Transcription
Hoarseness CaseA Self-Directed Learning ModuleDepartment of Otolaryngology – Head & Neck SurgerySchulich School of Medicine & Dentistry, Western UniversityClick to Begin
Case PresentationA 55-year-old male mechanic presents toyour clinic with a four week history ofhoarseness.You are the otolaryngologist, click through the module to diagnose and treat this patient.Obtain a history
Patient HistoryBack to Case PresentationWhat brings you in today?My voice has gotten progressively hoarse over the past month. The hoarseness is constant, and nothing makes itbetter or worse. I haven’t tried any medications or therapies. This has never happened to me before. I have alwayshad a bit of a cough, but it has gotten worse over the past month. Recently, there has been some blood on thetissue.Past medical history?My overall health is ok besides some heartburn. I don’t take any medications or have any allergies. I have not hadany radiation exposure, head and neck surgeries, or recent injuries or trauma.Social history?I work full time as a mechanic, and live alone in an apartment downtown. I am divorced, and have a son who livesin California. I have smoked about a pack of cigarettes each day since I was 18 years old. I have 1-2 beers/night onweekdays, and 8-10/night on weekends. I don’t do any recreational drugs. I rarely exercise and eat a lot of takeoutfood.What is on your differential diagnosis so far?
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.Neurologic?SystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.(K) Congenital?Why not?A congenital problem, such ascongenital web, would have likelypresented much earlier in life.NeurologicSystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaInfectious & IdiopathicInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.Why?No infectious symptoms, but need toconsider idiopathic causes.?DDx-Laryngitis-Vocal fold immobility-Muscle-tension disordersNeurologicSystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaToxins & TraumaInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.Why?No history of trauma or toxin exposure, but canconsider diagnoses related to poor voicehygiene.DDx-Laryngeal cysts, nodules, or polyps-Voice abuse-Reinke’s edemaNeurologicSystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaTumourInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.Why?Gradual onset, smoking history.DDx-Recurrent respiratory papillomatosis-Laryngeal cancer-Benign laryngeal massesNeurologicSystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaInfectious & Idiopathic(K) CongenitalEndocrineWhy not?No associated , R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.With your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaNeurologicInfectious & Idiopathic(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.Why not?No associated symptoms.DDx-Spasmodic dysphonia-Tremor-Multiple sclerosis, Myasthenia Gravis,Parkinson’s-StrokeNeurologicSystemicWith your DDx in mind, proceed to focused physical exam.
What diagnoses are coming to mind?Back to Case PresentationThink KITTENS! (Click on heading to test yourself)TumourEndocrineToxins & TraumaInfectious & IdiopathicSystemicNeurologicWhy?Patient stated history of GERD.(K) CongenitalPasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery ClinicalReference Guide. Fourth Edition. San Diego, California: Plural Publishing.DDx-GERD-Connective tissue disordersSystemicWith your DDx in mind, proceed to focused physical exam.
Back to Case PresentationPhysical Exam(Click on the physical examinations.)General inspection & vitalsCranial nerve examsHead & neck examProceed to investigations
Back to Case PresentationPhysical ExamGeneral inspection & vitals(Click on the physical examinations.)Patient looks comfortable with a hoarse andstrained voice. There is no stridor.Vitals:Cranial nerve examsHR: 90 bpmRR: 16 breaths/minuteBP: 150/90 mmHgTemperature: 37 Head & neck examProceed to investigations
Back to Case PresentationPhysical Exam(Click on the physical examinations.)General inspection & vitalsCranial nerve exams:CN II – XII: IntactCranial nerve examsHead & neck examProceed to investigations
