Transcription
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGYVOL. 74, NO. 15, 2019ª 2019 THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION.PUBLISHED BY ELSEVIER. ALL RIGHTS RESERVED.THE PRESENT AND FUTUREJACC COUNCIL PERSPECTIVESPreventive Cardiology as a Subspecialtyof Cardiovascular MedicineJACC Council PerspectivesMichael D. Shapiro, DO, MCR,a David J. Maron, MD,b Pamela B. Morris, MD,c Mikhail Kosiborod, MD,d,ePratik B. Sandesara, MD,f Salim S. Virani, MD, PHD,g Amit Khera, MD, MSC,h Christie M. Ballantyne, MD,iSeth J. Baum, MD,j Laurence S. Sperling, MD,k Deepak L. Bhatt, MD, MPH,l Sergio Fazio, MD, PHDmJACC JOURNAL CME/MOC/ECMEThis article has been selected as the month’s JACC CME/MOC/ECMECME/MOC/ECME Objective for This Article: Upon completion of thisactivity, available online at http://www.acc.org/jacc-journals-cme byactivity, the learner should be able to: 1) discuss the coalescence ofselecting the JACC Journals CME/MOC/ECME tab.competencies necessary to provide expert guidance to patients seekingAccreditation and Designation Statementcardiovascular risk assessment and management; and 2) define initialstrategies to consolidate and standardize education and training in car-The American College of Cardiology Foundation (ACCF) is accredited bydiovascular disease prevention.the Accreditation Council for Continuing Medical Education to providecontinuing medical education for physicians.The ACCF designates this Journal-based CME activity for a maximumof 1 AMA PRA Category 1 Credit(s) . Physicians should claim only the creditCME/MOC/ECME Editor Disclosure: JACC CME/MOC/ECME EditorRagavendra R. Baliga, MD, FACC, has reported that he has no financialrelationships or interests to disclose.commensurate with the extent of their participation in the activity.Author Disclosures: Dr. Shapiro has served on an Advisory Board forSuccessful completion of this CME activity, which includes participa-Esperion; has been a consultant to Amarin; and has received institutionaltion in the evaluation component, enables the participant to earn up togrant/research support from the National Institutes of Health (NIH),1 Medical Knowledge MOC point in the American Board of InternalAkcea Therapeutics, Amarin, and the FH Foundation. Dr. Morris has beenMedicine’s (ABIM) Maintenance of Certification (MOC) program. Par-a consultant to and served on an Advisory Board for Akcea Therapeutics;ticipants will earn MOC points equivalent to the amount of CME creditsand has received research funding from Esperion. Dr. Kosiborod has beenclaimed for the activity. It is the CME activity provider’s responsibilitya consultant to and served on Advisory Boards for Amarin, Amgen,to submit participant completion information to ACCME for the pur-Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Eisai,pose of granting ABIM MOC credit.GlaxoSmithKline, Glytec, Eli Lilly, Intarcia, Janssen, Merck (Diabetes),Novartis, Novo Nordisk, and Sanofi; and has received research supportPreventive Cardiology as a Subspecialty of Cardiovascular Medicine:from AstraZeneca, and Boehringer Ingelheim. Dr. Virani has receivedJACC Council Perspectives will be accredited by the European Board forresearch grants from the Department of Veterans Affairs and World HeartAccreditation in Cardiology (EBAC) for 1 hour of External CME credits.Federation; and has received honoraria from the American College ofEach participant should claim only those hours of credit that have actu-Cardiology as associate editor for Innovations, acc.org. Dr. Ballantyne hasally been spent in the educational activity. The Accreditation Council forbeen a consultant to Abbott Diagnostics, Akcea Therapeutics, Amarin,Continuing Medical Education (ACCME) and the European Board forAmgen, Arrowhead, AstraZeneca, Boehringer Ingelheim, Denka Seiken,Accreditation in Cardiology (EBAC) have recognized each other’sEsperion, Intercept, Janssen, Matinas BioPharma, Merck, Novartis, Novoaccreditation systems as substantially equivalent. Apply for creditNordisk, Regeneron, Roche Diagnostic, and Sanofi-Synthelabo; and hasthrough the post-course evaluation. While offering the credits notedreceived institutional grant/research support from Abbott Diagnostic,above, this program is not intended to provide extensive training orAkcea Therapeutics, Amgen, Esperion, Novartis, Regeneron, Rochecertification in the field.Diagnostic, Sanofi-Synthelabo, NIH, American Heart Association, and theMethod