Transcription
HoneywellHuman Factors DesignGuidelines for the Elderlyand People with DisabilitiesRevison 3—DraftMay 1992Honeywell SSDC3660 Technology DriveMinneapolis, MN 55418SSDC-SYS/AI-C92-009C920317
HoneywellHuman Factors Design Guidelines for theElderly and People with DisabilitiesRevision 3 DraftPrepared by:Sandra DennoBrian A. IsleGinny JuChristopher G. KochStephen V. MetzRobin PennerLi WangJohn WardMay 1992Permisssion is granted to reproduce anddistribute this document as long as it is notfor profit. For more information, write:Brian IsleMN65-2300Honeywell Inc.3660 Technology DriveMinneapolis, Minnesota 55418SSDC-SYS/AI-C92-009 Copyright 1992, Brian Isle, Sandra Denno, Stephen V. MetzC920317
Table of ContentsSectioniPage1Introduction and Scope .Background .Needs of a Special Population .Human Factors Issues .The Role of Design Guidelines .Topics for Human Factors Design Guidelines .1-11-11-11-21-31-32Population Served .Categories of Functional Disabilities .Physical Impairment .Perceptual Impairment .Cognitive Impairment .Disabling Conditions .Aging .Age-Related Effects on Hearing .Arthritis .Multiple Sclerosis .Cerebral Palsy .Stroke and Head Trauma .Spinal Cord Injury trols .Finger-Operated Pushbutton .Palm-Activated Pushbutton .Push-Pull Controls .Membrane Touch Keys—Pushbuttons .Keypad Keys .Toggle Switches .Rocker Switches .Slide Switches .Detented Rotary Selectors .Continuous Rotary Controls .3-13-13-13-23-23-33-33-43-43-53-54Visual Displays .Alphanumeric Text Displays .Light Indicators .Labels .Color . 4-2Emergency Indicators .4-14-14-24-24-2
Table of Contents (concluded)SectioniiPage5Auditory Displays .Informational Auditory Displays (tone or beep) .Informational Auditory Displays (synthesized speech) .Emergency Auditory Warnings .5-15-15-15-26Functional Allocation and Panel Layout .Functional Allocation .Principles of Arrangement .Panel Layout .Keypads .Panel Design—Continuous Controls .6-16-16-16-16-16-17Operating Protocol .Matrix of Categories of Functional Disabilities vs. Design Principles .Functional Performance Specifications (details TBD) .7-17-17-1Appendix A Types of Grips .A-1References .R-1
List of FiguresFigure Page2-1Hand Grip and Lateral Pinch Strength for Subjects with Various DisablingConditions .2-32-2Change of Hand Grip Strength with Age .2-42-3Percent Loss of Hand Grip Strength with Age .2-42-4Change of Lateral Pinch Grip Strength with Age .2-52-5Percent Loss of Lateral Pinch with Age .2-52-6Change of Tip Pinch Grip Strength with Age .2-62-7Percent Loss of Palmar Pinch with Age .2-62-8Change of Palmar Pinch Strength with Age .2-72-9Percent Loss of Tip Pinch Grip with Age .2-72-10Changes in Visual Accommodation with Age .2-82-11Changes in Visual Acuity Measured in Snellen Index with Age .2-92-12Changes with Age in Pupillary Diameter and Area, Measured in LightAdapted and Dark-Adapted Individuals .2-9Decline in Light Sensitivity with Age; Data Show Changes in VisualThreshold After Dark Adaptation in Different Age Groups .2-102-14Decade Audiogram Illustrating the Audiometric Patterns of Normal Aging .2-122-15Percentage Hearing Loss by Age and Frequency .2-133-1Torque Applied to Rotary Control by Subjects with Arthritis andControl Groups .3-62-13iii
AcknowledgmentsThe authors would like to acknowledge the various groups who have supported and encouragedthe project since its inception: The Honeywell Foundation; The Southeastern Minnesota Center for Independent Living; Rachel Wobschall, Executive Director of the Minnesota STAR Program; The management at Honeywell SSDC.vii
