Transcription
Asthma, GERD and LaryngealPharyngeal Reflux (LPR)Richard F. Lockey, M.D.Division of Allergy and ImmunologyDepartment of Internal MedicineUniversity of South FloridaCollege of MedicineandJames A. Haley Veterans’ Medical CenterTampa, Florida
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Definitions GER: backflow of stomach contents into theesophagus, usually acidic GERD: abnormal GER– DeMeester score with pH probe– Dobhan criteria for proximal GERD– May result in inflammation of esophagus LPR: laryngopharyngeal reflux
Definition of GERD –Genval Workshop “The term GERD should be used to include allindividuals who are exposed to the risk ofphysical complications from gastroesophagealreflux, or who experience clinically significantimpairment of health-related well-being (qualityof life) due to reflux-related symptoms, afteradequate reassurance of the benign nature oftheir symptoms”Dent et al. Gut 1998
Heartburn Heartburn is the most common manifestation ofGERD The word ‘heartburn’ is often misinterpreted bypatients1 Description of heartburn as “a burning feeling risingfrom the stomach or lower chest up towards theneck” can help patients to recognize this symptom1 When heartburn is the main or only symptomexperienced by a patient, it is strongly suggestive ofthe presence of GERD21Carlssonet al. Scand J Gastroenterol 19982Klauser et al. Lancet 1990
Typical symptoms of GERD otherthan heartburn Regurgitation (GER) an effortless returnof gastric contents into the esophagus andfrequently into the mouth; often confused withvomiting Dysphagia difficulty swallowingYounes and Johnson. Gastroenterol Clin North Am 1999
Definition Laryngopharyngeal Reflux: a form ofgastroesophageal reflux disease thatproduces prominent symptoms and signs inthe pharynx and larynx characterized byacute, chronic, and intermittent laryngitisand ionary.phpDecember 1, 2010
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Atypical symptoms of GERD Throat clearingGlobusLaryngospasmDental erosion1Mujica Chest painHoarsenessChronic coughSore throatWheezinget al. Postgrad Med 19992DeVault et al. Am J Gastroenterol 1999
Symptom patterns in GERD Reflux-related symptoms occur predominantlyafter meals Reflux-related symptoms are often triggered by––––unusually large mealsfatty, spicy, or acidic foodsbending, stooping, or lying downlifting, straining, or other strenuous activities The frequency of reflux-related symptoms varieswidelyJohnsson et al. Gullet 1992
Distribution of GERD symptomsover 24 hoursLunchDinner45n 1053015Time of dayJohnsson et al. Gullet 1992am6am3ightmidn129pmpm6pm3noon12am9am06Number of episodes ofreflux symptoms/hour(mean x 102)Breakfast
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Prevalence of GERD worldwideHeartburnRegurgitation3-month prevalence (%)2522201415108101011104501817Italyn 999Japann 500Scandinavian 1010Canadan 1036Stanghellini. Scand J Gastroenterol 1999United Statesn 1020
Age-adjusted prevalence of GERD symptoms:the DIGEST studyThe proportion of respondents experiencingsymptoms increased significantly withage (P 0.001).3-month prevalence (%)20151050 2121-3536-50Age in years51-65 65N 5581Includes all respondents from US, Canada, European countries, and Japan.Stanghellini. Scand J Gastroenterol 1999
Frequency of heartburn% 050Daily1/week 1/ week 1/month 1/month 1/monthFrequency of heartburnOliveria et al. Arch Intern Med 1999
Patients with heartburn (%)Severity of GERD symptoms does notcorrelate with severity of disease60No heartburnMild heartburnModerate heartburnSevere heartburn50403020100Grade A(n 1466)Grade B(n 1634)Grade C(n 869)N 4283Levine et al. Am J Gastroenterol 1999Grade D(n 314)
Approximately half of all patients withreflux symptoms have erosiveesophagitisPatients presentingwith reflux symptoms (n 97)Barrett’sesophagusErosive esophagitis46%12%42%No erosive esophagitisWinters et al. Gastroenterology 1987
Symptoms are not reliably predictive ofmucosal damage Patients with and without erosive esophagitisare similar with respect to symptom severity1 Patients with and without erosive esophagitisare similar with respect to symptom frequency1 Patients with different grades of erosiveesophagitis are similar with respect to symptomseverity21Smout.Aliment Pharmacol Ther 19972Lundell et al. Gut 1999