Back to Case PresentationFocused Head & Neck ExamGeneral:Inspection No distress No scars, asymmetry, masses,enlarged thyroid, or skin lesionsAnterior rhinoscopy exam: NormalOral Cavity Exam:Nasolaryngoscope:Otoscopy: NormalPalpation No palpable lymph nodes Salivary glands palpable Thyroid not palpablevoicedoctor.net Vocal cords are mobileReview: Cervical lymph nodesReview: Laryngeal anatomyBack to Physical Exam
Back to Case PresentationReview: Cervical lymph nodesDistinguishing palpable LNs: Infected LNs Firm, tender, enlarged and warm.Overlying skin can appear reddened. Malignant LNs Firm, non-tender, matted, fixed, andincrease in size over time.Back
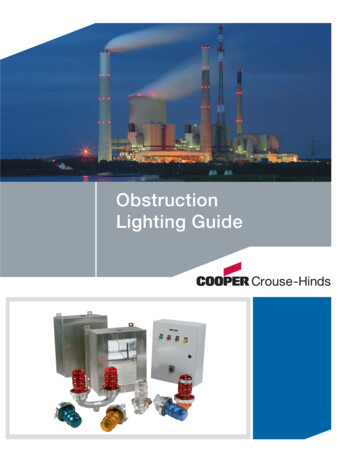
Review: Laryngeal anatomySuperior Views of LarynxEpiglottisAnteriorBack to Case PresentationThyroid cartilageBase of tongueTruevocal foldFalsevocal geal inletBack
Back to Case PresentationInvestigations (Click on the buttons to see investigation results.)CT NeckU/S of neckBiopsyContinue to Diagnosis
Back to Case PresentationInvestigations (Click on the buttons to see investigation results.)CT NeckU/S of neckBiopsyContinue to Diagnosis
Back to Case PresentationInvestigations (Click on the buttons to see investigation results.)CT NeckU/S of neckAn U/S of the neck is notnecessary as it will not addinformation to the diagnosis.BiopsyContinue to Diagnosis
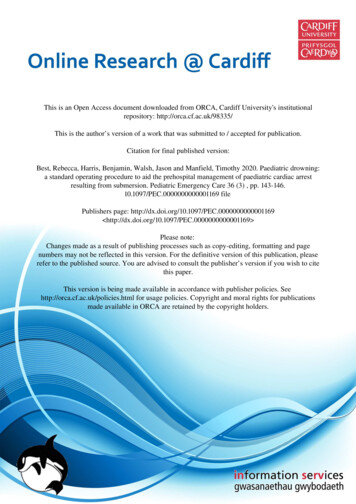
Back to Case PresentationInvestigations (Click on the buttons to see investigation results.)Biopsy of vocal cord lesion: squamous cell carcinomaCT NeckU/S of 807541/PMC2807541 12105 2008 93 Fig1 HTML.pngContinue to Diagnosis
Back to Case PresentationSummary of findingsChief Complaints: 55 year old man with 4 week history of progressivehoarseness and intermittent hemoptysis 37 pack year smoking historyPhysical Exam: Vitals: hypertensive Cranial nerve exams: normal Head and neck exam: no enlarged cervical lymph nodes Nasolaryngoscope: lesion on R vocal cord. Vocal cordsmobile.Based on your findings,choose the most likely diagnosis:a. Hypopharyngeal cancerb. Laryngeal cancerc. Recurrent respiratory papillomatosisd. Vocal fold polypvoicedoctor.netInvestigations: Head & neck CT scan: lesion on R vocal cord, noenlarged cervical lymph nodes Biopsy: positive for squamous cell carcinoma
Back to Case PresentationDiagnosisIncorrect. Anatomically, the hypopharynx isdefined as the area from the level of the hyoidbone to cricopharyngeus (upper esophagealsphincter). In this patient, the lesion waslocated on the vocal fold, classifying it as alaryngeal cancer.Most hypoharyngeal cancers are squamous cellin origin.Risk factors include: smoking,alcohol, GERD, and Barrett’s esophagus.Hypopharyngeal cancers can be classifiedbased on location: piriform sinus (mostcommon), posterior pharyngeal wall, and thepost-cricoid region.Please choose again.Back to diagnosis
Back to Case PresentationDiagnosisCorrect! This is a case of laryngeal cancer, specifically of the glottis. Major risk factors forlaryngeal cancer include smoking and alcohol.Signs and symptoms include: hoarseness, dysphagia, odynophagia, sore throat, hemoptysis,stridor, referred otalgia, weight loss, and globus sensation.Since laryngeal cancer treatment is based on staging, click on “staging” below to review thestaging for glottic cancer before you decide on a treatment.Staging
Back to Case PresentationGlottic Cancer StagingTCategoryT CriteriaNCategoryT1Tumour limited to the vocal cord(s) with normal mobility.T1a: Limited to 1 vocal cord.T1b: Limited to 2 vocal cords.N0T2Tumour extends to supraglottis and/or subglottis withimpaired vocal cord mobility.Clinical N CriteriaENE – extranodal extensionMCategoryM CriteriaNo regional LN metastasis.M0No distantmetastasesN1Single ipsilateral LN 3 cm and ENE (-).M1DistantmetastasesT3Tumour limited to larynx with vocal cord fixation and/orinvasion of paraglottic space and/or inner cortex of thethyroid cartilage.N2N2a: Single ipsilateral LN 3 cm but 6 cm & ENE (-).N2b: Multiple ipsilateral LNs 6 cm & ENE (-).N2c: Bilateral or contralateral LNs 6 cm & ENE (-).T4T4a: Moderately advanced local disease. Tumour invadesthrough the outer cortex of the thyroid cartilage and/orinvades tissue beyond the larynx.T4b: Very advanced local disease. Tumour invadesprevertebral space, encases carotid artery, or invadesmediastinal structures.N3N3a: Any LN 6 cm & ENE (-)N3b: Any LN with clinically overt ENE ( )Patient in this case: T1aN0M? T1a: One vocal fold involved (Based on nasopharyngoscopy and CT). N0: Neck is free of lymph nodes (Based on palpation of cervical lymph nodes and confirmed by CT scan). M?: Would need CT head, neck, and chest to determine if metastases are present in the lungs.Treatments
Back to Case PresentationDiagnosisIncorrect. The appearance of the lesion on the vocal cord and biopsy findings point to a differentdiagnosis.Recurrent respiratory papillomatosis (RRP) is caused by the human papilloma virus (HPV), mostcommonly HPV 6 & 11. RRP presents with progressive hoarseness, stridor, or dyspnea. RRP can bediagnosed via nasolaryngoscopy. The lesions tend to recur, therefore treatment includes repeatedendoscopic excisions. HPV vaccination is important for prevention of RRP.www.massgeneral.orgPlease choose again.www.chicagovoicecare.comBack to diagnosis
Back to Case PresentationDiagnosisIncorrect. The appearance of the lesion on the vocal cord and biopsy findings point to adifferent diagnosis.Vocal fold polyps develop due to chronic vocal fold irritation. Risk factors include:smoking, GERD, and muscle tension dysphonia. Polyps tend to be unilateral and areusually treated conservatively. Surgical excision is considered if the polyp is symptomaticand conservative treatment failed.Please choose again.http://voicehealth101.comBack to diagnosis
Back to Case PresentationThere are three main treatment categories for laryngeal cancer.Please select the two most appropriate for this particular case.ChemotherapyRadiationSurgery
Back to Case PresentationThere are three main treatment categories for laryngeal cancer.Please select the two most appropriate for this particular case.ChemotherapyRadiationIncorrect. Chemotherapy is only indicated foradvanced stage laryngeal cancer. Since the patientin this case is presenting early in the disease,chemotherapy is not indicated.Please choose another treatment.Surgery
Back to Case PresentationThere are three main treatment categories for laryngeal cancer.Please select the two most appropriate for this particular case.ChemotherapyCorrect!RadiationEarly glottic carcinoma is treated with eitherradiation therapy or surgery. This decision iscenter specific and requires a multidisciplinarydiscussion.SurgeryContinue to Quiz
Back to Case PresentationThere are three main treatment categories for laryngeal cancer.Please select the two most appropriate for this particular case.ChemotherapyCorrect!RadiationEarly glottic carcinoma is treated with eitherradiation therapy or surgery (such as acordectomy). This decision is center specific andrequires a multidisciplinary discussion.SurgeryContinue to Quiz
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. Alcoholc. HPVd. a & ce. All of the above
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. AlcoholIncorrect. While tobacco is a major risk factor for headand neck cancers, it is not the only one.c. HPVPlease try again.d. a & ce. All of the above
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. AlcoholIncorrect. While alcohol is a major risk factor for headand neck cancers, it is not the only one.c. HPVPlease try again.d. a & ce. All of the above
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. AlcoholIncorrect. While HPV infection is a major risk factor forhead and neck cancers, it is not the only one.c. HPVPlease try again.d. a & ce. All of the above
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. Alcoholc. HPVd. a & ce. All of the aboveIncorrect. While tobacco and HPV infection are majorrisk factors for head and neck cancers, they are not theonly ones.Please try again.
