Transcription
Quick GuideFor CliniciansBased on TIP 36Substance Abuse Treatment forPersons With Child Abuse andNeglect Issues
ContentsWhy a Quick Guide? . 2What Is a TIP?. 3Introduction . 4Issues. 4Screening and Assessing Adults forChildhood Abuse or Neglect . 7Comprehensive Treatment .20Therapeutic Issues for Counselors .24Breaking the Intergenerational Cycle .28Legal Issues.35Selected Resources .39
Quick GuideFor CliniciansBased on TIP 36Substance Abuse Treatmentfor Persons With Child Abuseand Neglect IssuesThis Quick Guide is based entirely on information contained inTIP 36, published in 2000. No additional research has beenconducted to update this topic since publication of theoriginal TIP.
2Child Abuse and Neglect IssuesWHY A QUICK GUIDE?The purpose of a Quick Guide is to providesuccinct, easily accessible information to busyclinicians.This Quick Guide is based on Substance AbuseTreatment for Persons With Child Abuse andNeglect Issues, number 36 in the TreatmentImprovement Protocol (TIP) Series, published bythe Center for Substance Abuse Treatment (CSAT),Substance Abuse and Mental Health ServicesAdministration. It will help substance abusetreatment providers recognize and treat clientspresenting with a history of child abuse andneglect or clients who are currently maltreatingtheir children.The Quick Guide is divided into sections to helpreaders quickly locate relevant material. For morein-depth information on the topics in this QuickGuide, readers should refer to TIP 36.
What Is a TIP?WHAT IS A TIP?The TIP Series was launched in 1991. The goal ofthese publications is to disseminate consensusbased, field-tested guidelines on current topics tosubstance abuse treatment providers.TIP 36, Substance Abuse Treatment for PersonsWith Child Abuse and Neglect Issues Defines child abuse and neglect Describes screening and assessment tools foridentifying individuals with child abuse andneglect issues Presents comprehensive plans for treating adultsurvivors Discusses ways to break the intergenerationalcycle of child abuse Explains legal responsibilities and recourse.To order a copy of TIP 36 and other relatedproducts, see the inside back cover of thisQuick Guide.3
4Child Abuse and Neglect IssuesINTRODUCTIONPhysical, emotional, and sexual abuse and neglectduring childhood can increase a person’s risk ofdeveloping substance abuse disorders. Childrenof substance-abusing parents, in turn, are morelikely to be abused or neglected, resulting in anintergenerational cycle.The reported cases of abused and neglected children increased from 1.4 million in 1986 to morethan 3 million in 1997. Substance abuse wasinvolved in more than 70 percent of these cases.Substance abuse severely complicates efforts bychildren’s protective service (CPS) agencies toprotect children and rehabilitate families.ISSUESCompared with other substance users, clientswith childhood abuse histories Have more severe substance abuse disorders Started using substances at a younger age Use substances for reasons that differ fromthose of other clients Have a higher attempted suicide rate Show more posttraumatic stress disorder (PTSD)
Issues Have personality or relationship problems thatmake them hesitant to accept help Are more vulnerable to relapse.(For more information, see TIP 36, pages 1–8.)DefinitionsThe Child Abuse Prevention and Treatment Actdefines child abuse and neglect as any recent actor failure to act that results in “imminent risk ofserious harm, death, serious physical or emotionalharm, sexual abuse or exploitation” to a childbelow the age of 18, or (except in sexual abuse)below the age specified by the child protection lawof the State, by a parent or caretaker (includingany employee of a residential facility or any staffperson providing out-of-home care) who is responsible for the child’s welfare.Types of child maltreatment are Neglect—failure to provide basic physical,educational, medical, or emotional needs. Physical abuse—injury inflicted by deliberateactions. Sexual abuse—engaging a child in sexualactivities that the child cannot comprehend,consent to, or be prepared for developmentally. It includes all forms of sexual contact,5
6Child Abuse and Neglect Issuesnontouching abuse (exhibitionism, voyeurism),and commercial exploitation. Incest is theimposition of sexual acts, or acts with sexualovertones, on a child by persons who haveauthority through ongoing emotional bondingwith that child. Some States define abuse as anact perpetrated by a caregiver and assault as anact committed by a noncaregiver. However, it iscommonly held that any use of force constitutessexual assault. Emotional or psychological abuse—an act ofcommission or omission that causes seriousbehavioral, cognitive, emotional, or mentaldisorders; it is the most difficult form of abuseto identify.The counselor should consider the meaning of thetrauma or abuse to the client, the effect on theclient, and not just legal definitions.Childhood trauma can Increase the intensity of treatment servicesrequired Lengthen the time needed for treatment Increase the number of sessions needed.(For more information, see TIP 36, pages 9–14.)
