Transcription
A Biannual Publication of theGeorgia Regents Digestive Health CenterDIGESTIVEMATTERSADVANCED ENDOSCOPY:STATE-OF-THE-ART FACILITIES AND HOWADVANCED ENDOSCOPISTS ARE CHANGINGLIVES AND MEDICINE IN GEORGIAP4WINTER 2015VOLUME 1 ISSUE 2
MESSAGE FROM THE DIRECTORWelcome to the second volume ofDigestive Matters. It is amazinghow time flies and six monthshave elapsed since the previous edition.Although we have made many strides inseveral disciplines within digestive health andhave cured many patients with a variety ofproblems and yes, would love to share themall space constraints dictate otherwise.You will learn first-hand how our expertsin the Digestive Health Center, notably Drs.John Affronti, Subbaramiah Sridhar andSumanth Daram are using their unique skillsand talents to diagnose and treat complexgastrointestinal problems that is only possibleat the DHC.You will read about Frank Thomas who wasreferred with an unsuspected growth in hisesophagus (food pipe) and how endoscopicultrasound and a new minimally invasivetechnique of video-assisted thoracoscopicsurgery (VATS) performed by Dr. CarstenSchroeder, a nationally renowned thoracicsurgeon enabled his full recovery.“A positive attitude is contagious, but don’t wait to catch it from others, be a carrier.”AnonymousAnd then there is Allen Rowe whopresented with flu-like symptoms andjaundice and who was initially diagnosedwith a stricture (blockage) of bile ducts (pipesthat connect the liver with the intestine),possibly due to a cancer. Dr. Daram used thenovel revolutionary technique of Spyglass, aninstrument half the thickness of a pencil, tofacilitate a surprise diagnosis.The Digestive Health Center has sixregular endoscopy rooms and three advancedendoscopy and fluoroscopy suites withstate-of-the-art facilities for both diagnosisand management of pancreatico-biliarydisorders as well as complex cancers in theabdomen and chest. We use minimallyinvasive technology without major surgeryfor diagnosis and treatment of gallstones,strictures, pancreatic cysts, endoscopicremoval of large polyps, radiofrequencyablation of Barrett’s dysplasia, endoscopicmucosal resection and celiac plexus block forchronic abdominal pain or for stenting of2many digestive organs.Also in this issue we are introducing a newSection “DHC Highlights” that will providea GI quiz for diagnosis, a practical tid-bitfor diet and nutrition, a top-line summaryof the latest advances in GI/hepatology andupcoming DHC news.Finally, we wish to share some of the keyfeatures and outstanding achievements of ourDHC team which are summarized in ourannual report.The DHC not only provides world-classhealth care, but its research team is toilinghard to develop the next best test to improvediagnosis of common GI problems and topioneer new treatments where there is none.We implore you to please join us in ourcampaign to promote colon cancer awarenessthrough early diagnosis and treatment, curehepatitis C, prevent and treat obesity, developcutting-edge therapies for ulcerative colitisand Crohn’s disease, and quite importantlyto diagnose and treat gastroparesis, fecalincontinence, IBS and constipation. Towardthis important mission, we are launching afundraising campaign to support our researchinfrastructure and research programs. We hopeyou will consider supporting our endeavors,so that we can provide the best care for ourpatients and keep our department on thecutting edge. To learn more about how youcan make a gift, please contact David Cantrellat 706-721-1817 or dcantrell@gru.edu.I trust you will enjoy reading this issue, andplease contact me with suggestions or advice.Respectfully,Satish SC Rao, MD, PhD, FRCPProfessor of MedicineChief, Gastroenterology/HepatologyDirector, Georgia RegentsDigestive Health Centergrhealth.org/digestivehealth