of Participation and Receipt of CME/MOC/ECME CertificateAmerican Diabetes Association. Dr. Baum has served on Advisory Boardsfor Sanofi, Regeneron, Amgen, Novartis, and Akcea Therapeutics; has beenListen to this manuscript’saudio summary byEditor-in-ChiefDr. Valentin Fuster onJACC.org.To obtain credit for JACC CME/MOC/ECME, you must:a consultant to Sanofi, Amgen, Regeneron, Novo Nordisk, and Akcea1. Be an ACC member or JACC subscriber.Therapeutics; and has received speaker honoraria from Amgen,2. Carefully read the CME/MOC/ECME-designated article available on-Boehringer Ingelheim, Nordisk, and Akcea Therapeutics. Dr. Bhatt hasline and in this issue of the Journal.3. Answer the post-test questions. A passing score of at least 70% must beserved on the Advisory Boards of Cardax, Elsevier Practice UpdateCardiology, Medscape Cardiology, PhaseBio, and Regado Biosciences; hasachieved to obtain credit.served on the Boards of Directors of the Boston VA Research Institute, the4. Complete a brief evaluation.Society of Cardiovascular Patient Care, and TobeSoft; has served as Chair of5. Claim your CME/MOC/ECME credit and receive your certificatethe American Heart Association Quality Oversight Committee; has servedelectronically by following the instructions given at the conclusion ofon Data Monitoring Committees for the Baim Institute for Clinical Researchthe activity.(formerly Harvard Clinical Research Institute, for the PORTICO trial,ISSN 0735-1097/ 36.00https://doi.org/10.1016/j.jacc.2019.08.1016
Shapiro et al.JACC VOL. 74, NO. 15, 2019OCTOBER 15, 2019:1926–42Preventive Cardiology as a Subspecialtyfunded by St. Jude Medical, now Abbott), Cleveland Clinic (including forResearch and Publications Committee (chair); has received researchthe ExCEED trial, funded by Edwards Lifesciences), Duke Clinical Researchfunding from Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer,Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGEBoehringer Ingelheim, Bristol-Myers Squibb, Chiesi, CSL Behring, Eisai,trial, funded by Daiichi-Sankyo), and Population Health Research Institute;Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Idorsia, Ironwood,has received honoraria from the American College of Cardiology (seniorIschemix, Lilly, Medtronic, PhaseBio, Pfizer, Regeneron, Roche, Sanofi,associate editor, Clinical Trials and News, ACC.org, and vice chair of theSynaptic, and The Medicines Company; has received royalties fromACC Accreditation Committee), Baim Institute for Clinical ResearchElsevier (editor, Cardiovascular Intervention: A Companion to Braunwald’s(formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trialHeart Disease); has been a site coinvestigator for Biotronik, Bostonsteering committee funded by Boehringer Ingelheim), Belvoir PublicationsScientific, St. Jude Medical (now Abbott), and Svelte; has been a trustee for(Editor-in-Chief, Harvard Heart Letter), Duke Clinical Research Institutethe American College of Cardiology; and has performed unfunded research(clinical trial steering committees, including for the PRONOUNCE trial,for FlowCo, Fractyl, Merck, Novo Nordisk, PLx Pharma, and Takeda. Dr.funded by Ferring Pharmaceuticals), HMP Global (Editor-in-Chief, JournalFazio has been a consultant to Amarin, Amgen, AstraZeneca, Esperion, andof Invasive Cardiology), Journal of the American College of Cardiology (guestNovartis. All other authors have reported that they have no relationshipseditor; associate editor), Medtelligence/ReachMD (CME steeringrelevant to the contents of this paper to disclose.committees), Population Health Research Institute (for the COMPASSoperations committee, publications committee, steering committee, andUSA national coleader, funded by Bayer), Slack Publications (chief medicaleditor, Cardiology Today’s Intervention), Society of Cardiovascular PatientMedium of Participation: Print (article only); online (article and quiz).CME/MOC/ECME Term of ApprovalCare (secretary/treasurer), and WebMD (CME steering committees); hasother relationships with Clinical Cardiology (deputy editor),Issue Date: October 15, 2019NCDR-ACTION Registry Steering Committee (chair), and VA CARTExpiration Date: October 14, 2020The views expressed in this paper by the American College of Cardiology’s (ACC’s) Prevention Council do not necessarily reflectthe views of the Journal of the American College of Cardiology nor the ACC.From the aCenter for Preventive Cardiology, Section on Cardiovascular