Screening and AssessingSCREENING AND ASSESSING ADULTSFOR CHILDHOOD ABUSE OR NEGLECTChildhood abuse and neglect often alter a child’sperception of the world, leading to feelings ofbetrayal, an inability to trust, low self-esteem,and great shame.The following reactions, symptoms, or disordersmay result: Self-mutilation Depression (thoughts of death, suicidalideation, feeling hopeless) Dissociative responses Aggressive behavior or “acting out,” includingwEarly sexual activity or sexualized behaviorwPhysically abusing or harming animals Poor relationships with one or both parents Attachment disorder, difficulty trusting others Excessive passivity Passive/aggressive behavior Blacked-out timeframes—no memory of periodsduring childhood Excessive nightmares, extreme fear of the dark,or requests for locks on doors7
8Child Abuse and Neglect Issues Posttraumatic stress disorder Eating disorders Borderline personality disorders Excessive anger or shame Anxiety High tolerance for inappropriate behavior Arousal, hyperreactivity Age regression Derealization/depersonalization Emotional and sensory numbing.Screening and assessment should be done In a safe, nonthreatening environment Early in the comprehensive assessment process At different times during treatment.Several factors make accurate screening achallenge: Underreporting or overreporting of traumahistories or symptoms Repressed memories Coexisting psychiatric disorders.
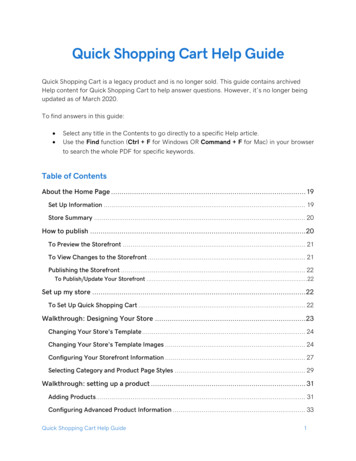
Screening and AssessingOngoing screening elicits more information abouttraumatic experiences—especially after trust hasbeen established in the therapeutic relationship.No one should screen for childhood traumawithout proper training and supervision.Counselors should learn to Understand the effects of childhood maltreatment on the adult’s feelings and behaviors Identify individuals with symptoms of abuse orneglect.Clinicians are more likely to ask female clientsabout past childhood maltreatment, but manymale clients also were neglected and abused(including sexually) as children.Screening MethodsExhibit 36–1 lists information about a sample ofscreening instruments. Screening can be done byasking direct questions (see exhibit 36–2) or byusing standardized instruments.(For more information, see TIP 36, pages 15–25and pages 169–172.)9
0/ctq.htmlhttp://home.earthlink.net/ rohner research28-item self-reportquestionnairebrief self-report questionnaire concerning parentalaffection, hostility, neglect,and rejectionChildhood TraumaQuestionnaire (CTQ)Parental Acceptance andRejection Questionnaire(PARQ)Contact161-item structured, clinicalquestionnaire, frequentlyused during intakeDescriptionAddiction Severity Index(ASI)InstrumentsExhibit 36–1Standardized Screening Instruments10 Child Abuse and Neglect Issues
http://portal.wpspublish.com/portal/page?pageid 53,53086&dad portal&schema PORTALEve Carlson, PhDNational Center for PTSD(334-PTSD)795 Willow RoadMenlo Park, CA 94025Email: m78-item self-report questionnaire assessing parenting,parental satisfaction, communication, limit setting, andautonomy17-item self-report tool, useful for clients with multipletraumas or an unknowntrauma history40-item self-report tool with6 subscales that evaluateanxiety, dissociation, andsexual concernsParent-Child RelationshipInventory (PCRI)Screen for PosttraumaticStress Symptoms (SPTSS)Trauma SymptomChecklist-40 (TSC-40)Screening and Assessing 11