Section 1Introduction and ScopeIndividuals with physical, sensory, or cognitive disabilities have special needs for interactingwith their environment. Effective design of controls and displays in the residence and workplaceused by individuals with disabilities is critical for maximizing their abilities; in reality, however,the design of these devices often fails to account for their special needs.People with disabilities are accustomed to accommodating to their environment or inventingways around it. They need devices that either require only their abilities or can be modified.With good planning, most devices can be designed for use by individuals with limited abilities.BackgroundThis document reflects the work of a group of engineers and designers who are studying theneeds of the elderly and people with disabilities and designing solutions. Their activities includeextensive literature review, analysis of population demographics, interviews with individualswith disability, and controlled research.The group’s shared vision is the availability of a wide variety of affordable controls and productsfor the home and work environment that are usable or adaptable for all people, including theelderly and those with disabilities.The problem is defined below: All individuals need affordable access to controls, tools, communication devices,and other equipment and components in the home and work environments tointeract effectively with their world. Manufacturers often do not understand the special needs of the elderly or thosewith disabilities. Currently, highly specialized devices have low volume and high cost.Needs of a Special PopulationThere are three principal categories of disabilities: Physical/motor limitations that impair an individual’s ability to reach andmanipulate controls;1-1
Sensory limitations that impair an individual’s ability to receive information andfeedback; Cognitive limitations that impair an individual’s ability to process information.There are unique challenges to the engineering and design of controls and displays for peoplewith disabilities. Those with physical limitations need a usable control device in an accessiblelocation. For this group, conventional displays and feedback mechanisms may be satisfactory.For people with sensory limitations, adequate displays and feedback from devices are needed.Individuals with cognitive disabilities can use most well-designed controls and displays but takelonger to learn to use them and need error protection.Human Factors IssuesHuman factors engineering is the study and practice of designing equipment, machines, andenvironments to accommodate human users. Human factors encompasses physical requirementsof size and force as well as mathematical models of human information processing and control.Issues of operability and consistency affect design for special populations. Operability involvesthe amount of effort required to use a component or device. The accessibility of controls, thereadability of displays, and the logical sequence of actions required to produce any desired resultare all operability issues. For example, a control panel is poorly designed if it is too high for aperson in a wheelchair to reach, requires too much force on the keys for a person with limitedstrength, or requires memorization of a complex sequence of control inputs. Even if allcomponents and devices within a residence are easy and convenient to operate, confusion maystill result from the differences in the way similar functions are controlled in differentcomponents and devices. For instance, a variety of procedures exists for storing numbers in thememory dialers of telephones currently on the market. Learning the procedures for one productmay not help in learning the procedures for another, and in fact, may even inhibit such learning.There are several general human factors design goals that address operability and consistency incontrols/displays design and operation: Use a minimized set of unique controls or keys and avoid the use of the samecontrols or keys for different functions. Reduce the number of potential operating parameters while providing powerfulfunctionality. For example, use the fewest and simplest set of steps necessary toaccomplish a function and avoid unnecessary options. Design operating procedures to be fault tolerant. For example, allow entry of asequence of inputs in any order. Strive for standard operating procedures across dissimilar devices to promoteconsistency.1-2