Medicine, Wake Forest University Baptist Medical Center,Winston-Salem, North Carolina; bDepartment of Medicine and Cardiovascular Institute, Stanford University, Stanford, California;cSeinsheimer Cardiovascular Health Program, The Medical University of South Carolina, Charleston, South Carolina; dSaint Luke’sMid America Heart Institute and University of Missouri-Kansas City, Kansas City, Missouri; eThe George Institute for GlobalHealth, Sydney, New South Wales, Australia; fDivision of Cardiology, Department of Medicine, Emory University School ofMedicine, Atlanta, Georgia; gMichael E. DeBakey Veterans Affairs Medical Center and Baylor College of Medicine, Houston, Texas;hDivision of Cardiology, UT Southwestern Medical Center, Dallas, Texas; iBaylor College of Medicine, Houston, Texas; jCharles E.Schmidt College of Medicine, Florida Atlantic University, Boca Raton, Florida; kEmory Heart Disease Prevention Center, EmoryUniversity School of Medicine, Atlanta, Georgia; lBrigham and Women’s Hospital Heart and Vascular Center, Harvard MedicalSchool, Boston, Massachusetts; and themCenter for Preventive Cardiology, Knight Cardiovascular Institute, Oregon Health &Science University, Portland, Oregon. Dr. Shapiro has served on an Advisory Board for Esperion; has been a consultant to Amarin;and has received institutional grant/research support from the National Institutes of Health (NIH), Akcea Therapeutics, Amarin,and the FH Foundation. Dr. Morris has been a consultant to and served on an Advisory Board for Akcea Therapeutics; and hasreceived research funding from Esperion. Dr. Kosiborod has been a consultant to and served on Advisory Boards for Amarin,Amgen, Applied Therapeutics, AstraZeneca, Bayer, Boehringer Ingelheim, Eisai, GlaxoSmithKline, Glytec, Eli Lilly, Intarcia,Janssen, Merck (Diabetes), Novartis, Novo Nordisk, and Sanofi; and has received research support from AstraZeneca, andBoehringer Ingelheim. Dr. Virani has received research grants from the Department of Veterans Affairs and World HeartFederation; and has received honoraria from the American College of Cardiology as associate editor for Innovations, acc.org. Dr.Ballantyne has been a consultant to Abbott Diagnostics, Akcea Therapeutics, Amarin, Amgen, Arrowhead, AstraZeneca,Boehringer Ingelheim, Denka Seiken, Esperion, Intercept, Janssen, Matinas BioPharma, Merck, Novartis, Novo Nordisk, Regeneron, Roche Diagnostic, and Sanofi-Synthelabo; and has received institutional grant/research support from Abbott Diagnostic,Akcea Therapeutics, Amgen, Esperion, Novartis, Regeneron, Roche Diagnostic, Sanofi-Synthelabo, NIH, American Heart Association, and the American Diabetes Association. Dr. Baum has served on Advisory Boards for Sanofi, Regeneron, Amgen, Novartis,and Akcea Therapeutics; has been a consultant to Sanofi, Amgen, Regeneron, Novo Nordisk, and Akcea Therapeutics; and hasreceived speaker honoraria from Amgen, Boehringer Ingelheim, Nordisk, and Akcea Therapeutics. Dr. Bhatt has served on theAdvisory Boards of Cardax, Elsevier Practice Update Cardiology, Medscape Cardiology, PhaseBio, and Regado Biosciences; hasserved on the Boards of Directors of the Boston VA Research Institute, the Society of Cardiovascular Patient Care, andTobeSoft; has served as Chair of the American Heart Association Quality Oversight Committee; has served on Data MonitoringCommittees for the Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial,funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards Lifesciences),Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by DaiichiSankyo), and Population Health Research Institute; has received honoraria from the American College of Cardiology (seniorassociate editor, Clinical Trials and News, ACC.org, and vice chair of the ACC Accreditation Committee), Baim Institute forClinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded byBoehringer Ingelheim), Belvoir Publications (Editor-in-Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinicaltrial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor-inChief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (guest editor; associate editor), Medtelligence/ReachMD (CME steering committees), Population Health Research Institute (for the COMPASS operations committee,publications committee, steering committee, and USA national coleader, funded by Bayer), Slack Publications (chief medicaleditor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (secretary/treasurer), and WebMD1927