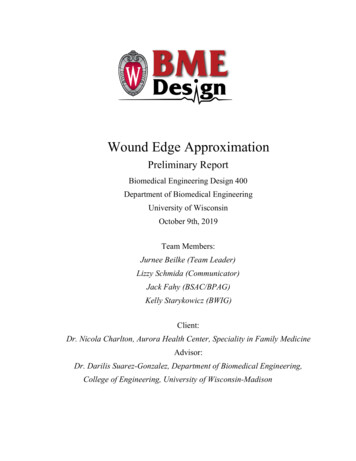
12 Child Abuse and Neglect IssuesExhibit 36–2Direct Questions To Use inChildhood Abuse or Neglect ScreeningQuestions about traumatic eventsWhen you were a child Were there any significant traumatic events inyour family while you were growing up? Forexample: deaths, hospitalizations, or incarcerations of a parent or sibling; divorces; orchronic diseases? Were you treated harshly? Did you ever experience physical, sexual, oremotional abuse? Did you experience inappropriate physical orsexual contact with an adult or person at least5 years older than you? Was there violence in your household, such asbattering of siblings, a parent, or his or herpartner? Do you feel that your parents neglected you?Did you have adequate food, clothing, shelter,or protection? Did your parents frequently use alcohol ordrugs? Did you ever use alcohol or drugs withthem?
Screening and Assessing 13Exhibit 36–2 (continued)Questions about circumstances suggestive oftraumatic events Have you or has anyone in your family ever beeninvolved with children’s protective services? Did you ever live away from your parents?Were you or your siblings ever in foster care? Did you ever feel unsafe or in danger? Have you ever felt that abuse or neglect wasyour fault and that you deserved it?Adapted from TIP 36, Substance Abuse Treatment for PersonsWith Child Abuse and Neglect Issues, page 24.AssessmentA positive screen indicates that more informationand a thorough assessment are needed. Alsoconsider The client’s readiness to discuss the issue The input of members of the treatment team The family’s involvement.Family-of-origin characteristics to consider duringan assessment include A history of parental substance abuse and/orviolence
14 Child Abuse and Neglect Issues CPS involvement The placement of children in foster care The use of severe discipline during childhood Traumatic family separations and losses.(For more information, see TIP 36, pages xvii–xx.)Ask for information about The type of abusewPhysical, sexual, or psychological abusewNeglectwExploitationwMultiple forms of abuse Whether the perpetrator was a parent, otherrelative, stranger, teacher, or caregiver The frequency and duration of abuse (i.e., agesat onset and cessation) The context of the trauma, including the use offorce or fear The family’s knowledge of and response to theabuse
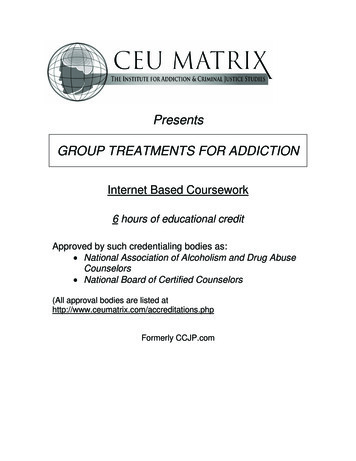
Screening and Assessing 15 Any mental health counseling or othertreatment as a child How and when the abuse was disclosed Its social and legal consequences.(For more information, see TIP 36, pages 25–39.)Special ConsiderationsTreatment programs should have written protocolsthat describe The who, when, and where of screening andassessments The information required Confidentiality and reporting regulations Each treatment team member’s role Screening instruments to use How to present, discuss, document, andinterpret findings How to incorporate findings into treatmentplans.Standardized tests should be used as guidelinesto conduct screening and assessments. Exhibit36–3 presents a sample of assessment tools.(For more information, see TIP 36, pages 39–41.)
