Transcription
Stroke PatientEducation WorkbookA Guide to Understanding StrokeThis workbook is designed to help you become a well-informed participant inyour health care decisions regarding your stroke. We hope this will help you betterunderstand stroke and guide you through your recovery and rehabilitation.www.hoag.org/stroke
ForwardA Guide to UnderstandingStrokeIt is our sincere hope that this stroke patienteducation workbook will provide you and your lovedones with helpful information. This is designed tobe your personal workbook during your stages ofrecovery. Understanding what happens when astroke occurs and being a knowledgeable participantin your treatment plan are essential for your recoveryand rehabilitation.This workbook is organized to help you understandthe general and specific information regarding yourstroke. If you or a family member have questionsafter reading this material or at any time, pleasecontact the Neuroscience Stroke Nurse Navigatorat 949-764-8273.Some of the enclosed materials were selected frompublications of The National Stroke Association,The American Heart Association/American StrokeAssociation, Brain Aneurysm Foundation,The American Academy of Sleep Medicine, andThe Brain Attack Coalition.Hoag Stroke Program TeamPickup Family Neurosciences Institute949-764-6066iii
Table of Contents –A Guide to Understanding StrokeIntroductionLife After StrokeWelcome to Hoag’s Stroke Program . . . . . . . . . . . 1Meet the Team Members. . . . . . . . . . . . . . . . . . . . 1What to Expect During Your Hospital Stay. . . . . . . 3All About Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . 3Warning Signs of Stroke . . . . . . . . . . . . . . . . . . . . 5More Stroke Facts. . . . . . . . . . . . . . . . . . . . . . . . . 6Frequently Asked Questions . . . . . . . . . . . . . . . . . 6Take These Step to Prevent a Second Stroke. . . . . 7Job Retraining/Volunteering. . . . . . . . . . . . . . . . . 46Driving . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Sexuality. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Risk Factors and PreventionFamily InvolvementRisk Factors and Prevention . . . . . . . . . . . . . . . . . 8Uncontrollable Stroke Risk Factors . . . . . . . . . . . . 9Controllable Stroke Risk Factors . . . . . . . . . . . . . . 9The Caregiver’s Role. . . . . . . . . . . . . . . . . . . . . . 51Taking Care of Yourself . . . . . . . . . . . . . . . . . . . . 52Working Together . . . . . . . . . . . . . . . . . . . . . . . . 54Effects of StrokeCommunity ResourcesYour Brain and You. . . . . . . . . . . . . . . . . . . . . . . 11Right-Brain vs. Left-Brain Stroke. . . . . . . . . . . . . 13Characteristics Based on Location of Stroke . . . . 14Physical Effects. . . . . . . . . . . . . . . . . . . . . . . . . . 14Caregiver’s Bill of Rights . . . . . . . . . . . . . . . . . . . 55A Caregiver’s Resource Guide. . . . . . . . . . . . . . . 55Where To Turn For Help. . . . . . . . . . . . . . . . . . . . 56Palliative Care Medicine Consult Serviceat Hoag Hospital. . . . . . . . . . . . . . . . . . . . . . . . . 58MedicationsMedications To Help Manage and Prevent Stroke. 17RehabilitationYour Rehabilitation Program. . . . . . . . . . . . . . . . . 21Personal Care. . . . . . . . . . . . . . . . . . . . . . . . . . . 23Mobility. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Home Safety Tips. . . . . . . . . . . . . . . . . . . . . . . . 28No Such Word As “Can’t” . . . . . . . . . . . . . . . . . . 29NutritionIntroduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Healthy Eating After A Stroke. . . . . . . . . . . . . . . . 30Dysphagia Diet Summary. . . . . . . . . . . . . . . . . . . 32Fat Facts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Healthy Substitutions to Reduce Fat . . . . . . . . . . 35Sodium-Controlled Diet. . . . . . . . . . . . . . . . . . . . 38Understanding Food Labels. . . . . . . . . . . . . . . . . 41Eating Out. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Recommended Books/Cookbooks . . . . . . . . . . . 45ivLifestyle ModificationSmoking Cessation. . . . . . . . . . . . . . . . . . . . . . . 49Stop Smoking Directory. . . . . . . . . . . . . . . . . . . . 49Stress Management . . . . . . . . . . . . . . . . . . . . . . 50AppendixGlossary. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Meet the TeamMembersHoag Stroke ProgramMission StatementHelping you to maximize your recovery is a multidisciplinary team effort. The stroke team includesdoctors, nurses, nursing aides, respiratory therapists,physical therapists, occupational therapists, speech/language pathologists, care managers, socialworkers, dietitians, your family, friends, and YOU.Stroke patients at Hoag receive the highest levelof care through a patient-centered, integrated,multidisciplinary team approach, using the best inevidence-based practice, state-of-the-art technologyand advanced research.Pickup Family Neurosciences Institute’s StrokeProgram is DNVGL certified as a ComprehensiveStroke Center at its Newport Beach campus, anda Primary Stroke Center at its Irvine campus. HoagStroke Program has received the American StrokeAssociation’s “Get With the Guidelines” – StrokeGold Plus Performance Achievement Award and theTarget Stroke Honor Roll Elite Award.Our Stroke Program is patient-centered with anadvanced approach to caring for our patients. TheStroke Team is multidisciplinary involving nurses,therapists, care managers, social workers as well asphysicians from other specialties to assure optimalmedical management and therapies are provided toeach of our stroke