Transcription
Excellence in Continence CareEnglandYEARSOF THE NHS1948 - 2018EXCELLENCEin Continence CarePractical guidance forcommissioners, andleaders in health andsocial carewww.england.nhs.uk1
NHS England Reader Information BoxDirectorateMedicalNursingFinanceCommissioning OperationsTransformation and Corporate OperationsPatients and InformationCommissioning StrategyPublications Gateway Reference: 08266Document puropse:StrategyDocument name:Excellence in Continence Care: Practical guidance for commissioners,and leaders in health and social careAuthor:NHS EnglandPublication date:June 2018Target audience:CCG Clinical Leaders, CCG Accountable Offcers, Foundation Trust CEs , MedicalDirectors, Directors of PH, Directors of Nursing, Local Authority CEs, Directorsof Adult SSs, NHS Trust Board Chairs, NHS England Directors of CommissioningOperations, Directors of Finance, Allied Health Professionals, GPs, CommunicationsLeads, Directors of Children’s Services, NHS Trust CEs, members of the publicAdditionalcirculation list:N/ADescription:Practical guidance for commissioners, providers, health and social care staff to putinto effect best careCross ref:N/ASuperseded docs:(if applicable)Excellence in Continence Care: Practical guidance for commissioners, providers,health and social care staff and information for the public (November 2015)Action required:N/ATiming/deadlines:(if applicable)N/AContact details forNHS England, Quarry House, Quarry Hill, Leeds, LS2 7UEfurther information:Document status:This is a controlled document. Whilst this document may be printed, the electronic version posted on thewebsite is the controlled version. Any printed copies of this document are not controlled. As a controlleddocument, this document should not be saved onto a local or network drive but should always beaccessed from the internet.Equality and Health Inequalities StatementPromoting equality and addressing health inequalities are at the heart of NHS England’s values. Throughout thedevelopment of the policies and practices cited in this document, we have given due regard to: Eliminate discrimination, harassment and victimisation, to advance equality of opportunity and to foster goodrelations between people who share a relevant protected characteristic (as cited under the Equality Act 2010)and those who do not share it; and Reduce inequalities between patients in access to, and outcomes from, healthcare services and to ensureservices are provided in an integrated way where this might reduce health inequalities.
Excellence in Continence CareContentsExecutive summary4Reducing healthcare related harm and costs5Commissioning for dignity and value10References203
4Excellence in Continence CareExecutive summaryContinence is an important component in aperson’s health and well-being at any stage oflife and is also an important factor in the use ofhealth resources for the following reasons: Normal bowel and bladder function is animportant part of a child’s development andtheir path to adult and independent living.Failure to acquire control in a timely mannerwill affect schooling and education. Adult incontinence produces markedloss of self-esteem, depression, loss ofindependence, and can affect relationshipsand employment prospects. In older people, incontinence and associatedbladder and bowel disorders may beassociated with physical problems such asskin breakdown, falls, urine infection andcatheter associated urinary tract infectionwhich in turn often causes confusion.Confusion can result in falls, head injury orfemur fractures requiring an acute hospitaladmission. Incontinence or dependence on a urinarycatheter signifcantly increases the level ofdependency in frail older people. This maydelay discharge from hospital or initiatea move into a residential or nursing caresetting.This guidance is a refreshed and updatede-resource that builds on an earlier publicationfrom November 2015. To help ensure peoplereceive excellent continence care, considerationshould be given to: Early assessment by an appropriately trainedprofessional allows a patient centred and costeffective care pathway to be followed. Afterassessment the use of containment products,medication and the level of intervention canbe triaged and escalated. Effectively resourcing the continence teamand its management structure as part of anintegrated service. How local people may need more specialistassessment which should be provided basedon population needs. Containment with the use of pads orcatheters may be the only realistic optionfor some people, but this management hasassociated problems. Actively support the individual to participatein the management and treatment of theircontinence care. Simple approaches to care delivery, includingelectronic and telecommunications, can helppeople lead healthy lives as well as providingadvice and support to implement bestpractice or services in organisations.Minimum standards which help buildcompetence and knowledge for the workforceinvolved in continence care are included in thisdocument. For further supporting informationon specifc roles and responsibilities go towww.england.nhs.uk/commissioning/continenceThis guidance is intended to assistcommissioning discussions for those developinghigh quality community continence servicesand provides a valuable supporting resource forthe wider STP planning process.