1928Shapiro et al.JACC VOL. 74, NO. 15, 2019OCTOBER 15, 2019:1926–42Preventive Cardiology as a SubspecialtyPreventive Cardiology as a Subspecialty ofCardiovascular MedicineJACC Council PerspectivesMichael D. Shapiro, DO, MCR,a David J. Maron, MD,b Pamela B. Morris, MD,c Mikhail Kosiborod, MD,d,ePratik B. Sandesara, MD,f Salim S. Virani, MD, PHD,g Amit Khera, MD, MSC,h Christie M. Ballantyne, MD,iSeth J. Baum, MD,j Laurence S. Sperling, MD,k Deepak L. Bhatt, MD, MPH,l Sergio Fazio, MD, PHDmABSTRACTAlthough significant progress has been made to reduce the global burden of cardiovascular disease, efforts have focusedprimarily on treatment of manifest disease rather than on prevention of events. An enormous opportunity exists totransition focus from intervention to providing equal attention to prevention of cardiovascular disease. The nascentspecialty of “preventive cardiology” is emerging from the background of long-established services such as lipid, diabetes,hypertension, and general cardiology clinics. It is incumbent on the cardiology community to invest in cardiovascularprevention because past gains are threatened with the rising tide of obesity and diabetes. Now is the time to establish adedicated preventive cardiology subspecialty to train the clinicians of the future. This American College of CardiologyCouncil Perspective aims to define the need for preventive cardiology as a unique subspecialty, broaches controversies,provides a structure for future training and education, and identifies possible paths forward to professional certification.(J Am Coll Cardiol 2019;74:1926–42) 2019 the American College of Cardiology Foundation. Published by Elsevier.All rights reserved.Over the last 4 decades, we have witnessedcardiovascular (CV) mortality are reaching a nadir,significant reductions in morbidity andour health care system is unable to support additionalmortalitydiseasetherapies, particularly those that are prohibitively(CVD) (1). Nonetheless, CVD remains the leading killerexpensive and with modest impact on risk reduction.in both men and women across the globe. What is lessFurthermore, past gains are threatened by thefromcardiovascularrecognized, however, is that at least one-half of whatexpanding epidemics of obesity and diabetes (3),has been achieved in terms of improvement in CVDand this has brought to the forefront the practicaloutcomes relates to greater access to procedural in-value and need for expansion of structured andterventions and technological advancements thatcomprehensiveallow patients to live and cope with advanced athero-Indeed, it is likely that a paradigm shift is necessarysclerotic cardiovascular disease (ASCVD) and heartto fulfill the promise of improving CV health in thefailure rather than preventing the disease in the firstpopulation at large. Put another way, the real revolu-place (2). Although avoiding earlier death, these indi-tion in CVD prevention will occur when greater ef-viduals are at high risk for disability, and theirforts and resources are applied to all preventivecontinued clinical needs are associated with signifi-efforts (secondary, primary, and primordial preven-cant cost to the health care system. As declines intion) (4). As such, preventive cardiology as a uniqueinterventionsto(CME steering committees); has other relationships with Clinical Cardiology (deputy editor), NCDR-ACTION Registry SteeringCommittee (chair), and VA CART Research and Publications Committee (chair); has received research funding from Abbott,Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, CSL Behring, Eisai,Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Idorsia, Ironwood, Ischemix, Lilly, Medtronic, PhaseBio, Pfizer,Regeneron, Roche, Sanofi, Synaptic, and The Medicines Company; has received royalties from Elsevier (editor, CardiovascularIntervention: A Companion to Braunwald’s Heart Disease); has been a site coinvestigator for Biotronik, Boston Scientific, St.Jude Medical (now Abbott), and Svelte; has been a trustee for the American College of Cardiology; and has performed unfunded research for FlowCo, Fractyl, Merck, Novo Nordisk, PLx Pharma, and Takeda. Dr. Fazio has been a consultant toAmarin, Amgen, AstraZeneca, Esperion, and Novartis. All other authors have reported that they have no relationships relevantto the contents of this paper to disclose.Manuscript received August 6, 2019; accepted August 20, 2019.preventCVD.
