Transcription
ROOTCAUSEANALYSISA Summary of Root Cause Analysis and its use in StateDevelopmental Disabilities AgenciesRecommended Procedures for the Review of Sentinel Events and forIdentifying Systems Factors that Require ImprovementPrepared by Steven D. Staugaitis, Ph.d.March 2002developed by:Human ServicesResearch Instituteunder subcontract to:The MEDSTAT Group, Incfor the:Centers for Medicareand Medicaid ServicesCMS Contract No. 500-96-006, Task Order No. 21
PrefaceRoot Cause Analysis represents a structured approach to the investigation andanalysis of significant adverse events or system deficiencies and require improvement.This introduction to root cause analysis, and its adaptation to developmental disabilitiessystems, has been commissioned by the Human Services Research Institute (HSRI) in aneffort to assist state DD program administrators enhance their risk management andquality improvement activities. It is designed to provide guidance on the use of rootcause analysis to individuals charged with managing programs and larger systems thatserve and support persons with developmental disabilities. It includes information andtools that can be incorporated into existing or planned risk management and qualityimprovement procedures in order to:1. PREVENT the future occurrence of adverse events that do or can cause harm toindividuals; and,2. CORRECT practices that have led to regulatory noncompliance, includingidentified deficiencies noted by regulatory agencies such as CMS.Readers interested in applying root cause analysis to specific incidents or adverse eventsin order to minimize future risk should carefully review Chapter 2: Root Cause Analysisand Risk Management. They should also review Chapter 5: Tools and Techniqueswhere they will find a number of different group exercises and forms that can be directlycopied or adapted for use by the RCA Team.Readers only interested in applying root cause analysis to a system failure, such as thatidentified by a regulatory agency (i.e., citation or deficiency), should focus their reviewon Chapter 3: Adapting RCA to the Evaluation of DD System Deficiencies.As noted, this overview represents an introduction to the use of root cause analysisspecifically adapted to address some of the unique issues and concerns present in supportand service systems that assist people with mental retardation and other developmentaldisabilities. There is substantial literature available for review that addresses the use ofroot cause analysis in engineering, transportation, and health care settings. Readersinterested in implementing the process on a regular basis are strongly encouraged toreview the references and additional resources noted at the end of this manual and toconsider additional training, with a clear recognition that such information/training willneed to be adapted to the regulatory requirements and special considerations inherent inthe field of developmental disabilities.2
ContentsPage1What is Root Cause Analysis12Root Cause Analysis and AdverseEvents53Adapting RCA to Evaluate DD SystemDeficiencies124References and Additional Resources185Tools and Techniques20 5 Rules of CausationSequence AnalysisFlowchartingCommon Factors ChecklistBrainstormingAffinity DiagramContributory Factors DiagramEfficiency DiagramSample RCA Report Form3
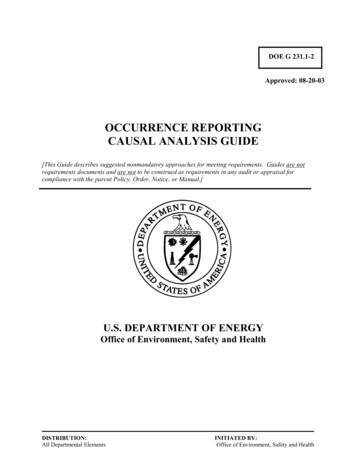
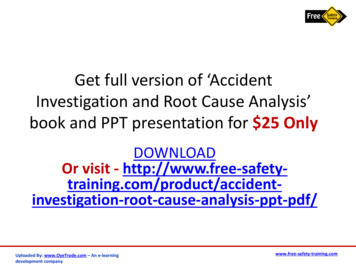
1WHAT is Root CauseAnalysis?Root Cause AnalysisRoot Cause Analysis has been utilized ina wide variety of industries for the pasttwo decades. While the origin of RCAwas within the engineering field, it hasquickly became a standard managementtool in the fields of transportation andtransportation safety, pollution control,nuclear power, information technology,and manufacturing. It is a relativelyrecent addition to the risk managementarmamentarium in the health caresystem, with the JCAHO recognizing itspotential and establishing a requirementfor RCA in its 1999 sentinel eventstandards.The movement to incorporate RCA inhealth care was driven by a recognitionthat the health delivery system hasbecome extremely complex and suffersfrom an abnormally high rate of adverseevents that result in harm and even deathto the consumers of the system.Estimates suggest that almost 4% of allhospitalizations are associated