Description21-item scale; measures depression severity53-item tool/10 minutes65-point objective rating scale; measures mood states90-item brief multidimensional inventory; screens forpsychopathology/15 minutes120-question structured interview; screens for majorpsychiatric disordersdiagnostic interview; based on Diagnostic and StatisticalManual of Mental Disorders, Fourth Edition (DSM–IV)/90to 150 minutesNameBeck Depression Inventory(BDI)Brief Symptom Inventory (BSI)Profile of Mood States (POMS)Symptom Checklist-90-Revised(SCL-90-R)Mini International Neuropsychiatric Interview (MINI)Psychiatric Research Interviewfor Substance and MentalHealth Disorders (PRISM)A. Mental Health AssessmentsExhibit 36–3Assessment Tools16 Child Abuse and Neglect Issues
comprehensive interview tool; reviews all DSM-IV Axis IdisordersStructured Clinical Interviewfor DSM-IV Axis I Disorders(SCID-I)focuses on psychological abuse and neglect; assessesphysical and sexual abuse17-item tool/10 to 15 minutesAssessing Environments III,Form SDChildhood MaltreatmentQuestionnaire (CMQ)Trauma Assessment for Adults(TAA)-Self-Report(continued on next page)Description170 items, 7 scales; determines clients’ perceptions ofmaltreatmentNameB. Trauma-Oriented Toolsused for evaluation, diagnosis, determining prognosis andseveritySchedule for AffectiveDisorders and Schizophrenia(SADS)Screening and Assessing 17
Descriptionevaluates 30 specific traumas28-item tool; elicits information on pathological and normative dissociative experiences/5 to 10 minutes17-item tool/10 to 15 minutes26-item tool/5 to 15 minutes49-item tool; assesses all DSM-IV criteria for PTSD/10 to15 minutes100-item test; evaluates consequences, identifiesproblems needing immediate attention (suicidal ideation/behavior, psychosis, self-mutilation)/20 minutesNameTraumatic Events Scale (TES)Dissociative ExperiencesScale (DES)Modified PTSD SymptomScale: Self-Report Version(MPSS-SR)Penn Inventory forPosttraumatic Stress DisorderPosttraumatic StressDiagnostic Scale (PDS)Trauma Symptom Inventory(TSI)Exhibit 36–3 (continued)18 Child Abuse and Neglect Issues
46-items; assesses emotional, physical, and sexual abuse49 items plus multiple followup probes/30 to 90 minutes13-item tool; evaluates potentially traumatic events56-item self-report questionnaire semistructuredinterview7 screening items with probes for positive answers/15 to30 minutes30-item structured interview/30 to 60 minutes toadministerChild Maltreatment InterviewSchedule (CMIS)Childhood Trauma Interview(CTI)Trauma Assessment forAdults (TAA)Evaluation of LifetimeStressors (ELS)National Women’s StudyEvent History (NWSEH)Clinician-AdministeredPosttraumatic Stress DisorderScale (CAPS)Screening and Assessing 19
20 Child Abuse and Neglect IssuesCOMPREHENSIVE TREATMENTAcknowledging past child abuse helps clientsbreak through secrecy and shame resulting fromabuse. Talking to a sympathetic listener can be animportant first step in the healing process.Counselors should Show their unconditional regard, nonjudgmentalattitude, and sincerity Be sensitive to the client’s cultural background Be a sympathetic listener Acknowledge and validate the client’s experience by recognizing the issue and refocusingthe treatment to address the issue Provide a link to mental health services, if theclient needs additional treatment Adhere closely to accepted standards of practice, ethics, and legal requirements Delicately discuss past abuse in the presenceof family members who were involved Disclose abuse with tact and sensitivity Explain the treatment itself and when and howabuse issues will be addressed.