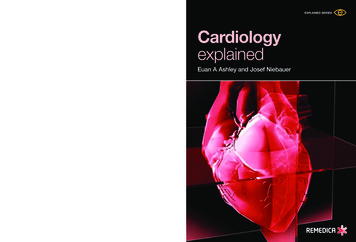
Shapiro et al.JACC VOL. 74, NO. 15, 2019OCTOBER 15, 2019:1926–421929Preventive Cardiology as a SubspecialtyHIGHLIGHTS The medical community must invest incardiovascular disease preventionbecause past gains are threatened byincreased rates of obesity and diabetes.Framingham opened up the whole field ofABBREVIATIONSpreventive cardiology by identifying modifi-AND ACRONYMSable risk factors for heart disease. Next, clinicaltrialsextendedtheepidemiologicalfindings to demonstrate that managing hypercholesterolemia, hypertension, cigarette An enormous opportunity exists to transition focus from intervention to prevention of cardiovascular disease. Given the array of dedicated skillsnecessary to manage cardiovascular risk,the specialty of “preventive cardiology”is emerging.ABIM American Board ofInternal MedicineACC American College ofCardiologysmoking, and diabetes reduced the risk forAHA American HeartASCVD across age and sex (7). Indeed, sinceAssociationthe landmark publication of 4S study (Scan-ASCVD atheroscleroticdinavian Simvastatin Survival Study) in 1994,cardiovascular diseaseanCAC coronary artery calciumuninterruptedstreamofrandomizedcontrolled trials validated the effectivenessCV cardiovascularof statin drugs in virtually all clinicallyCVD cardiovascular diseaserelevant patient groups (8). Due to the successEPA eicosapentaenoic acidof several early studies, trial design pro-FDA U.S. Food and Drugsubspecialty is emerging naturally and spontaneouslygressed from placebo-controlled to statin-Administrationas a separate discipline providing a comprehensivecontrolledIMT intima-media thicknessapproach to a sector of CV care with enormouslymoderate-intensity) studies. The clinical out-LDL-C low-densityincreasing demand. However, this subspecialty is incomes from these studies suggested that therelipoprotein cholesterolits infancy and remains fragmented and disorganizedwas no low-density lipoprotein cholesterolLp(a) lipoprotein(a)at all levels, from education and training, to imple-(LDL-C) level below which patients did notMACE major adversementation, operations, and coordination with stan-receive further benefit, thus setting the stagecardiovascular eventsdard of care services. This subspecialty will notfor the current standard of statin recommen-MI myocardial infarctionrealize its full potential until political barriers aredation for all individuals above a certain riskPCSK9 proproteintranscended, training is standardized, structured,threshold. The improved CVD outcomesconvertase/subtilisin kexinand delivered as part of dedicated fellowships, andobserved across the statin mega-trials wererecognition by a national certifying body is achievedimpressive and strikingly consistent. Moreover, the(5). What follows is a critical examination of theresults of these studies transformed the way cliniciansneed for the development of preventive cardiologyperceived hypercholesterolemia and combined dysli-as a subspecialty, highlighting the barriers to itspidemia, both in terms of risk assessment andmaturation and the opportunities for successfultreatment.