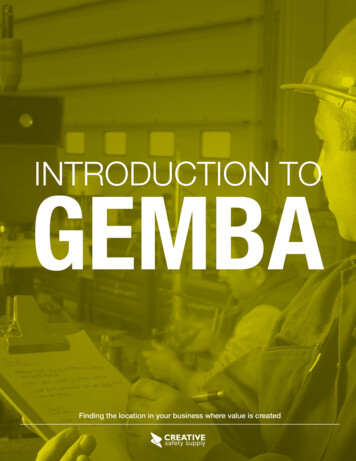
Excellence in Continence CareReducing healthcare relatedharm and costsThe case for changeThe NHS Five Year Forward View1 puts anemphasis on prevention and keeping peoplewell for longer. Prevention is a key part of anystrategy to minimise harm and reduce healthcare costs.PreventionThe Prevention PyramidThe All Party ParliamentaryGroup for Continence Care hasdesigned a Prevention Pyramid showinghow risk and costs are reduced wherecare is underpinned by high qualityintegrated community continenceservices. These services not only provideexpert treatment within the communitybut advice regarding self-help strategies.Skills include training colleagues ininitial continence assessment andconservative treatments and ensuringthat referrals to secondary care aremade where appropriate. Movementup the pyramid can be delayed orprevented by an integrated continenceservice with a traffc light systemillustrating the risks and rising costs ofuntreated continence needs.In an ageing population, greater prevalenceof bladder and bowel problems and the widerange of care groups affected, mean thatcontinence services require a higher priority.Effective community based continence servicescan save valuable NHS resources whilstrestoring dignity to people and improvingquality of life2.Incontinence is reported as a signifcant reasonfor care home admissions3. Variation in serviceprovision and practice is a particular area ofchallenge. There appears to be no consistencyas to the frequency of continence assessments.Physical harm related to complications andtreatments for continence problems forexample pressure ulcers, urinary tract infection,catheterisation and faecal impaction can alllead to admission to hospital and care facilitiesfor extended lengths of stay and sometimespermanently.Reviewing the evidenceThe National Audit of Continence Care4found that many services were not providingservices in line with NICE guidance and that thequality of care is worse among older patientsover the age of 65 in whom the condition ismost prevalent5, 6. Of women suffering from‘moderate’ or ‘severe’ urinary incontinence,fewer than one third were found to bereceiving health or social services for theircondition7.5
6Excellence in Continence CareTowards the aim of reducing healthcare relatedharm and costs, the Leading Change, AddingValue - a framework for nursing, midwiferyand care staff8 sets out a systematic way ofaddressing gaps in services and unwarrantedvariation across the system. The frameworkrecognises the importance of being able tomeasure the impact for the improvement ofoutcomes for local people.The principles embodied in the NHSImprovement programme Getting it Right FirstTime9 should be applied to continence care asit recognises the importance of access to earlyassessment and diagnosis and the focus onimproving the patient experience.Towards these aims, pathways of care shouldbe commissioned that ensure early assessment,effective management of incontinence, alongwith other bladder and bowel problems suchas constipation and urinary tract infections andtheir impact on social, physical and mentalwell-being and existing comorbidities in orderto reduce expensive pad usage, high costcomplications and unnecessary hospital andcare home admissions.It is estimated that 14 million men, women,young people and children of all ages are livingwith bladder problems, roughly the equivalentsize of the over 60 population in the UK10.It is also estimated that 61% of men in thegeneral population experience lower urinarytract symptoms11, 12 (LUTS) and around 34% ofwomen are living with urinary incontinence13.In addition, 900,000 children and youngpeople suffer from bladder and boweldysfunction14, 15. Bowel and bladder problemshave more impact than almost any othermedical condition on children’s self-esteem,education and social relationships, andeffective treatment can change children’s lives(Dr Eve Fleming, ERIC Trustee).6.5 million adults in the UK suffer withsome form of bowel problem. 1 in 10 of thepopulation are affected by faecal incontinence,with over half a million adults suffering fromfaecal incontinence, with a negative impact ontheir lives16. It is likely that 0.5-1% of adultsexperience regular faecal incontinence thataffects their quality of life17, 18.Faecal incontinence is closely associated withage (prevalence is about 15% in adults aged85 years living at home) and is more commonin residential and nursing homes19 (prevalenceranges from 10-60%) (APPG 2011; NICECG171, 2013).Urinary and faecal incontinence are conditionsaffecting one in three people living inresidential care and two in three nursinghome residents20. Inadequate management ofincontinence can lead to escalating costs dueto morbidity and unnecessary hospitalisation.The rate of emergency admissions due to aurinary tract infection (UTI) has almost doubledover the last fve years to 60 per 100,000population placing additional pressure on acutesettings which could often be avoided throughearly continence intervention.
