Transcription
Basic Interpretation ofSpirometryChris CrockerCOPD Team
Aims When to do spirometryWhen not to do spirometryDefinition of termsDifferent patterns in spirometryProblemsInterpreting Time/Volume graphs
SpirometrySpirometry is a method of assessing lungfunction by measuring the volume of air apatient can expel from the lungs aftermaximal inspiration
WHY WE DO IT ! Diagnosis confirmationCOPD classificationDisease progressionResponse to treatmentHealth Promotion (Smoking Cessation)Targets
FINDING THE MISSINGMILLIONSNational Clinical Strategy recommends “ Adiagnosis of COPD should be confirmedby quality assured spirometry .”
When not to perform spirometry Inadequate trainingInadequate equipmentLack of quality controlContra-indicationsDuring or immediately after anexacerbation
Contra-indications HaemoptysisPneumothoraxUnstable cardiac statusAneurysmRecent eye surgeryRecent thoracic or abdominal surgeryAcute disorders: D&V, Exacerbations
How we do it! Equipment / spirometers on checksFilters
Patient preparation Pre-test informationDocumentationPatient comfortExplanation/demonstrationSeated, chair with arms
Definition of terms FEV1FVCVC (RVC,SVC,EVC)Ratio FEV1/FVC or FEV1/VC
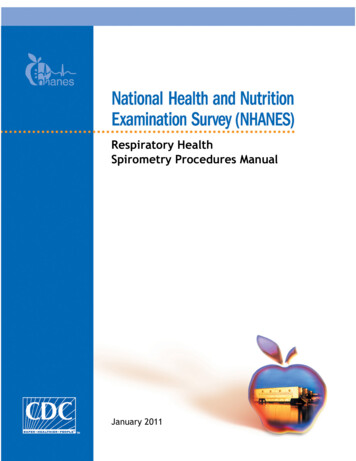
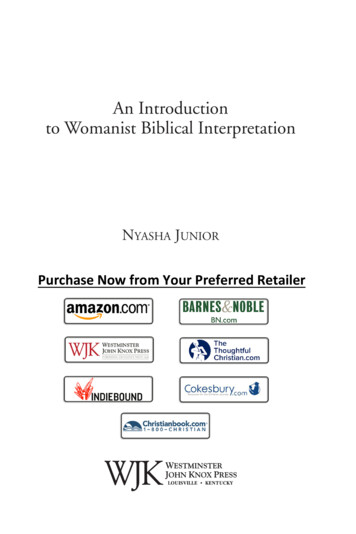
FEV1(Forced Expiratory Volume in 1 second)FEV1Time inseconds
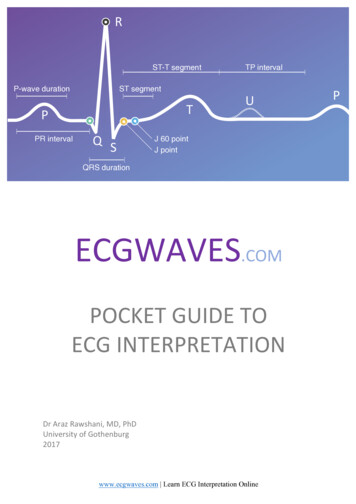
FVCThe maximum volume of air exhaled as rapidly, forcefullyand completely from maximum inspirationFVC
Relaxed Vital CapacityThe maximum volume of air expelledduring a relaxed exhalation from maximuminspiration
FEV1%or Ratio of FEV1 to FVCFEV1/FVC x 100The proportion of air exhaled in one secondThis percentage is important in identifyingairways obstruction
Airflow ObstructionDefinition of airflow obstruction:FEV1 80% predictedandFEV1/FVC 70%
Definition of Chronic ObstructivePulmonary Disease (COPD)COPD is predominantly caused bysmoking and is characterised by airflowobstruction that is not fully reversible.The airflow obstruction does not changemarkedly over several months but isusually progressive in the long term.(NICE 2010)