IN THIS ISSUEWINTER 2015In this issue, you will discover howthe new generation of cutting-edgetechnology has revolutionized ourapproach and management of complexgastrointestinal problems at the DigestiveHealth Center. We will focus on AdvancedEndoscopy and Gastrointestinal Services(AEGIS), in particular, endoscopic retrogradecholangio pancreatography (ERCP),endoscopic ultrasound (EUS), Spyglass andother technologies.ADVANCED ENDOSCOPY 4PATIENT TESTIMONIALS 6DHC UPDATE & HIGHLIGHTS 8ABOUT THE COVERAdvanced Endoscopy suite with state-ofthe-art equipment at DHC. Insert shows anERCP image. Read more on page 4.Digestive Matters, Winter 2015MEET OUR TEAM 10GRATEFUL PATIENT GIVES BACK 123
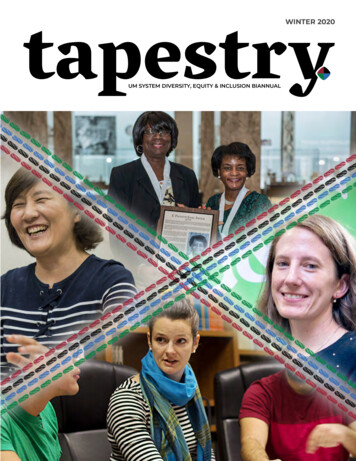
ADVANCED ENDOSCOPY:MINIMALLY INVASIVE ALTERNATIVES FOR GASTROINTESTINAL PROBLEMSIf you’re suffering from a digestive health disorder, consider a gentler option for treatment. The Advanced Endoscopy &Gastrointestinal Service (AEGIS) at the Georgia Regents Digestive Health Center offers a wide range of highly advanced,minimally invasive alternatives to standard invasive diagnostic and surgical procedures. Our multidisciplinary advancedendoscopy team has more than 50 years’ experience in diagnosing and caring for:General disorders affecting the esophagus,stomach and duodenum, and colon and rectum Management of large complicated polyps, or abnormal tissue growth Diagnosis and treatment of fistula, abnormal connection between vessels or intestinesdue to infection or inflammation Diagnosis of cancer, or lymphadenopathy, swollen or enlarged lymph nodes outsidethe gut wall either in the chest or inside the abdomenSpecific esophageal disorders Barrett’s esophagus, a complication of gastroesophageal reflux disease (GERD) thatcan causedysplasia, or abnormal cell changes, and increase risk of cancer Perforation, a hole in the esophagus caused by injury Submucosal mass, a tumor in the submucosa layer of the lining of the esophagus ordigestive tractDr. SridharPancreas and bile duct disorders Stones in the bile duct (choledocholithiasis) or gallbladder (cholelithiasis) Infection of the bile duct (cholangitis) Cancer of the bile duct or gallbladder Inflammation of the pancreas (acute or chronic pancreatitis) Cyst in the pancreas or bile duct (choledochocele) Mass in the pancreas or in the ampulla of Vater, an area where the bile duct andpancreatic duct join Bile duct muscle dysfunction (Sphincter of Oddi dysfunction), causing abdominal painTake the QuizWhich of the statements below is trueabout the further management of thispatient?An 18 year-old was seen in the ERwith food impaction after eating steak.He describes mid-chest discomfort andpooling salivary secretions. He has ahistory of severe allergic rhinosinusitis.The meat bolus was disimpactedsuccessfully with an endoscopy whichalso revealed the following findings:A. Treatment with antihistaminesimproves this dysphagia.Seigfried Yu, MDEndoscopy Exam RoomB. Botulinum toxin injection isconsidered first-line therapy.C. If the patient does not respond toPPI therapy, an Anti-TNF biologicagent would be indicated.D. A course of PPI bid with singulair isusually first line of treatment.E. Esophageal dilation iscontraindicated.ANSWER:D. The picture depicts distinct rings,consistent with eosinophilic esophagitis(EoE). Esophageal dilation is safe inmost patients with EoE to addressdominant strictures.4Ultrasound image
Technologically Advanced CareSharper images in real time. Greaterdetail. 3-D imaging. GRHealth’s ongoingpartnership with Philips, a worldwideleader in health care electronics, meansthat we have the most advancedtechnology available today at ourfingertips, allowing us to deliver bettercare and the latest minimally invasivetreatments to you and your family.Our procedures include: Bariatric endoscopy, endoscopicmanagement of complications afterweight-loss surgery Complex polypectomy, removal ofpolyps or small growths found during acolonoscopy Deep/device-assisted enteroscopy orsmall bowel endoscopy, which looksdeep inside the small intestine todiagnose digestive disorders Endoscopic ablation therapy (HALO),a nonsurgical