Comprehensive Treatment 21Clients’ subjective experience of and feelingsabout the abuse can shape their psychologicalresponse more than the actual circumstances ofit. It is normal for clients to be uncertain about theabuse or not remember all that happened. Thecounselor should Support the client’s recall Reinforce that the feelings about thetrauma are the most significant aspect ofthe experience Consider the client’s coping strategies and theireffectiveness.Substance abusers generally go throughthree stages when dealing with their childhoodmaltreatment issues, which may take years tocomplete. They are Stage 1 (0–30 days)—Substance abuse treatment begins. In-depth attention to childhoodtrauma issues is not appropriate. Stage 2 (31 days–2 yrs.)—The client may beable to address childhood issues. Stage 3 (2 yrs.)—The client is able to deal witha broad range of issues.Never force clients to confront abuse issues. Thismay create an abusive situation and retraumatize
22 Child Abuse and Neglect Issuesthe client. Whether to address childhood abuse isthe client’s choice and depends on the client’ssymptoms and ability to stay sober.Some individuals with childhood abuse issuesmay not do well in group settings, so grouptherapy may not be appropriate. Gender-specificgroups are generally more beneficial.For most clients, therapeutic work in addition tosubstance abuse treatment is required for fullresolution of the issue.Tell clients Their history of child maltreatment may havecontributed to some of their errors in thinkingand decisionmaking. They may have medicated themselves with substances to avoid dealing with their feelings. They are not alone, and resources are availableto help. They can learn better ways to cope and live ahappier life.(For more information, see TIP 36, pages 43–50.)
Comprehensive Treatment 23Involving the Family in TreatmentIf a client and the treatment team agree toinclude family therapy in substance abuse treatment, it should be conducted by a licensedmental health professional with specific trainingin childhood abuse and neglect. Whether familytherapy is appropriate depends on The family’s knowledge and acknowledgment ofthe abuse The client’s feelings and preferences The current relationships among familymembers.Counselors should be cautious about discussingchild abuse issues with family members. This maynot be therapeutic or essential for every client.Mental Health Treatment ServicesCounselors should consider their limitations whenworking with clients who were severely abused.Although it is best to treat substance abuse andother mental health issues in the same venue,this is not always possible. When a client’s mentalhealth problems are beyond the counselor’streatment ability, a referral must be made to anappropriate provider.
24 Child Abuse and Neglect IssuesClients should be immediately evaluated bya psychiatrist if they have or show Active, severe depression or anxiety Self-mutilation tendencies Suicidal ideation or behavior Extreme dissociative actions A history of other psychiatric crises.(For more information, see TIP 36, pages 50–58.)THERAPEUTIC ISSUES FORCOUNSELORSMany clients raised in abusive householdslearned how to function in an unhealthy environment and did not learn healthy interpersonalbehavior skills. Counselors should model thesebehaviors and Expect their clients to do well Be warm and respectful Be sensitive to cultural concerns Recognize potential language differences Not excuse parents’ abusive or neglectfulbehavior because of cultural differences.
Therapeutic Issues for Counselors 25The violence and cruelty clients experiencedupsets many counselors and results in intensereactions. Counselors should be aware of The effect a client’s story has on them Their own countertransference reactions Any judgmental or insensitive attitude The need to seek supervision.The counselor must be aware of the following: Transference—feelings and issues that clientsproject onto a counselor during therapy. Countertransference—a counselor’sreactions and responses to a client’s issues.The counselor loses objectivity and becomesoverwhelmed, angry, or bereft about a client’sexperience. Secondary Traumatization—symptoms oftrauma that are brought about by repeatedconfrontations or disclosures of victimizationand exploitation. Burnout—when work pressure erodes a counselor’s well-being and interferes with his or herpersonal life.