patients.Hoag Newport Beach is designated a StrokeNeurology Receiving Center with Orange County EMS.IntroductionWelcome to Hoag’sStroke ProgramYour physician will determine which members ofthe multi-disciplinary team will assist you in yourrecovery. Although these professionals have differentspecialties, they share a common goal of helping youto recover.Primary Care PhysicianYour primary care physician or hospitalist directs andplans your medical care in cooperation with yourneurologist and neurosurgeon.NeurohospitalistYour neurohospitalist is a hospital-basedneurologist who diagnoses and treats diseasesof the nervous system.Stroke Program Medical DirectorThe Stroke Program Medical Director is aNeurohospitalist who is fellowship trained in strokeand cerebrovascular disease. He oversees anddirects the care of the stroke patient in conjunctionwith the other physicians, nurses and staff thatmake up the stroke team. He also ensures thatpatients receive consistent, state-of-the-art care inaccordance with the latest scientific research.Registered NurseYour registered nurse (RN) will assist your progress,monitor your recovery and administer yourmedications. Throughout your hospitalization, yourRN will assess your neurological function, level ofpain, signs and symptoms of any complications.Your RN will educate you regarding prevention ofcomplications and help communicate any concernsthat you and your family may have to your physiciansand other healthcare members.Patient Care AssistantYour patient care assistant will help you withpersonalized care and daily needs. He or she mayalso perform procedures such as blood pressure,temperature and drawing of blood.1
IntroductionStroke Program Nurse NavigatorYour stroke program nurse navigator workscollaboratively with the physicians, nurses andmultidisciplinary team to oversee your care andmanage quality improvement. Your navigator willalso assist with your education regarding strokesigns and symptoms, treatment and preventionof complications, and will meet with you and yourfamily to assess your individual needs. At 30 daysand 90 days after discharge, you will receive a phonecall from your navigator to assess your progress andreinforce any education. Hoag’s nurse navigator alsocoordinates the monthly support group meetingsand educational flyers mailed to your home.Respiratory TherapistYour respiratory therapist (RT) works with thehealthcare team to help maintain and/or improvethe health of your lungs. He or she will assist youwith breathing exercises, breathing medications,ventilator care and coughing techniques.Speech/Language Pathologiststrength, and function of the arms, and may utilizemodified techniques and/or adaptive equipment.OTs will also address problems related to vision,perception, problem-solving, safety, reasoning,decreased sensory awareness, sitting balance/endurance and positioning. One of the importantaspects of therapy is the education and training forthe patient and caregiver.Physical TherapistPhysical therapists (PT) will help you regain the abilityto be mobile again. They focus on deficits in yourstrength, balance, stamina, coordination and safetyto help you regain bed mobility along with the abilityto stand up, balance, walk, and navigate stairs.Your PT will also assess the need for any equipmentsuch as a cane or walker, address any safety issuesfor returning home, and provide training for youand your family that will assist you through a safetransition back to self sufficiency.Care ManagerYour speech/language pathologist (SLP) will workwith you and your family to evaluate and treatany problems you may have in your ability to uselanguage. If needed, the SLP will assess your abilityto swallow. Following this assessment, he or shemay make recommendations to your physician toensure safety in swallowing, adequate nutritionalintake and prevention of aspiration.Your care manager is an RN or social worker whoassesses your status and evaluates your treatmentplans throughout your hospital stay. He or she worksclosely with your primary physician, healthcareprofessionals and family to develop a qualitydischarge plan and coordinate all options for posthospital continued care, including transitionto a lower level of care, alternative medical services,durable medical equipment and supplies.Dysphagia/Dietary TeamSocial WorkerYour physician may initially order no liquids or foodby mouth (NPO) until your swallowing ability hasbeen evaluated. The dysphagia team will evaluate ifyou have difficulty swallowing (dysphagia). After theevaluation, the dysphagia team will recommend anappropriate diet.The primary goals of the dysphagia evaluation areto ensure that swallowing is safe (no food or liquidgoing down the airway), and that intake of food/liquidis efficient and sufficient.Occupational TherapistOccupational therapists (OT) will assist you inmanaging activities of daily living (ADL) such asself-feeding, bathing, dressing, home managementskills and community re-entry. These tasks areaccomplished by working to improve coordination,2The clinical social worker is a licensed professional(LCSW) who will help provide you and your familywith emotional counseling, crisis intervention,support groups and community resourceinformation.DietitianThe dietitian works with your doctor to meet yournutritional needs. He or she may check your eatinghabits and teach you about your diet. He or she willmake sure that meals are healthy and tasty.ChaplainThe hospital chaplain is available to providespiritual guidance and emotional support foryou and your family.