procedure for Barrett’sesophagus that uses a special catheterand heat to remove diseased orprecancerous tissue in the esophagus Endoscopic celiac plexus block/neurolysis. These nerve block injectionshelp reduce often intense, hard-totreat pain in patients with pancreaticcancer or chronic pancreatitisDigestive Matters, Winter 2015 Endoscopic mucosal resection (EMR), nonsurgical removal of cancerous or otherabnormal tissues from the digestive tract for patients with Barrett’s esophagus Endoscopic therapy for Barrett’s esophagus, including EMR, endoscopic mucosectomy(removal of the mucosal layer), and radiofrequency ablation Endoscopic ultrasound (EUS). This procedure allows physicians to examine the liningand walls of the upper and lower gastrointestinal tract using a tube with an ultrasoundcomponent. EUS is commonly used to evaluate and drain cysts, stage and manage cancer,and evaluate and perform fine needle aspiration of masses and/or lymph nodes Endoscopic retrograde cholangiopancreatography (ERCP). This procedure allowsphysicians to examine pancreatic and bile ducts using contrast material and fluoroscopy(X-ray). ERCP is commonly used for stent placement, stone removal and fracture(lithotripsy), stricture dilation (opening narrowed areas), and tumor sampling andmanagement Enteral stent placement. Stents, hollow mesh tubes, may be placed in the digestive tractto correct narrowed areas caused by disease or illness Enteral tube/feeding tube placement and venting gastrostomy. During this procedure, anendoscope is inserted through the mouth and into the stomach for the placement of afeeding tube. MEET OUR ADVANCED ENDOSCOPY TEAMDr. John Affronti,Advanced Endoscopy, Biliary/Pancreas and Director, AEGISDr. Sumanth Daram,Advanced Endoscopy, Biliary/PancreasDr. Subbaramiah Sridhar,Advanced Endoscopy, Biliary/PancreasAmanda Lee ARNP,Nurse Practitioner5
PATIENT TESTIMONIALSAllen Rowe, Spyglass Direct Visualization SystemFor Allen Rowe, 81, his case beganwith something simple: He thoughthe had the flu. But his doctor thoughtotherwise: “He said, ‘I think you havegallstones.’”Tests confirmed not only stones buta stricture in the bile duct that requiredstents—and possible gallbladder removal.Then the word “cancer” was mentioned, andRowe was referred to Dr. Sumanth Daramand GRHealth Digestive Health Center,which offers the area’s only endoscopicultrasound, for further testing.After part of his gallbladder was removed,Rowe continued to be followed by Dr. Daram,an interventional gastroenterologist andspecialist in biliary/pancreas, to manage hisgallbladder and assess for possible cancer.He received endoscopic ultrasounds, tissuebiopsies and stent replacements every two tofour months over the course of three years.6“When I first met Dr. Daram and the rest of the staff atthe GRHealth Digestive Health Center, I felt immediatelycomfortable. I was confident in the people I talked to, thatthey knew what they were doing and I was going to get takencare of. And he’s been watching me like a hawk ever since!”“After an endoscopy visit, it takes about a week to get over it,” said Rowe, who also suffers from heartarrhythmia. “It drains the heck out of me.”But then, a new technology: SpyGlass Direct Visualization System. Ideal for older patients orthose with underlying health issues, the system helps reduce the need for endoscopic ultrasound byoffering a clear and magnified view into the bile duct, viewable to the naked eye.Rowe’s SpyGlass procedure found that his bile duct was completely benign. As a result, he nowwill see Dr. Daram and the Digestive Health Center team in six months. “When I first met Dr.Daram and the rest of the staff at the GRHealth Digestive Health Center, I felt immediatelycomfortable. I was confident in the people I talked to, that they knew what they were doing and Iwas going to get taken care of,” said Rowe. “And he’s been watching me like a hawk ever since!” grhealth.org/digestivehealth