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Pathogenesis of GERD –overview GERD results from exposure of the esophagealmucosa to refluxed gastric contents In most patients with GERD, exposure of theesophagus to refluxate is greater than normal In a minority of patients, exposure is withinnormal limits; in these patients, GERD may bedue to decreased mucosal resistance torefluxate1DeVaultet al. Am J Gastroenterol 19992Dent et al. Gut 19983Shi et al. Gut 1995
Defective esophageal clearance Ineffective peristalsis Reduced salivarysecretion Reduced secretion fromesophageal submucosalglands
LES ‘dysfunction’ Inappropriate andprolonged transientrelaxations Reduction in basalLES pressure/tone
Hiatal hernia May trap a reservoir ofgastric contents abovethe diaphragm,increasing reflux May compromise LESfunction
Increased intra-abdominal pressure PregnancyObesityBendingStrainingCoughingTight clothes
Delayed gastric emptying May result in anincrease in thevolume of gastriccontents availablefor reflux into theesophagus Exact role in GERDremains to beclarified
Causes of increased exposure of theesophagus to gastric refluxate
Medications that may aggravate GERDsymptoms by damaging the esophagealmucosa TetracyclineQuinidinePotassium chloride tabletsIron saltsAspirin and other NSAIDsBisphosphonates
Medications that may aggravate GERDsymptoms by impairing LES function β-adrenergic epressants Progesterone α-adrenergicantagonists Diazepam Calcium channelblockers
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Complications of GERD Esophageal– Barrett’sesophagus– adenocarcinoma– stricture– ulceration– bleeding Extra-esophageal– asthma– reflux laryngitis– vocal cord ulcers– subglottic stenosis– tracheal stenosis
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
Diagnostic methods in GERD HistoryRhinoscopyEndoscopyEmpiric therapypH monitoringRadiology
History History-taking is the primary diagnostic tool forGERD Typical GERD can usually be diagnosed on thebasis of history alone
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
GERD and Chronic Rhinosinusitis Upper respiratory symptoms frequent amongsubjects with symptomatic GERD Dx’d byesophageal study GERD associated with chronic rhinosinusitisin children and adultsTheodoropoulos DS et al. Am J Resp Crit Care Med 2001;164:72-6Barbero GJ. Otolaryngol Clin North Am 1996;29:27-38Phipps CD et al. Arch Otolaryngol Head Neck Surg 2000;126:831-6Ulualp SO et al. Am J Rhinol 199;13:197-202DiBaise et al. Ann Int Med 1998;1291078-83
GERD and Upper Airway DisordersFactors Associated with GERD Lifestyle issues– EtOH, cigarette smoking Obesity Medications– Beta agonists, theophylline, first generationantihistamines Food– High fat diet
GERD and Upper Airway DisordersTheodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
GERD and Upper Airway DisordersPathophysiology Direct irritation by acidNeurogenic reflex (increased vagal tone)Neurogenic inflammationVisceral sensitivity
GERD and Upper Airway DisordersPathophysiology
GERD and Upper Airway DisordersPathophysiologyTheodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
GERD and Upper Airway DisordersPathophysiologyOdds Ratio of GERDURS Score 4URS Score 8URS Score 111.53.86.8Theodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
GERD and Upper Airway DisordersPathophysiologyUpper Airway Symptoms Related toGER or GERD Throat clearing Voice change Hoarseness Cough Post nasal drip Nasal congestionTheodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
GERD and Upper Airway DisordersPathophysiologyUpper Airway Symptoms Possibly Related to GER orGERD Rhinorrhea Ear ache/fullness Sneezing Otitis media with effusion Sinusitis Serous otitis media Sinus Headache Upper airway itchingTheodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
GERD and Upper Airway DisordersPathophysiologyTheodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76
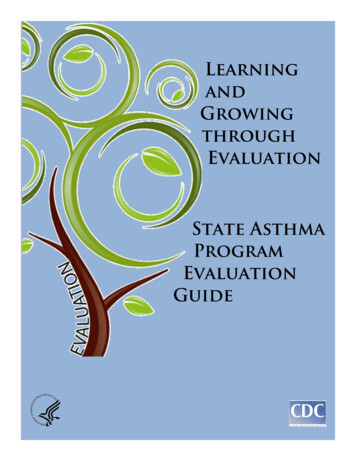
GERD and Upper Airway DisordersNormalFrom www.voiceproblem.orgLarynx with GERD
GERD and Upper Airway DisordersBelafsky Score for Diagnosis of LPR(0-4 score for each component)7 or more is diagnostic of LPR Diffuse edemaSubglottic edemaVentricular obliteration GranulomaVocal fold edemaPosterior commissure hypertrophy
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
GERD and Asthma William Osler noted “ attacks may be due todirect irritation of the bronchial mucosa or indirectly, too, by reflex influences from thestomach ”. Up to 80% of patients with asthma have GERD.Smith LJ, Winslow C. Asthma and Surgery. In Asthma & Rhinitis 2.Bussee W and Holgate S (eds). Blackwell Science 2000, pp 1834-5.