with anadverse event and that 16% of these leadto death or serious disabling injuries.1Accidental Deaths in U.S.120000Medical Errors are the8th Leading Cause of Deathin the United States100000No. Deaths(RCA) isan analytic process designed to helpidentify the underlying factors that havecontributed to or have directly caused amajor adverse event or systems failure.The results of a RCA are typicallyutilized to guide and direct changes toprocesses, the environment, and humanbehavior in order to prevent or reducethe probability that the adverse eventwill occur in the future.800006000040000200000Med Error Motor VehAccFallsCommAviationSource: National Safety CouncilThe results of such error in health careare staggering. According to theHarvard School of Public Health, it isestimated that one million people areinjured in the hospital, and between44,000 and 120,000 people die each yearas a result of medical errors, more thanfrom motor vehicle accidents, breastcancer, and accidental falls combined.2Given the extent of serious injuries anddeaths resulting from preventablemedical errors, the Institute of Medicine3as well as patient safety organizationshave concluded that patient safety can1Hirsch & Wallace (2001)Doing What Counts (2000)3Institute of Medicine (1999)24
only be improved by increasing thefocus on reducing faulty systems. Thisis best accomplished by embracing asystematic approach to learning fromprevious errors and mistakes andmaking changes to organizationalprocesses – not blaming individuals.Root Cause Analysis is the preferred toolfor doing such, and as previouslymentioned, is now a required riskmanagement procedure by the JCHO.More recently the benefits of RCA havestarted to become recognized by thehome health care industry, again drivenby standards established by the JCAHO.4However, the potential of RCA has beenslow to enter the developmentaldisabilities field, even though many ofthe very same issues and causes of injuryand death are equally present in thisservice system. To date there are noknown regulatory or accreditationrequirements for conducting RCA in DDservice and support settings, and there isvery little evidence of its utilization byservice providers or governmentagencies. Given increasing attention toconsumer safety and risk it can bereasonably predicted that in the nearfuture the use of root cause analysis willbecome a common practice in the DDsystem.Some Basic Tenets of RCARoot Cause Analysis is a process ofdiscovery that attempts to find outexactly WHAT happened, WHY ithappened, and HOW it can be preventedfrom happening again. Consequently,the goal of RCA is prevention.Perhaps more importantly, RCA places afocus on understanding, not on blame.4hcpro’s accreditinfo.com (2002)It begins from the basic premise thaterrors and failures are the result of flawsin the system, not simply the action orinaction of people. As noted by Morey5,“ the systems which humans are a partcall forth errors from humans, not theother way around.” Thus, unlike thetraditional process of investigation, RCAdoes not focus on finding out who madethe mistake, but rather why the mistakewas made. The emphasis is onidentifying the environmental andsystem factors that directed or allowed aperson or persons to make the mistake inthe first place.Root Cause Analysis involves anexploration of CAUSE and EFFECTrelationships. It requires a thoroughreview and analysis of human factors,organizational and support systems, andthe formal and informal processes thatguide the actions of people within theorganization. It does this by directing aseries of why questions, over and overagain, to identify the actual and potentialcontribution different factors have tocausing the event under study. Oncecausative and contributory factors areidentified, the process is repeated touncover potential solutions andimprovements to the system that can actas barriers and prevent future failures.Some Concepts and TermsROOT CAUSE ANALYSISProcess to discover WHAT happened WHY it happened HOW it can be preventedFocuses on UNDERSTANDINGnot on BLAMINGAnalyses CAUSE and EFFECTrelationships5Morey (1994) SOLUTIONS andEmphasizesSystem IMPROVEMENTS5