Excellence in Continence CareIn 2012/13 unplanned admissions for urinarytract infections (UTIs) cost 432 million peryear, averaging 2.1 million per CCG21. Patientswith incontinence are at increased risk ofhospital acquired UTI which extends lengthof stay by 6 days. In 2010, 27,000 men werehospitalised for untreated LUTS22 (NICE CG139,2012).Catheter associated urinary tract infections(CAUTI) have signifcant associated costs ofadditional bed days and treatment, estimatedto cost the NHS up to 99m p.a., or 1,968 perepisode. Patients are often catheterised in wayswhich could have been avoided through goodcontinence care. Nearly one third of urinarycatheter-days are inappropriate in medicaland surgical inpatients with 26% of cathetersinserted in Accident and Emergency having noappropriate indication, suggestive that manycatheters are inserted unnecessarily23, 24.Urinary tract infections are the most commonhealthcare acquired infection (HCAI),comprising 19% of all HCAIs; 43-56% ofUTIs are associated with urethral catheters;approximately 17% of secondary nosocomialbloodstream infections are caused by catheteruse, with an associated mortality of 10%(Loveday et all 2014).Urinary catheters as a source of bacteraemiahave seen an increase in both the numbers ofcases and as a proportion of cases withsource information between 2015/16 and2016/17 and will require further effort toreduce this25, 26,.Gram negative septicaemia is most commonlycaused by UTIs and is considered to someextent to be preventable through goodquality continence and medical care. NHSImprovement have mandated that all NHSTrusts have a strategy to reduce incidence by10% in 2017 and by 50% in 202027, 28. Thiswill require a collaborative approach across thewhole health and social care system to achievethis.In 2015, GP prescribing data29 illustratesthere were 1.1 million prescription items forcatheters at a cost of 115.1 million pounds,an increase of 7.1% from 2014.The 2013 Continence Care Services reportfor England30 indicated that catheterisationis often a consequence of poor continencecare. Continence services working closely withinfection teams and GPs is the most effectiveway to either avoid urinary catheterisationaltogether or else to shorten the duration ofinsertion.Poor continence care is a contributory factorto pressure ulcers31. Nearly 700,000 people areaffected by pressure ulcers each year, acrossall care settings. Each pressure ulcer costs anaverage of 4,638 - which creates a fnancialburden on the NHS of between 1.4 and 2.1billion per year. Savings could be made byreducing the number of people who developpressure ulcers; good continence care plays animportant role in their prevention.7
8Excellence in Continence CareBowel-related costsIn the period 2010/11, it was reported that57,000 hospital admissions in England weredue to constipation. In 2010, 103 deathswere registered in England and Wales withconstipation cited as a contributory factor.Public Health England publishAMR indicators intended toraise awareness of antibioticprescribing, antimicrobial resistance,healthcare associated infections,infection prevention control andantimicrobial stewardship. Theseindicators are available at: atorsNHS Improvement publishedan on line improvementresource to help health andsocial care economies reduce thenumber of gram-negative bloodstreaminfections with an initial focus onEscherichia coli (E.coli) to support thedelivery of the national ‘Reducingthe impact of serious infections(Antimicrobial Resistance an
Incontinence or dependence on a urinary catheter signifcantly increases the level of dependency in frail older people. This may delay discharge from hospital or initiate a move into a residential or nursing care setting. This guidance is a refreshed and updated e-resource that builds on an earlier publication from November 2015. To help ensure people