Hoag Stroke Program follows evidence-basedstate-of-the-art stroke treatment protocols. Onceyour stroke is diagnosed via clinical assessmentand brain imaging, treatment begins to help stabilizeyour symptoms. Then additional assessment isinitiated to identify the reason for your stroke andthe risk factors involved. The treatment of yourstroke entails a through cerebrovascular and cardiacdiagnostic evaluation.At the bedside, you will be evaluated daily bythe Stroke Team to update you and your family ondiagnostic results, medications and rehabilitationneeds. A key component once the assessment iscomplete and you are medically stable, is to initiaterehabilitation evaluations by the physical therapist,occupational therapist and speech therapist.Aggressive rehabilitation is an essential part of yourphysical and cognitive recovery. A care manager willalso visit you routinely to assist you and your familywith discharge and other social needs.This Stroke Patient Education Workbook will bereviewed with you and your caregivers to help youunderstand the type of stroke you suffered andthe cause of the stroke. In addition, importanteducational topics such as the signs and symptomsof stroke, calling 9-1-1 at the first signs ofsymptoms, your risk factors and recommendationsfor stroke risk reduction.You are the most important individual of your strokerecovery and our goal is to practice a holisticapproach addressing your physical, emotional,spiritual and social needs to maximize your recovery.IntroductionWhat to Expect DuringYour Hospital StayAll About StrokeWhat is a Stroke?Stated simply, a stroke is an injury to the braincaused by an interruption of the blood supply. Braincells must have a continuous supply of blood. Whena person has a stroke, this continuous supply is cutoff and the brain cells suffer damage.The brain also must receive oxygen and nutrients(such as glucose) from the blood vessels. Whenbrain cells do not function, neither do the partsof the body controlled by those brain cells.The extent and location of the injury to the braindictates which brain functions are affected bythe stroke.A stroke is a sudden unexpected happening withdiverse results. Some stroke patients recover to adegree that normal life can be resumed. Some strokepatients have residual damage (loss of function)that is not recoverable. No two stroke patients haveexactly the same injuries or disablements.Disability from stroke can take many formsdepending on the area of the brain that is damaged.The stroke’s effect may be slight and temporary or itmay be serious, even fatal. A typical stroke survivormay not be able to use his or her right or left sideof the body, or may have communication problemssuch as not being able to speak or read. Everystroke is different.Because a stroke patient’s recovery is both medicaland rehabilitative, the recovery continues over aperiod of time, which can be weeks, months, or evenyears. Sometimes the damage done to the braincells cannot be overcome. Only time can tell theoptimum recovery for each patient.If you or your loved one has had a stroke, you arenot alone. Every 40 seconds someone in the UnitedStates will experience a stroke. This amounts toapproximately 795,000 people a year. Currently, about610,000 people suffer first strokes each year. Thesenumbers are expected to increase significantly as aresult of an increase in the country’s aging population.3
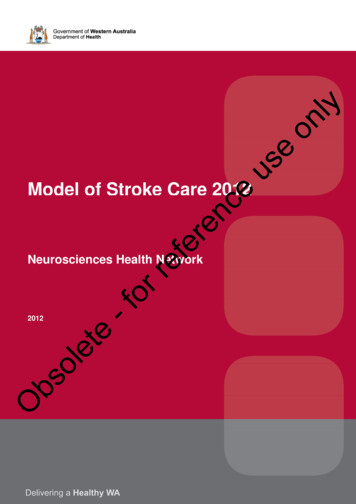
IntroductionTypes of StrokeThere are two types of stroke: ischemic and hemorrhagic. The majority (87 percent) of all strokes are ischemic,while the remaining 13 percent are hemorrhagic.Ischemic StrokesHemorrhagic Strokesclot causingembolic strokeburst aneurysm causingsubarachnoid hemorrhageplaque causingthrombotic stroketorn artery causingintracerebral hemorrhageIschemic StrokeHemorrhagic StrokeThe most common type of stroke, an ischemic stroke,occurs when a blood clot blocks an artery cutting offthe flow of blood to the brain. Without enough oxygenbeing delivered to the affected area, brain cells willbegin to die and stroke survivors will start to haveproblems using certain parts of their bodies.Strokes caused by a bursting blood vessel in the brainthat spills blood into the brain are called hemorrhagicstrokes. High blood pressure and brain aneurysmscan both cause the wall of a brain artery to becomeweak, and possibly result in this type of stroke.There are two types of ischemic strokes: embolicand thrombotic. During an embolic stroke, a bloodclot (embolus) or other undissolved piece of materialmoves through the body and lodges in a brain arterycutting off the supply of blood. A thrombotic stroke,a blood clot (thrombus) forms in the brain artery andblocks the flow of blood.4There are two types of hemorrhagic stroke:intracerebral and subarachnoid. An intracerebralhemorrhage is caused when a ruptured bloodvessel bleeds into the tissue deep within the brain.The bleeding causes brain cells to die, and thatpart of the brain no longer functions correctly. In asubarachnoid hemorrhage, a blood vessel burstsnear the surface of the brain and bleeds into the areabetween the brain and the skull. This bleeding mayincrease pressure in the brain, injuring brain cells.