Root Cause Analysis has been designedprimarily as a risk management tool thatcan foster a greater understanding ofwhy an incident has happened thataffects health and safety and what can bedone in the future to prevent itsreoccurrence. There are a few basicconcepts and terms that are important tounderstanding and utilizing the process.1. Adverse Event. Any undesirableincident that causes harm or callsinto question the adequacy of care.2. Barrier. In root cause analysis abarrier represents a process,environmental change, or system thatcan prevent or reduce the probabilityof an adverse event.3. Brainstorming. A process usedwith a group that encourages freethinking and leads to the generationof numerous ideas.4. Contributory Factor. These areadditional reasons, beyond the rootcause, that an adverse event hasoccurred. They increase risk bysetting the stage for or contributingto the probability of an adverseevent.5. Incidental Finding. Problems,inefficiencies or failures in a processor system that did not contribute tothe incident under consideration butwhich require attention by theorganization in order to prevent othertypes of adverse events.6. Proximate Cause. This is the mostobvious reason an adverse eventoccurred. Usually the proximatecause is identified in investigations.Often it reflects a superficialanalysis, focusing on human error.7. Root Cause. This is the most basicand fundamental or underlying causeof an adverse event. It is the “root”of the problem and must beaddressed if prevention strategies areto be effective. In most instances theroot cause is a systems failure, nothuman error.8. Sentinel Event. This is an adverseevent that is unexpected and thatleads directly to or places someone atrisk of death or serious harm.Typical RCA ProcessRoot Cause Analysis is typically utilizedto evaluate a specific adverse or sentinelevent. Team members include personnelthat were directly involved in theincident as well as supervisory andcontent experts in the organization.A minimum of three to four meetings aretypically scheduled, with the team leaderand facilitator performing a number ofactivities both before and in betweenformal meetings.In general, the RCA process involvesperforming a sequence analysis ordetailed description of everything thathappened before, during andimmediately after the adverse event.The process makes liberal use offlowcharting to provide visualillustrations of the sequence and interrelationships between the activities ofthe various units within the organizationthat may have had any involvement withthe incident under study. This isfollowed by brainstorming to identifyfactors that may have influenced orcontributed to the incident and a rigorousprocess of classifying and prioritizingthese factors to identify the true rootcause. Additional time is then spentidentifying possible solutions, resulting6
in the selection of those that appear to bethe most effective and cost efficient.When to Use RCAThere are usually multiple and variedapproaches to solving any givenproblem, each of which has differentresource and time requirements. RootCause Analysis is a very structuredprocess of discovery that requires usersto go through a series of step-by-stepactivities, all designed to find out whysomething happened and what can bedone to prevent it from happening again.Because it is a structured and formalprocess, RCA is relatively timeconsuming.In many organizations the demand forimmediate action can result in atendency to select the most expedientprocess and solution. This need to act,often results in repeated and sometimesfrenzied efforts to manage “symptoms,”rather than the underlying problem thatis responsible for the continuedappearance of adverse events or systemfailures. Expediency can be a “doubleedged sword.” Program and systemmanagers should therefore establishformal or informal criteria to help themdecide when to “pause” and take a morecomprehensive approach to problemsolving, including the use of root causeanalysis.Since RCA is a demanding process, thatrequires a commitment of time andenergy, it should not be usedhaphazardly – i.e., maintain the integrityof the process and reserve its use forspecial circumstances where there issignificant risk if a problem is notcorrected.The inherent need in most organizationsfor immediate action following asignificant event or major failure (e.g.,regulatory citation) can result in atendency to take “shortcuts,” andeliminate steps or