(high-intensityvs.low-ortype 9As the understanding that LDL-C lowering is safe,implementation and growth.easy to achieve, and effective at mitigating athero-A HISTORICAL PERSPECTIVE OF PREVENTIVEsclerotic risk in broad populations became widelyCARDIOLOGY—HOW WE GOT delines adopted LDL-C lowering as a top priorityThe Framingham Heart Study, launched in 1948,for ASCVD risk management. At the same time,established the principle of CV risk, with its com-proper risk assessment became a key driver of treat-pounding predictive factors (6). Early work fromments that are long-term and occasionally associatedT A B L E 1 Components of an Academic Preventive Cardiology ProgramClinical staffSpecialized physiciansClinical pharmacistDietitianServicesDaily outpatient clinics Counseling on diet, exercise,and smoking cessationAdvanced practice providersCardiac rehabilitationPCSK9 inhibitor clinic LDL apheresisOutreach clinics andtelemedicineDiagnosticsLipid and biomarkerlaboratorySubclinical atherosclerosisimaging (CIMT, CACS,CCTA)Genetic testingAmbulatory bloodpressuremonitoringEchocardiographyStress testingEducationPreventive cardiologyfellowsGeneral cardiology fellowsInternal medicineresidentsMedical studentsVisiting physiciansClasses for patients,staff, and the publicResearchBasic science in lipidsTranslational studiesand vascular biologyClinical trials of noveltherapeutics anddevicesRegistry andbiorepositoryClinical research (familyEpidemiologicalstudies, cohorts, EMR)studiesGenetic counselorRegistered nurseCACS ¼ coronary artery calcium score; CCTA ¼ coronary computed tomography angiography; CIMT ¼ carotid intima-media thickness; EMR ¼ electronic medical record; LDL ¼ low-density lipoprotein;PCSK9 ¼ proprotein convertase/subtilisin kexin type 9.
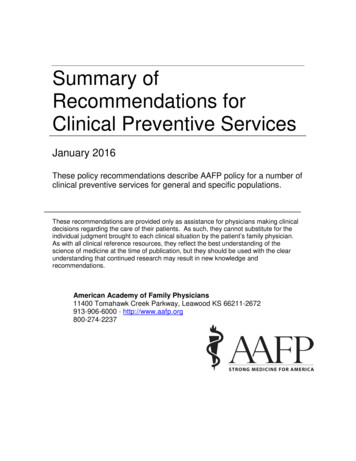
1930Shapiro et al.JACC VOL. 74, NO. 15, 2019OCTOBER 15, 2019:1926–42Preventive Cardiology as a Subspecialtywith side effects. Specialty lipid clinics emerged tooptimize implementation of evidence-based guidelines for lipid-lowering therapies, to provide management for patients with high-risk genetic lipidT A B L E 2 Common Indications for Referral toPreventive Cardiology ServicesCardiovascular risk assessmentNutritional interventionsdisorders, and for consultative guidance in the settingLifestyle counselingof treatment-associated adverse effects. However, itSmoking cessationhas become increasingly recognized that cholesterolCardiac rehabilitationmanagement is most often required for individualsFamily history of premature ASCVDwhose ASCVD risk is driven by a multiplicity ofcomorbidities and risk exposures. Thus, lipid management is 1 component of a comprehensive inter-Personal history of ASCVD, particularly in individuals 60 yrs of ageInherited and/or severe dyslipidemiasEvaluation and management of SAMSLDL apheresisvention addressing multiple important ASCVD riskGenetic testingfactors, often including a combination of therapeuticNoninvasive atherosclerosis imaginglifestyle changes and medical therapies. This conceptOptimization of hypertension managementshould be extended to the management of hyper-Optimization of diabetes managementtension, diabetes, obesity, and suboptimal lifestyleParticipation in clinical trialshabits, and so on—all of which can be addressed under the auspices of a dedicated preventive cardiologyASCVD ¼ atherosclerotic cardiovascular disease; LDL ¼ low-density lipoprotein;SAMS ¼ statin associated muscle symptoms.program. As the need to identify more tionsemerged, the value of the limited specialty clinicapproaches for treatment and prevention. Table 2model diminished and the roots of preventive cardi-delineates common indications for referral to pre-ology took hold. It became increasingly apparent thatventive cardiology services.to prevent ASCVD most effectively, multiple riskLIPID-RELATED RISK. Scientists and clinicians fromfactor interventions are required.varied backgrounds have been drawn to the relationGlobal risk assessment tools have limitations, withbetween cholesterol and ASCVD since 1913 whenprior algorithms underestimating and more modernNikolai Ansitschkow, a Russian pathologist, fed purerisk scores