The Role of Design GuidelinesOur premise is that devices can be made user friendly for the elderly and those with disabilitiesby applying good human factors design principles and limiting the set of unique abilitiesrequired to use an interface. Furthermore, equipment design that is consistent with this premise isalso effective and often preferable for people without disabilities.The purpose of this document is to provide a preliminary set of appropriate design guidelines forcomponents and devices found in the home and workplace that can accommodate the abilities ofthe elderly and individuals with disabilities as well as enhance the usability of products. Theguidelines are intended to ensure that the products designed, selected, and built by variousmanufacturers (who voluntarily choose to apply the guidelines) will be safe, convenient, andeasy to use. The human factors guidelines are not intended to establish specific and inflexiblestandards for device design; rather, to promote good design practice, and allow a variety ofeffective solutions to each design requirement.Many of the values identified in this document for parameters such as size, force, coding, andtonal amplitude are derived from published standards, textbooks, or other human factorsguidelines. These sources are listed in the References section. Although exceptions may beencountered for some design problems, the use of the word “should” indicates generalapplicability of the guideline item; the word “preferred” indicates a recommendation.Topics for Human Factors Design GuidelinesThe scope of the human factors guidelines for component and device design includes thefollowing topics: ted pushbuttonPalm-operated pushbuttonPush-pull controlsMembrane touch keys—pushbuttonsKeypad keys—pushbuttonsToggle switchesRocker switchesSlide switchesDetented rotary selectorsContinuous rotary controls Visual displays– Alphanumeric text displays– Light indicators– Labels1-3
–––––––ColorUse of color in displaysUse of color in organization and labelingColor specificationSize of colored areaColor namingEmergency indicators Graphics––––SymbolsCreating or building new symbolsGraphics symbols for SMART HOUSE useAdditional illustrations Auditory displays– Informational auditory displays (tone or beep)– Informational auditory displays (synthesized speech)– Emergency auditory warnings Functional allocation and panel layout–––––Functional allocationPrinciples of arrangementPanel layoutKeypadsPanel design—continuous controls Operating protocol––––––––1-4Remote accessResponse timeComputer-based interface guidelinesInteraction stylesDesign of operating proceduresEmergency proceduresHelp featuresTerminology
Section 2Population ServedCategories of Functional DisabilitiesThe human factors guidelines address a wide variety of impairments subdivided under the threeprincipal categories of functional limitations:Physical Impairment Physical impairments– Extreme muscle weakness or reduced endurance– Paralysis—loss of sensation or voluntary movement– Paraplegia—paralysis of both legs and the lower portion of the trunk– Quadriplegia—partial or total paralysis of all four extremities, usually frominjury to the spinal cord at the sixth cervical vertebra or higher– Limited hand/arm reach capability, sometimes due to wheelchair positioning– Impairment of dexterity/manipulative skills– Tremor—continuous, involuntary quivering– Contracture—permanent contraction of a muscle– Spasticity—stiff, awkward movements due to involuntary muscle contractions– Ataxia—impaired muscle coordination, especially when voluntary musclecontrol is attempted– Apraxia—inability to perform voluntary movements although there is nosensory or motor impairment– Rigidity—immovability– Use of braces and other prosthetics– Extremes of size or maturity Speech impairments– Dysarthria—slurred speech due to impairment of the tongue or other musclesessential to speech– Stuttering– Aphasia—impairment of ability to communicate through speech, writing, orsigns– Complete loss of speech2-1
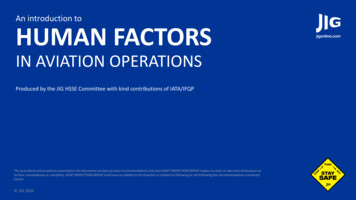