modify them to thedetriment of the process. This shouldNOT be done. Save root cause analysisfor when its really needed. And, whenits needed, invest the time and resourceto do it right.USE ROOT CAUSEANALYSIS WHEN: The cause of a MAJOR systemfailure is not evident.There are repeated failures thatare ascribed to HUMANERROR.There is a SENTINEL EVENTthat results in death or seriousinjury.There are a SERIES of incidentsthat could have resulted in deathor serious injury.There is TIME to gatherinformation, conduct aninvestigation, assemble a team,and “think” before acting.DO NOT USE RCA To review every incident orsystem failure.When the reason is obvious.When there is NOT TIME toproceed with a formal andrigorous process of discovery.7
2Root Cause Analysis andAdverse EventsRoot Cause Analysis is astructured set of processes or activitiesdesigned to identify the underlying orfundamental causes of a major adverseevent or incident so that specific actionscan be targeted to the real cause in aneffort to prevent a reoccurrence.RCA takes time. In fact, a typicalreview will involve 3 separate meetingsof a team of selected staff, each of whichis 2-3 hrs in length, plus substantial workin-between meetings to prepareinformation and materials. A decision toconduct a root cause analysis must bemade with recognition of this time andresource commitment. As noted earlier,it is not advisable to institute “shortcuts”that can compromise the process.Steps for Conducting a RCAThe following 6 steps represent arecommended process for use by stateMR/DD agencies that want to conduct aRoot Cause Analysis following asignificant sentinel or adverse event.Typically such events include veryunusual incidents that result in the deathof or serious injury to a consumer of theservice and support system. Once anagency becomes more comfortable withthe process, RCA can be expanded toaddress incidents that could haveresulted in death or serious injury.The specific nature of the incident underreview and the availability of personnel,investigation reports, and othervariables, will influence exactly how anygiven root cause analysis is conducted.In general though, the following stepsshould be followed as closely aspossible.1. Clarify the Issue. RCA should beconducted for one incident oradverse event at a time. If multipleincidents of the same type are underreview, it is usually best to completeeach RCA separately and thenconverge or integrate the findings toidentify common causes orcontributory factors. The first step,therefore, is to identify and clarifythe specific event(s) or incident(s)that the team will analyze. It isstrongly recommended that theorganization establish criteria forselecting events that will meet thethreshold for RCA as well asdesignating an individual or unit forcoordinating and managing theprocess. [Note: most DD agencieshave Quality Assurance, RiskManagement, or QualityImprovement units that could begiven the responsibility for oversightof RCA.]2. Assemble the Review Team. Inagencies that have an establishedRisk Management Division it isrecommended that a member of thatunit always be assigned to the RCAteam. Additional members shouldinclude a management or supervisory8
representative responsible for theprogram or service in which theevent occurred, the investigator orperson most familiar with anyinvestigation that has beencompleted, a content expert withknowledge of best practices, and oneor two personnel who were directlyinvolved in the incident.Membership should be formallyappointed or assigned by a seniorleader in the organization and shouldreflect individuals with knowledge ofthe incident and any policy orpractice requirements associatedwith the type of service or activityinvolved in the incident. Obviously,membership will vary dependingupon the type of incident underreview.3. Assign Roles and Responsibilities.Most teams will include 5-7individuals, all of whom should haveclearly assigned tasks andresponsibilities. At a minimum, theroles of team leader, meetingfacilitator, and note-taker need to beassigned. This leadership group willbe responsible for work in-betweenformal meetings, and should beprepared to commit a least 3-5 hoursbeyond the time directly spent inmeetings. Remaining team membersshould also be given assignmentsbefore the first meeting. Staff