Frank Thomas, Endoscopic UltrasoundWhen Frank Thomas, 66, first sawan image of the tumor pressingon his esophagus, he wasshocked at how large it was. Especially sincehe had felt no symptoms.Thomas was lucky. A CT scan andGI series related to his heart arrhythmiauncovered the mass—and his cardiologistat GRHealth immediately referred him toDr. John Affronti, Director of AdvancedEndoscopy and Gastrointestinal Services atGRHealth Digestive Health Center.Affronti immediately used endoscopicultrasound to pinpoint the depth ofinvolvement, location and stage of the tumor,and Thomas was even luckier: The mass hadnot yet extended to the muscle layer andwas contained. As a result, the tumor boardadvised that he undergo VATS surgery,without the need for further chemotherapyor radiation.In this region, VATS or video-assistedthoracoscopic surgery is only available atGRHealth Digestive Health Center (otherfacilities offering the procedure are twoplus hours away). Offered by Dr. CarstenSchroeder, the advanced technique relieson a tiny camera and tools inserted throughseveral small incisions through the chest. Theminimally invasive procedure results in fasterrecovery, less pain, fewer complications andthe same oncologic results as open surgery.Despite a few complications, Thomas waseating ice cream in his hospital bed a weekafter surgery. “I felt great,” he remembered.“They said they got it all and that I wasn’tgoing to have to go through the radiationtreatments and chemotherapy, and all thatmade it 10 times better.”Today, Thomas is free and clear of cancerand has no need to visit the GRHealthDigestive Health Center (other thanscheduled colonoscopies, one of which hecompleted earlier this year). He’s back toworking as a radiological control inspector atSavannah River Site and just enjoying his life.“This was my first real stay in a hospitaland my first-ever surgery,” said Thomas.“I expected it to be really, really bad, but itwasn’t. It was good, and those folks—theyreally take care of you.I’m doing well andI’m back at work—and I still eat steak!” Digestive Matters, Winter 2015“This was my first real stay in a hospital and my first-eversurgery I expected it to be really, really bad, but it wasn’t. Itwas good, and those folks—they really take care of you.I’mdoing well and I’m back at work—and I still eat steak!”Frank Thomas7
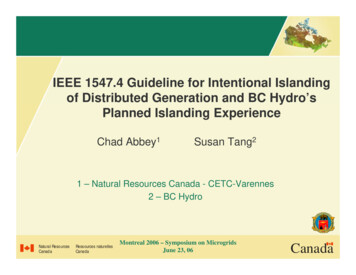
2015 ANNUAL REPORTduresescopy ProcTotal Endo4,028500450400H: 429350YEAR HIG: 2698200150JUNEMAYAPRMARFEBJANDEC50DHC offers the latest in 330 viewscope - one of the first in Georgia.A new generation ofcolonoscopes has beendeveloped, allowing for330-degree forward view.These Fuse colonoscopeshave been shown toincrease the rate ofdetection of colon polypsby 69 percent and arecurrently being used indaily practice at the DHC.250100YEAR LOWNOVOCTSEPTAUGJULYFUSE SCOPE300
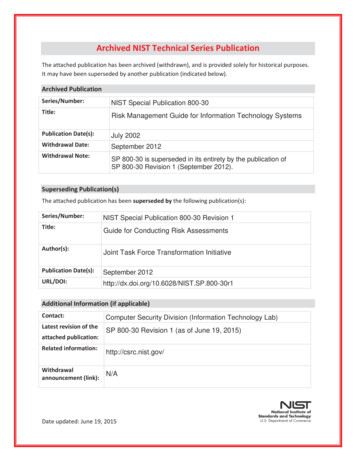
Drug development for hepatitis C has revolutionized our ability to cureand eradicate this disease. The combination of well-tolerated medications in a once daily pill, Harvoni , achieves cure rates in greater than 90percent of patients regardless of prior treatment. Unfortunately, withoutan aggressive specialty pharmacy, such as one found at DHC, access tothis medication remains limited in the community.NEWDRUGSNew Drug: HARVONI Indication: Hepatitis CNew Drug: ENTVYIO DHC CLINIC VOLUMEST R EN D IN G POS ITIV E800070006000Indication: IBD5000Finally, the new medication,Entvyio , available to our DHCpatients, offers IBD patients notresponsive to prior anti-TNFtherapy a promising treatmentoption with a completely novelmechanism of action.4000300020001000Treatment: NALOXEGOL0NEW VISITSTOTAL VISI T SFY 20132,004P R O CED UR E SFY 2014FY 20157,085NEW VISITS4,886TOTAL VISITSPROCEDURESMOTILITY PROCEDURES1473162605001000FY 20131500FY 20142000Naloxegol is a new treatment thatallows patients to continue opioidpain medication while reversingopioid induced constipation andother undesirable side effects.