Perceptual Impairment Hearing impairments– Partial hearing loss– Complete hearing loss– Listening impairment Vision impairments––––Legal blindnessColor blindnessComplete blindnessDiplopia—double visionCognitive Impairment Cognitive ility to interpret written languageConfusion or disorientationLoss of short-term memoryLoss of long-term memoryImpairment of learning and retentionImpairment of perception and attentionImpairment of intelligence and thinkingSevere mental retardationDisabling ConditionsThe functional limitations listed above are caused by a wide variety of disabling conditionsincluding diseases, accidents, aging and birth defects. The following are some of the morefrequently occuring conditions: Aging,Arthritis,Multiple sclerosis,Cerebral palsy,Stroke and head trauma,Spinal cord injury.Limited strength is common to nearly all disabling conditions and is a common reason for beingunable to operate household equipment. Figure 2-1 shows the hand functions (hand grip andlateral pinch) of the elderly and people with rheumatoid arthritis, multiple sclerosis, and spinalcord injuries (levels C4–C7). In this figure, the hand functions for the four groups are normalizedas the percentages of normal strength. The data for individuals with spinal cord injury are afterany surgical procedures (such as tendon transfers).2-2
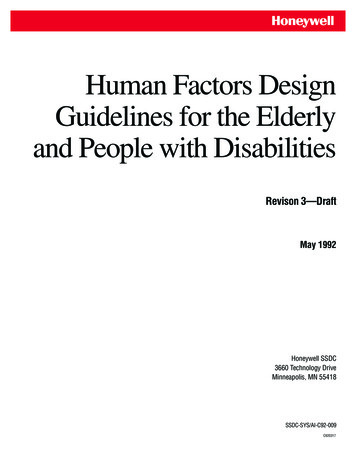
% of Hand Grip and Lateral Pinch GripStrength with Respect to Normal100% of 055–5960–6465–6970–74No DisabilityHand Grip75 RAMSDisabilitySCILateral Pinch GripC920317-01Adapted from Stover (1986), Tourtellotte (1965), Helliwell (1987), and Mathiowetz (1985)Figure 2-1. Hand Grip and Lateral Pinch Strength for Subjects with Various Disabling Conditions(Rheumatoid Arthritis (RA), Multiple Sclerosis (MS), Spinal Cord Injury (SCI))AgingThe aging process often leads to vision loss, hearing loss, and osteoarthritis, as well as loss ofstrength.Age-Related Effects on Hand Strength—It is well documented that muscle strength declineswith increasing age for all muscle groups. Here, only the change of hand strength with respect toage will be presented (Mathiowetz, 1985). The actual strengths and percentage losses, as ageincreases, of hand grip, lateral pinch, tip pinch strength and palmar pinch are illustrated in thefollowing eight figures. The data were gathered from a sample of 310 males and 328 females,ages 20 to 94 years old. The percentage loss is calculated based on the data at the age of 20 to24. Figures 2-2 to 2-9 show that in most cases the peak of hand strength occurs between 30 and40 years of age, and no more than 10% decline in strength occurs before age 50 or 55.Age-Related Effects on Visual Functions—Like other parts of the body, the eyes undergo manychanges due to aging. The lens becomes yellowed, thickened, and less elastic, which causesreduced accommodative capacity, reduced light entering the eye, and the scattering of light raysbefore they reach the retina. Changes in the cornea also lead to increased scattering of light rays.The iris dilator atrophies and becomes more rigid, which reduces the size of the pupil and itsability to adjust its size according to the amount of light available. The reduction in the size ofthe pupil is known as senile miosis. In addition, there may be deterioration in the visualpathways of the central nervous system (Whitbourne, 1985). These changes in the physicalstructure of the eye affect several aspects of visual function, including refractive power,accommodation, acuity, dark adaptation, sensitivity to light, color vision, temporal resolution,depth perception, and visual field.2-3
60MenWomenForce 70–7425–2935–3945–4955–5965–6975 Age (Years)C920317-02Figure 2-2. Change of Hand Grip Strength with Age120Men110WomenPercent ��6470–7425–2935–3945–4955–5965–6975 Age (years)2-4C920317-04
Figure 2-3. Percent Loss of Hand Grip Strength with Age16Men14WomenForce –7425–2935–3945–4955–5965–6975 Age (Years)C920317-03Figure 2-4. Change of Lateral Pinch Grip Strength with Age2-5
120MenWomen110Percent 70–7425–2935–3945–4955–5965–6975 Age (years)C920317-05Figure 2-5. Percent Loss of Lateral Pinch with Age16Men14WomenForce –7425–2935–3945–4955–5965–6975 Age (years)C920317-07Figure 2-6. Change of Tip Pinch Grip Strength with Age2-6