eitherdirectly involved in the incidentand/or those who conducted aninvestigation should complete aSequence Analysis prior to the firstformal meeting. A format fordocumenting such an analysis can befound in Chapter 5. Other teammembers can assist with thecollection and organization of otherdata and information that will beutilized in the review.4. Collect Information. Teamleadership should identify importantand relevant documents andinformation that will be needed bythe team. Such documentation willvary based upon the type of incidentunder review, and will include itemssuch as:a. Investigation reportb. Autopsy reportc. Police reportsd. Interviewse. Consumer record (includingmedical record)f. Incident reportsg. Staff notes/logh. Photographs or physicalmaterials involved in theincidenti. Pertinent policies,procedures, protocols, andguidelinesj. Training recordsk. Staffing schedulesl. Inspection or quality reviewrecordsm. Program/site descriptionn. Sequence analysis andassociated flowchart(s)prepared by knowledgeablestaff that summarize exactlywhat happened inchronological order.5. Initiate the Root Cause Analysis.Once this preparatory work has beencompleted, you can begin the actualRoot Cause Analysis by taking thefollowing steps:a. Schedule and organize thefirst meeting, providing9
adequate notice. Since RCArelies on a great deal of visualrepresentation, select alocation that can comfortablyaccommodate the full teamand that has a large markerboard or room for hangingwall charts.and have staff involved in thecase describe exactly whathappened. Allow forquestions and modification ofthe sequence. Use aflowchart to illustrate thesequence once it has beenfinalized.b. Explain the RCA process atthe first full team meeting.Stress the goal of“prevention” and explainhow RCA is different fromthe typical investigationprocess most members willbe more familiar with. Set upa schedule for the remainingmeetings, noting that it willtake between 2 and 3meetings to complete theanalysis, with most meetingslasting 2-3 hours. Emphasizethe need to completeassignments in betweenmeetings in order to make themaximum use of group time.e. Compare what actuallyhappened to what “shouldhave happened.” Comparethe sequence of events(flowchart) to what theagency policy, procedure orprescribed practice expects“should” have occurred.Make notes on the flowchartto identify any deviationsfrom what standard or bestpractice suggests needs tooccur. Make sure the teamleader reiterates the goal ofRCA and that the focus is noton “blaming” someone, butrather for identifying factorsthat may have contributed tothe error, if any.c. Review the incident andidentify the proximatecause. Provide backgroundinformation about theindividual and setting inwhich the incident occurred.Describe in objective termswhat happened. Usually themost immediate or proximatecause will be identified in aninvestigation report. In manyinstances it will reflecthuman error (someone didsomething they shouldn’thave, or didn’t do somethingthey were supposed to.)d. Review the sequenceanalysis that should havebeen prepared ahead of timef. Identify potentialcontributory factors that didor could have led to eachfailure or inability to followpolicy requirements and/orminimum standards. Firstcircle process steps on theflowchart that appear to havecontributed to the incident.Then brainstorm additionalfactors (see Chapter 5 forguidance on brainstorming).Reference the CommonFactors Checklist, also inChapter 5, and go througheach major category to selectand eliminate factors thatcould have contributed to theerror or event. During this10
stage of RCA it is importantto repeatedly use the question“why?” In describingpotential causes of failure,the National Council onPatient Safety recommendsusing the “Five Rules ofCausation” which areincluded in the Appendix.These “rules” stronglysuggest team members avoidnegative descriptors, focus onreal “cause and effect”relationships, always look forpreceding causes to humanerror and proceduralviolation, and assess the basisfor a “duty to act”6 wheneverpersonal noncompliance isidentified.g. Identify incidental findingsor inefficient processes oractivities that may not havedirectly contributed to thefailure, but which should befurther evaluated for possiblerevision. Make a separate listof these for