MEET OUR TEAMIf you have a digestive health disorder, big or small, we can help. As part of the region’s only comprehensive digestive health center, our physiciansare specially trained and experienced in virtually every subspecialty of gastroenterology — from advanced endoscopy to hepatology to IBD andneurogastroenterology and motility.Our center director, Satish Rao, MD, is an international leader in digestive health disorders. He is past president of the AmericanNeurogastroenterology and Motility Society, a recipient of the three highest honors from the American Gastroenterological Association, and a federallyfunded investigator.Satish Rao, MDDirector, Digestive HealthCenter & Professor ofMedicine & ProgramDirectorSpecialties: Neurogastroenterology & GIMotility, Nutrition, GastroenterologyResearch: Brain-Gut Interactions, Constipation,Biofeedback Therapy, Fecal Incontinence, IBS,Gastroparesis, Dietary Fructose Intolerance, 3-DAnorectal Evaluation, Magnetic Therapy, NovelDiagnostic Tools for GI MotilitySumanth ReddyDaram, MDInterventionalGastroenterologist,Advanced Endoscopy,Associate Professor ofMedicineSpecialties: ERCP, Endoscopic Ultrasound,Gastroenterology, Digestive HealthResearch: Clinical Outcomes, Therapeutic EUS,Endoscopic Videos in Education, EUS TissueSamplingHumbertoSifuentes, MDAssistant Professorof MedicineDirector, IBD ProgramSpecialties: Crohn’s Disease, Ulcerative Colitis,Microscopic Colitis, Pouchitis, Novel Treatmentof IBD, Postoperative Crohn’s Disease,Constipation and General GastroenterologyResearch: Inflammatory Bowel Disease,Nutrition, Quality Measures, Colon CancerPreventionJohn Affronti, MDDirector of AdvancedEndoscopy, Pancreas& Bile Duct Group &Professor of MedicineSpecialties: Advanced Endoscopy,Gastroenterology, Digestive HealthResearch: Pancreas and Bile Duct Disorders,Endoscopic Ultrasound (EUS), EndoscopicRetrograde Cholangiopancreatography (ERCP)Advanced Endoscopy Technology, EndoscopyTraining, Quality and Clinical Outcome MetricsThomas Kiernan, MDEmeritus ProfessorHepatologyGastroenterologySpecialties: HepatologyResearch: Hepatitis CSubbaramiah Sridhar, MDSandeep Khurana, MDDirector, Hepatology andAssociate Professor ofMedicineSpecialties: Hepatology, Gastroenterology,Digestive HealthResearch: Cholinergic Mechanisms of LiverInjury, Portal Hypertension, Hepatitis CNon-Alcoholic Fatty Liver DiseaseBrian Francis Lane, MDAssociate Professor ofSurgerySpecialties: Bariatric, Weight Loss, BariatricSurgery, Minimally Invasive and DigestiveDisease Surgery, General Surgery,Research: Mechanisms of Diabetes and NASHImprovement after Bariatric Surgery, RevisionBariatric Surgery, Total Endoscopic Approachesto Bariatric Surgery, the Application of MIS toComplex Gastrointestinal ProceduresProfessor of Medicine& Associate Director,GastroenterologyFellowship ProgramAdvanced &Interventional EndoscopyPancreas & Biliary GroupSpecialties: ERCP, Endoscopic Ultrasound, andAdvanced EndoscopyResearch: Translational Research, IschemicColitis, Interventions in GastrointestinalBleeding, Clinical Trials, and Clinical OutcomesSean Michael Lee, MDAssistant Professorof SurgerySpecialties: Minimally Invasive and DigestiveDisease Surgery, Bariatric Surgery, Weight Loss,General SurgeryResearch: Clinical Outcomes of BariatricSurgery, Metabolic Effects of Bariatric SurgeryOur team is pioneering and conducting cutting-edge research in many areas to uncover new solutions forchallenging diseases and to improve digestive health so that we practice tomorrow’s medicine today. Some ofour current and upcoming clinical trials include: Advanced Endoscopy, Colon, Hepatology Inflammatory BowelDisease,Motility and Neurogastroenterology. For more information, contact Amanda Schmeltz at 706-721-196810or Meagan Gibbs at 706-721-1968.