120MenWomen110Perce nt 70–7425–2935–3945–4955–5965–6975 Age (years)C92031 7-09Figure 2-7. Percent Loss of Palmar Pinch with Age16Men14WomenForce –7425–2935–3945–4955–5965–6975 Age (years)C920317-06Figure 2-8. Change of Palmar Pinch Strength with Age2-7
120MenWomen110Percent 70–7425–2935–3945–4955–5965–6975 Age (years)C920317-08Figure 2-9. Percent Loss of Tip Pinch Grip with AgeRefractive Power—From about age 30 to the mid-60s, the eye gradually becomes morehypermetropic (farsighted) as the lens flattens. After the mid-60s, this reverses and the eyebecomes more myopic (nearsighted) (Whitbourne, 1985). Roughly one-third of individuals overage 80 have vision of 20/50 or less (Lewis, 1985).Accommodation—Adaption is the eye’s ability to change its focus from far to near objects.The change in the refractive power of the lens in shifting focus from far to near objects becomesreduced from a peak of 14 diopters at 8 years to less than 2 diopters at age 50. By the age of 60,the lens is completely incapable of accommodating to focus on objects at close distance(Whitbourne, 1985). This is known as presbyopia (Figure 2-10).2-8
5455565C920317-10Source: Tuniras (1988)Figure 2-10. Changes in Visual Accommodation with AgeThe reduced elasticity of the lens with age makes the lens less able to accommodate for nearvision. The minimum distance between an object and the eye for a clear image, the “near point,”increases from 9 cm at 10 years to 10 cm at 20 years, 20 cm at 45 years, 84 cm at 60 years(Tuniras, 1988), and 100 cm by age 70 (Kenney, 1989).Acuity—Visual acuity is the ability to detect details on objects at varying distances. Scatter inthe cornea and lens serves to deflect light rays entering the eye and reduce the contrast necessaryfor detecting details (Tuniras, 1988; Whitbourne, 1985). Senile miosis, the decrease in pupil size,reduces the amount of light entering the eye by as much as one-third (Kenney, 1989; Tuniras,1988) and therefore also reduces the ability to detect details (Tuniras, 1988; Whitbourne, 1985).Visual acuity increases during the 20s–30s and remains stable for 10–20 years. It begins todecrease in the 40s, and by age 85, there is an 80% loss of acuity when compared to the acuity atage 40 (Figure 2-11). The loss of acuity is especially severe at low levels of illumination(Whitbourne, 1985) (Figure 2-11).Elimination of glare and improved illumination can help enhance visual acuity substantially inthe aged population (Tuniras, 1988).2-9
Visual rce: Pitts (1982)Figure 2-11. Changes in Visual Acuity Measured in Snellen Index with AgeDark Adaptation—Dark adaptation occurs when moving from a bright light to a dimenvironment. Decreased dark adaptation begins in the 20s and is especially pronounced after age60. This appears to be caused by reduced light transmission through the lens and the reduction inpupil size or senile miosis (Whitbourne, 1985). In a fully dark-adapted eye, the mean diameter ofthe pupil is 8 mm in the 20s and gradually decreases to a mean of 5 mm in the 90s (Tuniras,1988) (Figure 2-12).Age-Related Effects on Visual Functions85030205410Light-Adapted352Pupillary Diameter (mm)Dark-Adapted6Pupillary Area (mm )4072111020304050Age (years)607080C920317-12Source: Tuniras (1988); original data from Verriest (1971)Figure 2-12.2-10Changes with Age in Pupillary Diameter and Area, Measured in Light-Adapted
and Dark-Adapted IndividualsSensitivity to Light—Older adults are less able to detect low levels of light because theyellowing and increased density of the lens, as well as senile miosis, reduces the amount of lightthat enters the eye (Whitbourne, 1985) (Figure 2-13). Therefore, the minimum amount of lightnecessary to see an object increases with age (Tuniras, 1988). Glare may also increase and createvisual difficulties (Whitbourne, 1985).8Threshold Intensity (Log 10 µµl)7658046040203210203040Time (minutes in darkness)C920317-13Source: Tuniras (1988); original data from McFarland (1960)Figure 2-13.Decline in Light Sensitivity with Age; Data Show Changes in Visual ThresholdAfter Dark Adaptation in Different Age GroupsColor Vision—In the 40s and 50s, color perception begins to decline and there is reduced abilityto discriminate