COPD ClassificationNICE Guidelines Mild COPD FEVı 80% predictedModerate COPD FEVı 80-50% predictedSevere COPD FEVı 50-30% predictedVery Severe COPD FEVı 30% predicted
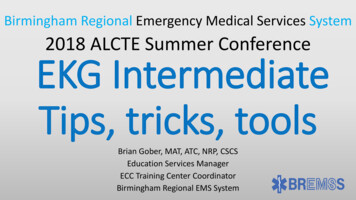
Different Patterns in Spirometry NormalObstructedRestrictedCombined/Mixed
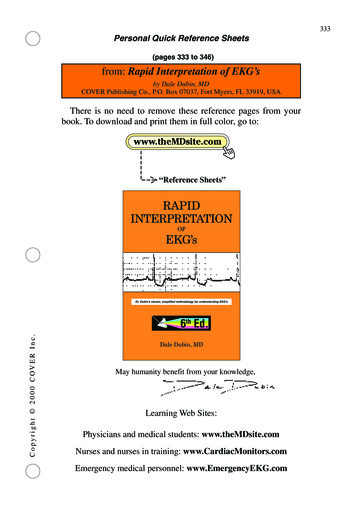
Normal spirometry traceeducation for
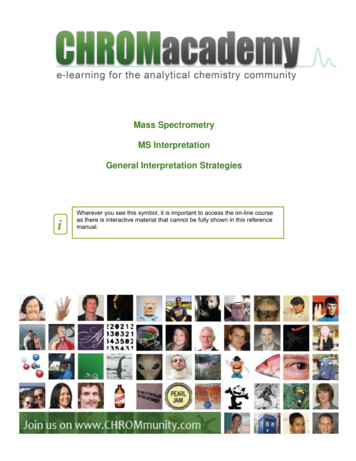
Restrictive SpirometryRestrictive: due to conditions in which the lung volume isreduced, eg fibrosing alveolitis, scoliosis.The FVC and FEV1 are reduced proportionately.
Reporting Spirometry Results should be the greatest valuesachieved from 3 technically acceptableblows. (FEV1 within 5%) Poorly performed spirometry is worse thanno spirometry!
QUALITY?National strategy cites an example:31% of spirometry measurements in 38practices in Rotherham met therequired standard of 3 readings within5% ( in contravention of BTS and GOLDspirometry standards)
New Guide to Spirometry!!! A Guide to Performing Quality AssuredDiagnostic Spirometry www.pcc.cic.org.uk
Problems! Slow startShort BlowCoughLeaks around mouthpieceSub-maximal effortUnable to achieve 3 acceptable resultsInadequate rest between attempts
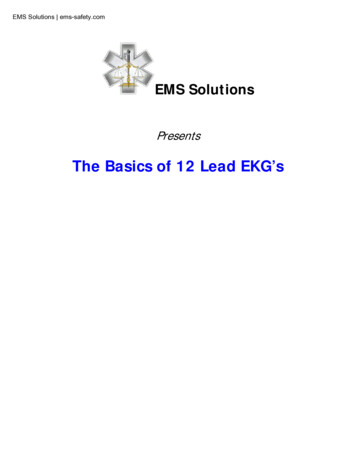
Parameters of Lung FunctionNormalObstructive Restrictive CombinedFVC 80%NormalReducedReducedFEV1 EV1/FVC 70%
Reading the tracing Is the spirometry valid ?Check sex/age/height/weight/BMICheck tracing for problemsIdentify ACTUAL ratio ? obstructionIdentify FEV1 and % predictedCheck VC and FVC ? Air trapping ? Reduced volumesRemember to use largest measurement from validblows, (these may not all be from one blow) Do the figures fit with the tracing? Interpret together with history, symptoms and medication
Training Do not perform spirometry withouttraining ARTP (www.artp.org.uk) EQUIP (www.essexequip.nhs.uk) Education for health(www.educationfor health.org.uk)
Thank you for listeningAny Questions ?
Definition of Chronic Obstructive Pulmonary Disease (COPD) COPD is predominantly caused by smoking and is characterised by airflow obstruction that is not fully reversible. The airflow obstruction does not change markedly over several months