NEW FACULTYWe are pleased to announce that Dr. Alan Herline has joined our Digestive Health Center team as our first boardcertified Colon and Rectal Surgeon. In addition to his clinical responsibilties, he is the Harrison Distinguished Chair ofSurgery, Vice Chair of Surgery, Associate Director, Digestive Health Center and Section Chief of Minimally InvasiveDigestive Disease Surgery.Previously he was an Associate Professor of Surgery and Biomedical Engineering at Vanderbilt Univerity and led theColon and Rectal program from its creation to being the busiest surgical program at Vanderbilt as well as the fastestgrowing and most accomplished Colon and Rectal program in Tennessee.Dr. Herline is an Engineering graduate from Vanderbilt Univerity and received his medical degree from the MedicalCollege of Georgia in 1994. He completed his Residency in Surgery at Vanderbilt, and specialized in Colon and RectalSurgery at the Lahey Clinic. He then returned to Vanderbilt to create the Colon and Rectal program.Clinical InterestsDr. Herline is a member of the American Society of Colon and Rectal Surgeons and the New England Colon andRectal Society. He is a board-certified specialist in the surgical care of disease affecting the colon and the rectum. Dr.Herline is accomplished in minimally invasive procedures, robotic and trans-anal procedures. Dr. Herline’s primarysurgical interest is in all aspects of colon, rectal disease and treatment, colorectal cancer, inflammatory bowel disease,perianal Crohn’s disease, transrectal ultrasound, and laparoscopic surgical approaches.Dr. Alan HerlineVice Chair, J. Harold HarrisonDistinguished Chair of Surgery,Section Chief of MIDDS,Associate Director,Digestive Health CenterResearch InterestsIn addition to his clinical practice, Dr. Herline has active, funded research projects that combine his engineering and clinical expertise. He speaksnationally, is well published and continues to develop intellectual property in surgical applications.Dr. Herline is excited about his return to his alma mater, Medical College of Georgia, and looks forward to advancing colon and rectal care in Augusta,the state of Georgia and regionally.We are pleased to announce that Dr. Sharma has joined the Georgia Regents University Department of Medicineas assistant professor in the Section of Neurogastroenterology and GI Motility. He was a resident in internalmedicine at Temple University Hospitals in Philadelphia, PA, and a fellow in the Division of Gastroenterology andHepatology at Penn State Milton S. Hershey Medical Center where he was the chief fellow. He has been recruitedto further the Neurogastroenterology/Motility Program at Georgia Regents Health System. Dr. Sharma is boardcertified in internal medicine.Clinical InterestsDr. Sharma has particular interest in neurogastroenterology & GI motility. During his training, he researched foregutmotility disorders and was recognized for his work by the American Neurogastroenterology & Motility Society asa Young Investigator. He looks forward to meeting the challenging needs of our patients in a patient-centered andmultidisciplinary manner with the expertise and resources available at the Georgia Regents Digestive Health Center.Dr. Amol SharmaAssistant Professor of MedicineNeurogastroenterology/MotilityResearch InterestsDr. Sharma’s research experience includes achalsia, non-obstructive dysphagia, gastoparesis, IBS, chronic constipationand fecal incontinence.GRHealth officially cut theribbon on their new stateof-the-art Digestive HealthCenter April 2015.Digestive Matters, Winter 2015Pictured: Dr. Satish Raowith wife Sheila Rao,Jenny Montgomery,Dr. Peter Buckley with wife11Leone Buckley.
Non-ProfitOrganizationU.S. PostageCommunications and Marketing1120 15th Street, TR-101Augusta, Georgia 30912PAIDAugusta, GAPermit No. 210CHANGE SERVICE REQUESTEDWrong address?Need to update your information?Tell us by email at updateinfo@gru.eduGo online to gru.edu/updateinfoOr call us at 706-721-4001GRATEFUL PATIENT GIVES BACKFor Laura Whitty, it has been a long and winding road from Louisville, Kentucky toAugusta, Georgia. Include pain, frustration and fear in that journey. She has suffered fromgastrointestinal issues since her teenage years much like her mother and grandmother. Shesaw several different physicians in Louisville, Cleveland and Indianapolis, none of whom offeredanything more than vague diagnosis of “irritable bowel syndrome”. At each stop, doctors ran thesame tests, offered the same prescriptions and got the same results-no relief. Finally, Dr. John Woorecommended that she travel to Georgia to see Dr. Satish Rao. By the time she arrived for her initialvisit, her weight had dropped from 130lbs to 98lbs. Her husband began to doubt that she wouldsurvive. That was almost three years ago.Dr. Rao had Laura tested completely differently from previous physicians and was, at last, ableto pinpoint her problem-extreme intolerance to high fructose corn syrup as well as dyssynergicconstipation. With careful adherence to diet and ? and treatment, Laura is well on her way to fullrecovery. She has regained her normal weight and has returned to her passion of gardening, chasinggrandchildren and enjoying life in general. While still fighting to overcome lingering issues, Dr. Raohas truly given her a bright future, for which she will be eternally grateful. Laura WhittyWe hope you will consider supporting our endeavors, so that we can provide the best care for our patientsand keep our department on the cutting edge. To learn more about how you can make a gift, please contactDavid Cantrell at 706-721-1817 or dcantrell@gru.edu.
f you’re suffering from a digestive health disorder, consider a gentler option for treatment. The Advanced Endoscopy & Gastrointestinal Service (AEGIS) at the Georgia Regents Digestive Health Center offers a wide range of highly advanced, minimally invasive alternatives