wasplaced. The patient was then placed in the prone position on Jackson frame. All the pressure points were padded. Iproceeded to localize the levels of T7 to T10 with lateral fluoroscopy, and I marked my incision in the midline.After adequate time-out and after adequate administration of preoperative antibiotics, Decadron as IV, and keeping themean arterial pressure above 90 at all times, I proceeded to make my incision with a 10 blade and achieved adequatesharp dissection through the dermis, subcutaneous tissue, and fascia with monopolar cautery and performedsubperiosteal dissection of the multifidus muscle off the spinous process, lamina, and facets bilaterally at the level of T7,T8, T9, T10, including the transverse processes.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYTHORACIC FUSION CASE (CONTINUED)At this time, I proceeded to perform a laminectomy at T7, 8, 9, and 10, a 4-level laminectomy, for excision of epiduraltumor, finding tumor along the inferior aspect of T8, full aspect of T9, and partially T10, epidural tumor intimatelyattached to the dura, if not invading the dura on the left side, and mostly on the left side, displacing the spinal cordtowards the right side. Tumor was removed, and I saw the tumor was invading the dura mostly on the left side. Therewas a small amount of spinal fluid leak, which was repaired with fat graft and dural sealant. Adequate hemostasis wasachieved with bipolar coagulation and FloSeal.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY22
6/17/2021THORACIC FUSION CASE (CONTINUED)After resection of epidural tumor and dural repair, I proceeded to perform an intraoperative CT scan with the O-arm toobtain 3D landmarks for neuronavigation after placing a clamp on the spinous process of T7. We proceeded to placebilateral pedicle screws at the level of T7, bilateral pedicle screws at the level of T8, right-sided pedicle screw at the levelof T9, and bilateral pedicle screws at the level of T10. These were placed under neuronavigation with Stealth spinalneuronavigation, and placement of hardware was confirmed with another O-arm spin, intraoperative CT scan confirmingadequate placement of hardware. After this, one rod was placed on each side, secured to the screw heads with the useof set screws, and the construct was finalized and locked. After the construct was finalized, posterolateral arthrodesisbilaterally with high-speed drill, decortication, and placement of morcellized allograft placed bilaterally at the level of T7T8, T8-T9, and T9-T10, three levels total.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYTHORACIC FUSION CASE (CONTINUED)Two #10 JP flat drains were placed in the epidural space through 2 separate incisions. The drains were secured to theskin with the use of Vicryl stitches, and then after copious irrigation with bacitracin irrigation and adequate hemostasiswith bipolar coagulation and FloSeal, I proceeded to perform closure of the fascia with interrupted sutures of 0 Vicryl,closed this with the interstitial dermis with interrupted sutures of 2-0 Vicryl, and the skin was closed with a running 4-0Rapide reabsorbable suture. The area was dressed in sterile fashion. The patient was allowed to wake up, extubated,and transferred to the postoperative area for further postop care. Family will be updated, and the count was correct.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY23
6/17/2021REVIEW THE DOCUMENTATIONWHAT PART OF THE SPINE WAS INVOLVED? Thoracic, T7-T10WHAT WAS THE APPROACH? PosterolateralWHAT SPECIFIC PROCEDURES WERE PERFORMEDAND FOR WHAT REASON(S)? Thoracic arthrodesis and removal of metastatic epiduraladenocarcinomaWHAT TYPE OF INSTRUMENTATION? Segmental-posteriorWHAT TYPE OF BONE GRAFTS? AllograftOTHER PROCEDURES? NeuronavigationYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYTHORACIC FUSION CASE CODES1. Spinal neuronavigation with Stealth Medtronic neuronavigation. 61783 Stereotactic navigational procedure spinal2. Spinal instrumentation with pedicle screws and rods bilaterally at the level of T7, T8, T9, T10, a total of 4levels of thoracic instrumentation. 22842 Posterior segmental instrumentation 3-6 vertebral segments3. Laminectomy for resection of spinal epidural tumor at the level of T7, 8, 9, and 10, a total of 4 levels,laminectomy for tumor resection.63276Laminectomy excision of extradural thoracic intraspinal neoplasm4. Bilateral posterolateral arthrodesis with high-speed drill, decortication, and allograft morcellized at the levelof T7-T8, T8-T9, T9-T10, a total of 3 levels, bilateral posterolateral arthrodesis.22610Arthrodesis, posterior or posterolateral technique, single level; thoracic (with lateral transverse technique,when performed) 22614 X 2Arthrodesis, posterior or posterolateral technique; each additional vertebral segment (Listseparately in addition to code for primary procedure) 20930 Allograft, morselized, or placement of osteopromotive material, for spine surgery only (List separately inaddition to code for primary procedure)Note: Modifier 51 for 22610 for ProFeeYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY24
6/17/2021REFERENCES CPT 2019 Professional Edition. American Medical Association, 2019. CPT Assistant Online - American Medical Association. sp?product id prod270004&navAction push. January 2011, April 2012, April 2016,March com/images/search?view detailV2&ccid pSbeJS56&id FB7789E4BE2B9375C4C7C8696043DD057D9F7AC1&thid OIP.pSbeJS56PY1eKEqJxAgJrwHaJK&mediaurl -2019-professionaledition-ama-9.jpg&exph 835&expw 675&q cpt assistant 2019&simid 608029722830900178&selectedIndex 0YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYCASE STUDIESLUMBAR ANDSPINAL DEFORMITYhttps://www.canva.com/YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY25
6/17/2021LUMBAR FUSION CASE EXCERPTSPREOPERATIVE DIAGNOSES:1. Mechanical lower back pain.2. Intractable right lumbar radiculopathy and radiculitis.3. Grade 1 lumbar 4-5 spondylolisthesis.4. Lumbar 4-5 instability.POSTOPERATIVE DIAGNOSES: SameYES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARYLUMBAR FUSION CASE (CONTINUED)PROCEDURES PERFORMED:1. Minimally invasive instrumented lumbar 4-5 fusion with placement of bilateral pedicle screws across L4-52. Arthrodesis lumbar 4-53. Open reduction of grade 1 lumbar 4-5 spondylolisthesis.4. Transforaminal lumbar interbody fusion, lumbar 4-5, with placement of Tritanium PL spacer and allograft.5. Right lumbar 4-5 microdiskectomy.YES HIM Consulting, Inc. 2021 CONFIDENTIAL AND PROPRIETARY26
6/17/2021LUMBAR FUSION CASE (CONTINUED)INDICATIONS FOR SURGERY: This 63-year-old presented complaining of a multi-year history of mechanical lowerback pain, as well as progressive right lower extremity radicular pain. Unfortunately, the patient has failed multipleconservative modalities consisting of not only a dedicated course of physical therapy, but also epidural steroid injectionsx4. She describes her back pain as dull and aching in nature. She also proclaims to have significant pain in the rightleg which will radiate posterolaterally down the leg across the anterior shin. An MRI of the lumbar spine was orderedand demonstrated a grade 1 anterolisthesis of L4 on L5. After a long discussion with the patie
American Medical Association. The AMA assumes no liability for the data contained herein. CPT codes and AMA CPT Assistant are copyrighted so only highlights, examples, or excerpts are presented or mentioned for educational purposes. We encourage all healthcare facilities, consulting companies, or