Back to Case PresentationQuiz – Q1What is/are the most important risk factor(s) for head and neck cancers?a. Tobaccob. Alcoholc. HPVCorrect! Tobacco, alcohol, and HPV infection are themajor risk factors for head and neck cancers.d. a & ce. All of the aboveProceed to Q2
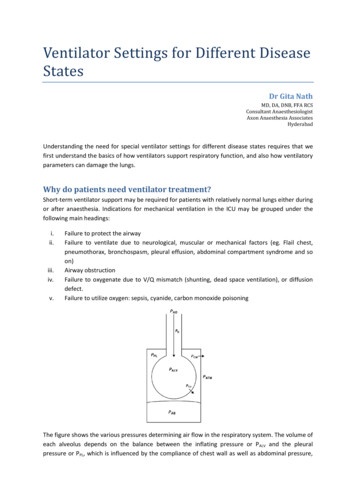
Back to Case PresentationQuiz – Q2Identify the structure indicated by the arrow.a. Cricoid cartilageAnteriorb. Piriform sinusc. Epiglottisd. Arytenoid cartilagePosterior
Back to Case PresentationQuiz – Q2Identify the structure indicated by the arrow.a. Cricoid cartilageAnteriorb. Piriform sinusc. Epiglottisd. Arytenoid cartilageIncorrect. Please try again.Posterior
Back to Case PresentationQuiz – Q2Identify the structure indicated by the arrow.a. Cricoid cartilageAnteriorb. Piriform sinusc. Epiglottisd. Arytenoid cartilageIncorrect. Please try again.PosteriorPiriformsinus
Back to Case PresentationQuiz – Q2Identify the structure indicated by the arrow.a. Cricoid cartilageAnteriorb. Piriform sinusc. Epiglottisd. Arytenoid cartilageIncorrect. Please try again.PosteriorEpiglottis
Back to Case PresentationQuiz – Q2Identify the structure indicated by the arrow.a. Cricoid cartilageAnteriorb. Piriform sinusc. Epiglottisd. Arytenoid cartilageCorrect!PosteriorProceed to Q3
Back to Case PresentationQuiz – Q3What is the first-line treatment for early glottic cancer?a. Chemotherapyb. Radiationc. Surgeryd. b & c
Back to Case PresentationQuiz – Q3What is the first-line treatment for early glottic cancer?a. Chemotherapyb. Radiationc. Surgeryd. b & cIncorrect. Chemotherapy is indicated in advancedlaryngeal cancer, where multimodal therapy can includesurgery, radiation, and chemotherapy.Please choose again.
Back to Case PresentationQuiz – Q3What is the first-line treatment for early glottic cancer?a. Chemotherapyb. Radiationc. Surgeryd. b & cIncorrect. While radiation is a first-line treatment forearly glottic cancer, it is not the only one.Please choose again.
Back to Case PresentationQuiz – Q3What is the first-line treatment for early glottic cancer?a. Chemotherapyb. Radiationc. Surgeryd. b & cIncorrect. While surgery is a first-line treatment for earlyglottic cancer, it is not the only one.Please choose again.
Back to Case PresentationQuiz – Q3What is the first-line treatment for early glottic cancer?a. Chemotherapyb. RadiationCorrect! Both surgery and radiation are first-linetreatments for early glottic cancer. This decision is basedon many factors and requires a multidisciplinarydiscussion.c. Surgeryd. b & cContinue
Back to Case PresentationCongratulations! You have finished the hoarseness module.Key points to remember: The larynx is the 2nd most common site for head and neck malignancy 90% are squamous cell carcinomas Signs and symptoms of laryngeal cancer: Hoarseness, dysphagia, odynophagia, sore throat, hemoptysis, stridor, referred otalgia, weight loss, globus sensation Risk factors for head and neck cancers: Smoking Alcohol HPV Radiation exposure Treatments for laryngeal cancer include radiation, chemotherapy, and surgery. Treatment choice depends on staging Primary treatment of early stages surgery or radiation therapyContinueor return to theReview sections.
Module Review SectionsBack to Case PresentationAnatomy:Review: Cervical lymph nodesReview: Laryngeal anatomyBack to summary
Back to Case PresentationReview: Cervical lymph nodesDistinguishing palpable LNs: Infected LNs Firm, tender, enlarged and warm.Overlying skin can appear reddened. Malignant LNs Firm, non-tender, matted, fixed, andincrease in size over time.Back
Review: Laryngeal anatomySuperior Views of LarynxEpiglottisAnteriorBack to Case PresentationThyroid cartilageBase of tongueTruevocal foldFalsevocal geal inletBack
Back to Case PresentationModule Authors Kylen Van Osch, Meds 2020 & Peng You MD Module adapted from: Jason Beyea MD PhD FRCSCYou may now exit, return to Review sections or retake theQuiz
Pasha, R., Golub, J. (2014) Otolaryngology Head and Neck Surgery Clinical Reference Guide. Fourth Edition. San Diego, California: Plural Publishing. Back to Case Presentation Physical Exam (Click on the physical exami