laterconsideration by the agency.This process of noting noncontributory factors or issuesshould occur throughout allof the RCA meetings, butmust be managed so that thegroup does not becomefocused on collateral issues.Therefore, the note-takershould assure members thatthe issue has been recorded6Duty to act is a legal concept. Fault, or noncompliance, can only be attributed to an act orfailure to act when there is a clear requirement todo something, such as is present in a formalpolicy, written program, or a basic and commonpractice standard.ESSENTIALSTEPS IN ROOTCAUSE ANALYSIS Clarify the issueAssemble a teamCollect InformationPerform sequenceanalysisIdentify the proximatecauseIdentify and groupcontributory factorsAsk “WHY,” over andover againDocument incidentalfindingsPropose solutionsReview the literatureand experience ofothersPrioritize solutionsReach consensus oncontent of reportPresent findings andrecommendations toagency leadershipand will be included in the finalreport.h. Organize the identifiedcontributory factors intoclusters. If time permits, theteam facilitator can lead thegroup in developing anAffinity Diagram (seeChapter 5) that can helporganize all of the variablesdiscovered thus far. Analternative approach involvesusing the major headings inthe Common FactorsChecklist and listing each11
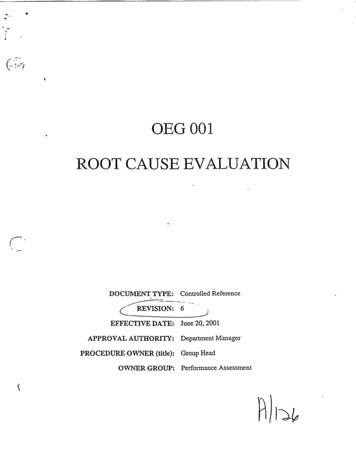
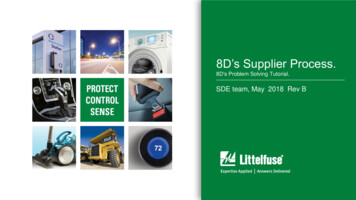
thefactor in its most appropriategroup. [Note: this is a goodpoint to end the first meeting,notifying participants thatthey will be asked to “drilldown” further at the nextmeeting to uncover additionalfactors and begin to prioritizethem.]i. Prioritize the alreadyidentified factors andcontinue brainstorming toidentify even more. This isthe point at which the teamleader should be relentless inpushing the team to ask“Why did the incident takeplace, the human erroroccur?” and “How did eachof these factors contribute tothe adverse event?” Oncethe team has exhausted allpossibilities, reorganize thefactors into clusters. Thenbegin to prioritize theidentified factors, rankordering them according toimportance (e.g., mostimportant to least important).j. Develop a ContributoryFactors Diagram, toillustrate the relationshipsbetween the various factorsyou have identified. Focuson those factors that the teamhas rated as most important.In developing the diagram,work to establish a hierarchy,with the system failure at thetop, followed by theproximate cause, followed bythe categories of contributoryfactors – rank-ordered - eachof which may containmultiple variables. Circlethose factors that appear to beEXAMPLE OF CF ryFactorsCommunicationCF #1CF #2CF #3Staff IssuesCF #4CF #5CF #6TechnologyCF #7CF #8CF #9fundamental cause of theincident.k. Identify the root cause, ormost fundamental reason thatled to the failure. Sometimesthe root cause may be relatedto problems with theprescribed process, i.e.,policy requirements are notconsistent with acceptedpractice standards or basicregulatory requirements. Inother instances the root causemay be related to insufficientcommunication to staff orlack of staff skills orknowledge. It may benecessary to combine one ortwo of the factors to capturethe essence of what the mostimportant cause of theerror/failure was.l.Brainstorm potentialsolutions that could addressthe root cause and prioritycontributory factors. Discussany potential barriers that12
could automatically interferewith or obstruct the mostimportant causes from takingplace. [In RCA a barrier isany physical entity orprocedure that blocks orreduces the likelihood of anaction.] Allow the team tocome up with multiplesolutions and barriers foreach factor. At this point donot attempt to prioritize orevaluate the feasibility of anyideas that are offered. [Note:the completion of this stepmay represent a good point toend the second meeting. Askmembers to think about moresolutions before the thirdmeeting.]m. Gather information fromother sources prior to thelast meeting to provideexamples of how similarissues have been dealt with.As noted earlier, review theprofessional literature, callcolleagues in other agenciesor states, or seek externalconsultation. This processshould be completed beforethe last RCA meeting.n. Review. At the next meetingthe leader should review thefindings to date and