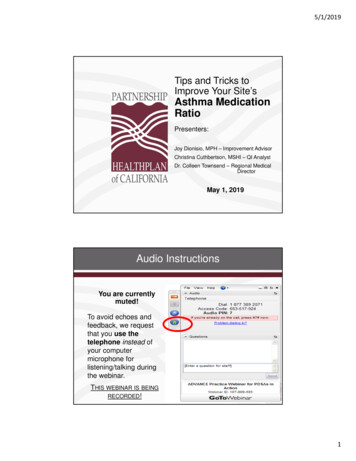
Risk factors for exacerbation ofdifficult-to-treat asthma39 had 3 severe exacerbations/yr136 subjects29 had 1 severe exacerbation/yrBrinke , et al. Eur Respir J 2005; 26: 812.
Conclusions1) Odds ratio (OR) associated with 3 exacerbationsa) severe sinus disease, OR 3.7b) GERD, OR 4.9c) URIs, OR 6.9d) Psychological dysfunction, OR 10.8e) Obstructive sleep apnea, OR 3.42) All patients with frequent exacerbations had 1/5 while52% had 3/5Brinke , et al. Eur Respir J 2005; 26: 812.
Effects of 24 weeks of lansoprazole onasthma in patients with GERD symptomsMulticenter, DB, randomized, placebocontrolled trial of 206 subjects with moderateto-severe asthma with reflux symptoms givenlansoprazole, 30 mg bid vs. placebo.Littner MR, et al: Chest 2005; 128: 1128.
ConclusionDid not improve symptoms by:a) Assessment by:1) participant2) investigatorb) Pulmonary function studiesc) Decrease in albuterol useBut did:a) Decrease asthma exacerbationb) Improve quality of life.Littner MR, et al: Chest 2005; 128: 1128.
Randomized DBPC Study of 770Subjects with GERD and Asthma Randomized to receive esomeprazole 40 mg or P2x QD for 16 wk No statistical difference in morning PEF overall Patients with nocturnal symptoms (NOC) improvedAM PEF 8.7-L/min ( p 0.03) and PM 10.2-L/min(p 0.012) over placebo 304 subjects on LABA improved both AM (12.2L/min, p 0.017) and PM (11.1-L/min, p 0.024)PEF, if they had GERD and NOC Conclusion: esomeprazole improves PEF inpatients with asthma and GERD and NOC Kiljander TO et al. Am J Respir Crit Care Med 2006;173:1091
Cochrane Data Base Review ofGERD Treatment for Asthma in Adults andChildren (2006) 12 randomized controlled trials of Rx for GERD in adultsand children 2 independent reviewers Interventions included proton pump inhibitors (6), H2receptor antagonists (5), surgery and conservativemanagement (1) Temporal relationship in 4 trials found between asthmaand GERD Anti-reflux Rx did not consistently improve lung function,asthma symptoms, nocturnal asthma and medication use Conclusion: No overall improvement but subgroups maygain benefit
Outline1.Definition and Description2.Symptoms3.Prevalence and RD and Upper Airway Disorders8.GERD and Asthma9.Management
GERD and Asthma and Upper Airway DisordersTreatment Empiric acid suppression– Proton pump inhibitors– H2 blockers Lifestyle changes– Diet– Weight loss– Cigarette smoking– EtOH– Elevation head of bed Modification of Rxswhich aggravate GER Increase dose of PPIsafter 6-8 weeks Confirmatory testing orGI consultation
Thank you!
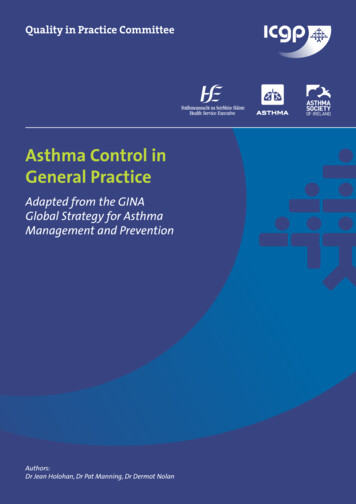
Treatment Data on the Use of Proton-PumpInhibitors and Histamine2-Receptor Antagonists(H2-Blockers)* Healing of esophagitisProton-pump inhibitorSuperior to placebo (83% vs. 18%) at 8 wk; NNTB, 1.7Superior to H2-blocker (83% vs. 18%); relative risk, 0.51Superior to H2-blocker (84% vs. 52%); relative risk, 0.51Significant Dose-response effect at 4 wkLow dose vs. standard dose once daily: NNTB, 10Standard dose vs. high dose once daily: NNTB, 25* Relative risk refers to the probability of treatment failure in the active-treatment group.NNTB denotes number of patients needed to treat to benefit one patient.Kahrilas PJ. N Engl J Med 2008;359:1700-7
Treat
Upper Airway Symptoms Possibly Related to GER or GERD Rhinorrhea Ear ache/fullness Sneezing Otitis media with effusion Sinusitis Serous otitis media Sinus Headache Upper airway itching GERD and Upper Airway Disorders Pathophysiology Theodoropoulos DS, Ledford DK, Lockey RF et al. Am J Respir Crit Care Med 2001;164:72-76