26 Child Abuse and Neglect IssuesCounselors should Not work in isolation Seek to treat individuals with a variety ofproblems Keep a manageable caseload Receive support from their agency Recognize when they are unable to work with aspecific client and refer that client to anotherprovider.An agency can support counselors by Providing a sense of mission Providing ongoing clinical supervision Supporting their efforts to keep their caseloadsmanageable.The Treatment FrameDevelop a treatment frame—the set of conditionsnecessary to support a professional relationshipwith the client. Its parameters might include Specifying regular appointment times inadvance Enforcing set starting and ending times for eachsession
Therapeutic Issues for Counselors 27 Declining to give out a home phone number oraddress to clients Canceling sessions if a client arrives under theinfluence of alcohol or psychoactive drugs Not having client contact outside the therapysession Not having sexual contact or interactions with aclient that could reasonably be interpreted assexual Terminating counseling if violence is threatened Establishing and enforcing a clear policyregarding payment.Building TrustBecause adults who were abused or neglected bytheir parents have experienced betrayal in theirmost significant relationships, they often cannottrust others. The counselor should Remain consistent and available Help allay clients’ fears of abandonment andrejection Show unconditional positive regard Maintain a nonjudgmental attitude.(For more information, see TIP 36, pages 61–71.)
28 Child Abuse and Neglect IssuesBREAKING THE INTERGENERATIONALCYCLEChildren whose parents abuse substances aremore likely to be abused or neglected than otherchildren, to grow up and abuse substances themselves, and to abuse their own children.Adults who were victims of childhood maltreatment often have difficulty parenting because oftheir inability to Trust Choose emotionally healthy partners Manage stress Nurture themselves or others.Family-centered interventions are the mostsuccessful at breaking the cycle of substanceabuse, child neglect, and child maltreatment.Just as substance-abusing parents often denytheir drug use, they may deny neglecting or abusing their children.(For more information, see TIP 36, pages xxii andxxiii.)
Breaking the Intergenerational Cycle 29Who Abuses and WhyCharacteristics shared by parents who abuse theirchildren include Considering child rearing difficult andunenjoyable Using excessively controlling disciplinarytechniques Not encouraging autonomy in their childrenwhile maintaining high standards ofachievement Promoting an isolated lifestyle for themselvesand their children Expecting their children to take on the role ofcaretaker.Other characteristics of abusive parents include Poverty, substance dependence, mental illness Feelings of inadequacy and self-reproach, oftenrelated to early negative experiences Depression, difficulty articulating their needs orfeelings, anxiety Seriously arrested development A sense of incompleteness resulting from afailure to internalize a separate identity (manifested by clinging to their children)
30 Child Abuse and Neglect Issues Having other abusive and unfullfillingrelationships An inability to tolerate being alone Fear of taking responsibility and makingdecisions Severe difficulty with verbal communication Difficulty in seeking or obtaining pleasure Extreme narcissism, gross immaturity, anddependence An impaired ability to empathize with a child’sneeds.Some children avoid becoming part of the cycle ofabuse. These children tend to exhibit “resilience”factors such as Insight—sensing that life in the troubled familyis not “normal” Independence—separating from the troubledfamily Other relationships—fulfilling needs not met bythe troubled family through others Initiative—attempting to overcome negativefeelings Creativity—transforming pain into somethingworthwhile
Breaking the Intergenerational Cycle 31 Humor—making tragedies into something funny Morality—understanding common mores ofgood and bad as they exist both inside and outside the family.(For more information, see TIP 36, pages 73–76.)Role of the CounselorBy working closely with a substance abuser, thecounselor can break the abuse cycle. The treatment provider should become familiar with theclient’s family life and any parenting behaviorsthat might indicate possible child abuse.Parents who abuse substances differ in experiences and parenting skills. Questions to askclients to gain insight into their home life include What groups give you support? Do you have anyspecial friends? Do you belong to a communityor faith-based organization? What type of social activities do you enjoy? Howoften do you participate in them? Have you been involved in the criminal justicesystem? When? Have you ever been onprobation? Have you been involved with other socialservice agencies? With CPS agencies? Why?