shareinformation obtained fromother sources. The team candiscuss this new informationand make revisions, ifappropriate, to the listing ofsolutions and barriers.o. Prioritize solutions. Onceall potential solutions areidentified, the team shouldassess the potentialeffectiveness, feasibility andestimated cost of adoptingeach solution and/or barrier.Approaches that are notpractical (e.g., have asignificant cost or lengthytimeline) should bediscarded, resulting in aprioritized list of solutions,and team selection of the“best” approach for eachfactor. Chapter 5 includesinformation about the use ofan Efficiency Diagram toassist the team in settingpriorities.p. Develop recommendationsbased on the top solutionsthat have been selected.Where possible, estimatepotential cost and discussother special considerationsthat will be important if theproposed solution is adoptedby the leadership of theorganization.q. Prepare a draft report thatincludes your basic findings,rationale, and suggestedsolutions. Chapter 5 includesa RCA Report Form that canbe used or adapted for use asthe format for organizinginformation and preparing areport. Make sure the entireteam has an opportunity toreview and comment on thecontents before issuing thereport.6. Share the report with the agencyleadership. The leadership of theteam should make any neededrevisions based on team membercomment and prepare the finalreport. It is strongly recommended13
that the team leaders schedule a timeto personally present the report to theleadership, making sure to focus onfacts, rationale, and the effectivenessand efficiency of proposed solutions.If leadership agrees, an individual orunit within the organization shouldbe designated as responsible foroverseeing implementation ofstrategies and documenting followup. This latter action is particularlyimportant in order to demonstrate theorganization’s commitment toreducing risk.RECOMMENDED SCHEDULE FOR RCA MEETINGSBefore 1stMEETING1STMEETINGAssign or appoint Explain RCATeam LeaderReview theincident andDesignate teamidentify themembersproximate causeSelect staff toReview Sequenceserve asAnalysisfacilitator andnote-takerCompare toexpectationsClarify the issueAssign tasks(e.g., informationOrganize intoClusters rioritize FactorsReview Literatureand BenchmarksDevelopContributoryFactors DiagramIdentify RootCauseBrainstormpotentialsolutionsIdentify IncidentalFindingsEvaluateSolutions andBarriersDevelopRecommendationsReview contentfor draft reportIdentify IncidentalFindingsMake sure ALL team members have an opportunity to review and commenton the draft findings and recommendations. Broad-based ownership of thefinal product will increase its acceptance and eventual success.14
3Adapting RCA to EvaluateDD System DeficienciesRoot Cause Analysis is designedfor uncovering causative andcontributory factors associated with aspecific sentinel – or adverse – event.As noted earlier, it typically follows arelatively prescribed process thatincludes the formation of a team,gathering of documents and informationrelated to the specific incident,completion of a sequence analysis (withflowcharting), brainstorming andliterature review to identify potentialfactors and solutions, etc. While thisprocess is well suited to the assessmentof a specific event, the basic tenets andsome of the analytic tools included inRCA can be readily adapted to yieldvaluable information about broadersystem failures as evidenced by multipleevents or identified deficiencies (e.g.,citations from a regulatory agency).7-Step ProcessThe following seven steps represent arecommended process for use by stateMR/DD agencies that want to conduct aRoot Cause Analysis for an identifiedsystem failure or deficiency. Thespecific nature of the issue under reviewand a variety of organizationalcharacteristics (administrative structure,geography, resources, etc.) willundoubtedly influence the process.Consequently, it will be important tomodify the recommended steps below inorder to meet situation-specificdemands.Through such adaptation RCA can
Root Cause Analysis represents a structured approach to the investigation and analysis of significant adverse events or system deficiencies and require improvement. This introduction to root cause analysis, and its adaptation to developmental disabilities systems, has been commissioned