between colors at the green-blue-violet end of the spectrum. This is due to thethickening and yellowing of the lens with age and is further affected by senile miosis, whichrestricts light entry to the thickest and most yellow central region of the lens (Tuniras, 1988;Whitbourne, 1985).Temporal Resolution—The critical fusion frequency is the least frequency of a flashing lightthat is perceived as an uninterrupted signal. This is also referred to as the critical flicker fusion.With increasing age, there is a decrease in the point at which a flickering stimulus fuses into acontinuous light. This is due to changes in the lens that reduce the amount of light entering theeye as well as aging effects in the central nervous system (Whitbourne, 1985).2-11
Depth Perception—Depth perception appears to remain unchanged through the mid-40s, butsome changes occur in later life (Whitbourne, 1985).Visual Field—The size of the visual field is reduced significantly due to loss of receptors, aswell as other factors (Kenney, 1989).Age-Related Effects on HearingHearing impairment is the third most prevalent chronic condition among the elderly population.About half of the population of hearing-impaired people is over 65. The prevalence of hearingimpairment is about 12% of all people between ages 45 and 64, about 24% of those between 65and 74, and about 39% of those age 75 and over (Schow, 1980). In nursing homes, theprevalence of hearing impairment is much higher than in the general population, ranging from 51to 97% (Schow, 1980).Hearing loss is classified as conductive, sensorineural, or mixed (Meyerhoff, 1984). Aconductive hearing loss is due to a malfunction in the gathering of sound by the external ear,secondary to obstruction of the external auditory canal, or incomplete or inefficient transfer ofsound energy to the cochlea by the eardrum or the ossicles of the middle ear. Sensorineuralhearing loss may be caused by a lesion of the sensory receptor elements in the cochlea or theauditory nerve or a lesion of the higher processing center. Mixed hearing losses are those thathave elements of both disorders (Meyerhoff, 1984).Presbycusis—The most common cause of sensorineural hearing loss is presbycusis, the gradualreduction in hearing loss with advancing age (Staloff, 1987). It has been shown that hearing lossincreases with age and is generally greater in the higher frequencies (Goldstein, 1984; Maurer,1979). The severity of loss is greater for men than women (Maurer, 1979). Studies have alsoshown that the elderly can have greater speech discrimination impairment than young adults,although hearing ability is the same for both groups (Kirikae, 1964). Most elements or phonemesof speech fall within the frequency range of 300 to 4000 Hz.Presbycusis is the most common communicative problem among the aging. It also is the mostcommon auditory disorder in the entire population (Mader, 1984). There are four specific classesof presbycusis, and they have different characteristics in hearing loss (Corso, 1984). Sensorypresbycusis produces a high-frequency loss (above 8000 Hz); neural presbycusis affects speechdiscrimination without a parallel loss in pure tone thresholds; metabolic presbycusis has a nearlyuniform threshold loss for all frequencies with loudness recruitment; mechanical presbycusisshows an increase in hearing loss values from low to high frequencies. The most common formis sensorineural presbycusis (Sataloff, 1987).Hearing Thresholds—Hearing tests are usually performed in the frequency range of 500 to 4000Hz (1000 to 2000 Hz in some cases) (Goldstein,1984), since this range is an estimate of theperson’s overall functional hearing sensitivity (Schow, 1980). The level of hearing impairmentthat is considered significant varies from different surveys and research projects and is still beingdebated.2-12
The level of impair
Human Factors Issues Human factors engineering is the study and practice of designing equipment, machines, and environments to accommodate human users. Human factors encompasses physical requirements of size and force as well as mathematical models of