IntroductionWhat is a Transient Ischemic Attack (TIA)?If an artery leading to the brain, or inside the brain,becomes blocked for a short period of time, theblood flow to an area of the brain slows or stops.This lack of blood and oxygen can cause temporarysymptoms that are similar to a stroke. Thesesymptoms usually last 5 minutes or less and leaveno permanent injury to the brain.TIAs are a serious warning sign of stroke and shouldnot be ignored. As many as 20 to 40 percent ofpeople who experience a TIA go on to have a stroke.MECHANICAL TREATMENT TO PHYSICALLYREMOVE THE CLOT Acute Stroke TreatmentManagement of Ischemic andHemorrhagic Stroke The first step is determining if the stroke is causedby the interruption of blood flow (ischemic) or bybleeding from an abnormal vessel (hemorrhagic)with rapid brain imaging.Clot Dissolving or Clot Removalfor Ischemic StrokeMEDICATION TREATMENT WITH ALTEPLASE –INTRAVENOUS (IV) TPA TO DISSOLVE THE CLOT Tissue plasminogen activator (tPA) or Alteplaseis the only FDA-approved medication for thetreatment of acute ischemic strokes.When promptly administered, it can save lives andreduce the long-term effects of stroke.Alteplase (tPA), is given through an IV in the arm. Itworks by dissolving the clot and improving bloodflow to the affected part of the brain.Alteplase (tPA) needs to be given within 4.5 hoursof having a stroke in eligible patients.Many people miss this key brain-saving treatmentbecause they don’t arrive at the hospital in timefor Alteplase (tPA) treatment. This is why it’s soimportant to identify a stroke and seek treatmentimmediately for the best possible chance at a fullrecovery. Physical removal of a blood clot in a large bloodvessel in the brain causing the stroke is called amechanical thrombectomy.This procedure has been clinically proven toprevent or reduce disability in many patientssuffering from a stroke due to occlusion of a largebrain artery, regardless of whether IV Alteplase(tPA) is given or not.To remove the clot, a specially trained doctorthreads a long tube, called a catheter, through anartery in the groin up to the blocked artery in thebrain using image guidance.Two different devices may be used to removethe clot: Stent retrievers grab the clot, which isthen removed with the stent; Aspiration cathetersremove the clot with suction. These devices mayalso be used together.Patients must meet strict criteria to be eligiblefor this procedure, so that the potential benefitoutweighs the risks of the procedure.Some patients will meet criteria for bothMedication Treatment with IV Alteplase (tPA) andMechanical Thrombectomy.RISKS OF IV ALTEPLASE (TPA) The main risk of IV Alteplase (tPA) is that it cancause serious bleeding in the head or body.If bleeding happens in the brain, it can causeworse stroke symptoms or even death.Doctors are very careful about using IV Alteplase(tPA). For example, a brain scan is done beforeTPA treatment to make sure you have no signs ofbleeding.After treatment, you are closely watched for the first24 hours in an Intensive Care Unit to make sure youhave no internal bleeding or allergic reactions.If you notice any headache, tongue swelling,bleeding gums, nose bleeding, bloody urine orstool; notify your nurse immediately.5
Warning Signsof StrokeRISKS OF MECHANICAL THROMBECTOMY The risks of thrombectomy are mainly related tothe procedure itself. Risks include bleeding wherethe catheter was put in and a tear or suddenclosure of a blood vessel.Doctors
and rehabilitation. This workbook is organized to help you understand the general and specific information regarding your stroke. If you or a family member have questions after reading this material or at any time, please contact the Neuroscience Stroke Nurse Navigator at 949-76