32 Child Abuse and Neglect Issues Who else lives in your home? Who else spendstime there? What is your routine each day? On weekends? What do you do with your children each day? Onholidays? Are your children receiving ongoing medicalcare? What is their health status? Does anyone care for your children besidesyou? What is his or her role and attitude towardthe children?If the counselor can observe how a client relatesto his or her children, the counselor shouldconsider these questions: How does the client react to the children’sbehavior? How does the parent respond to their emotionalneeds? Do the children make eye contact with him orher? How does he or she respond to the children’scrying? How does the parent praise and discipline thechildren? Are the parent’s expectations age appropriate?
Breaking the Intergenerational Cycle 33In addition to the above questions, counselorstreating clients who do not have custody of theirchildren should learn about The CPS agency’s plan, requirements, andschedule for family reunification The client’s history of custody challenges andoutcomes.(For more information, see TIP 36, pages 79–93.)Behavioral clues that suggest possible child abuseor neglect include Name calling, belittling, or negative labeling ofchildren Telling stories that suggest children are living inunsafe conditions (e.g., being left alone) Blaming children or directing misplaced angerat them that may mask guilt or poor parenting Having inappropriate expectations for thechildren’s age/developmental stage Giving children too many responsibilities andtoo much autonomy for their age Sexualizing a child/children Making negative comparisons involving thechildren
34 Child Abuse and Neglect Issues Imposing inappropriate discipline or not beingable to distinguish between discipline (guiding)and punishment (hurting).(For more information, see TIP 36, pages 73–80.)Treatment Strategies for Child AbusersWhen parents lack good parenting skills, they willneed help Recognizing the importance of appropriate parenting behaviors Seeking assistance in becoming better parents Identifying others who can support them Understanding how substance abuse affectsresponsible parenting.Remember to reinforce clients’ positive skills andpraise them when they demonstrate appropriateparenting behavior.Parents need help learning about Child development Good parenting skills The impact of child abuse on a person How to form good relationships with a partnerand other adults
Legal Issues 35 Healthy personal and social development skills.Counselors should make clear that They are concerned about the client both as aperson with a substance abuse disorder and asa parent with responsibilities. The client’s safety and the children’s safety areboth important.LEGAL ISSUESRecordkeepingInstances of abuse and neglect revealed by aclient must be recorded. To protect the provider,the record should state that the client reportedabuse, not that the client “was abused.”Counselors should Record information in an organized, professional manner Document only the factual, observable behaviorof a client and his or her statements Omit judgmental statements Respect the rules of confidentiality (42 Code ofFederal Regulations [C.F.R.] Part 2).
36 Child Abuse and Neglect IssuesAccording to Federal regulations, information maybe provided to outside sources only if there iswritten consent from the client, a court order, or aqualified service organization agreement.(For more information, see TIP 36, page 59 andappendix B.)Mandated ReportingAll States require counselors to report incidents ofknown or suspected child abuse or neglect suchas when A child has been injured by a parent or otheradult (other than accidentally). A parent or other adult does not seek medicalattention or fails to follow medical advice for aseriously ill or injured child. An adult has inappropriately touched a child (ormade the child touch an adult inappropriately),sexually abused a child, or exploited a child. A child is not attending school, and the parentrefuses to send him or her (home schoolingmust be documented).Consult a supervisor before reporting suspectedchild abuse or neglect, unless immediate action isrequired (the child is in immediate danger).
Legal Issues 37Agencies should provide orientation aboutreporting policies and procedures to all staff.An adult survivor of abuse usually discussesevents that took place many years before, whichgenerally are exempt from reporting requirements.However, if the person who abused or neglectedthe client has
Child Abuse and Neglect Issues 4 INTRODUCTION Physical, emotional, and sexual abuse and neglect during childhood can increase a person’s risk of developing substance abuse disorders. Children of substance-abusing parents, in turn, are more likely to be abus