at times overestimating risk. Moreover,cholesterol to rabbits to induce aortic atherosclerosisrisk assessment tools for ASCVD, although helpful,(10). The Framingham Heart Study launched thecontinue to exhibit gaps, such as not accounting forconcept of risk factors for ASCVD, a model that is justthe risk of heart failure, and also require frequentas important today (6). Years later, John Gofman, aupdating to incorporate contemporary data (9).physicist, defined plasma lipoproteins using analyt-Current work moves from population-level data andical ultracentrifugation, and demonstrated the directrisk factors, such as cholesterol, to a new generationand inverse relationships LDL-C and high-density li-of precision medicine and tailored therapeutics.poprotein cholesterol levels, respectively, have withWithin the realm of preventive cardiology, refine-rates of myocardial infarction (11). Ten years later,ment in risk estimation and therapeutic decisionKonrad Bloch and Feodor Lynen were awarded themaking is being facilitated by atherosclerosis imag-Nobel Prize for determining the complex metabolicing (e.g., ultrasound for carotid intima-media thick-pathway of cholesterol synthesis (12). In 1973, Michaelness and carotid plaque, computed tomography forBrown and Joe Goldstein made their groundbreakingcoronary artery calcium score), new biomarkers,discoveries related to the LDL receptor, with theadvances in genetic testing (identification of causaloriginal inspiration for their work being a young childmonogenic mutations and development of action-who sustained a heart attack due to homozygous fa-able polygenic risk scores), and a plethora of pipe-milial hypercholesterolemia (13,14).line and market pharmaceuticals with promise orThe Lipid Research Clinics–Coronary Primary Pre-proof of benefits. Given the proliferation of newvention Trial with cholestyramine and the Coronarydata, approaches, and pharmacotherapy, preventiveDrug Project with niacin ushered in the era of lipidcardiology needs a structure to deliver specializedmodulation for prevention of heart disease (15–17).training and produce dedicated clinician-scientistsThese studies gave birth to the concepts of primaryand practitioners to serve this ever-growing medi-and secondary prevention of CVD and paved the waycal need (Table 1). This new direction will befor the development and utilization of the statinimportant to help us define risks early, initiatedrugs, an incredible journey since lovastatin enteredappropriate treatments, and identify new drugs/the market in 1987 (18).
Shapiro et al.JACC VOL. 74, NO. 15, 2019OCTOBER 15, 2019:1926–42Preventive Cardiology as a SubspecialtyMere decades ago, atherosclerosis was seen as anscience and translation to patient management haveinevitable consequence of aging—a degenerative dis-andease about which nothing could be done. Today,knowledge to optimize evaluation and managementprevention of ASCVD has acquired status as anof patients at risk for CVD events. The basic role of theeffective, practical, and widely applicable art. Theprimary care provider in managing CV risk should bedisease is eminently preventable, and lowering bloodand likely will continue unchanged, even aftercholesterol is always effective, though often margin-specialized preventive cardiology services are avail-ally, irrespective of the original drivers of the disease.able in all major markets. However, select patientsEMERGING SCIENCE IN CVD RISK REDUCTION. Therelatively recent discovery of proprotein convertase/subtilisin kexin type 9 (PCSK9) as a master regulator ofplasma LDL-C has revolutionized our understandingof lipid metabolism (19,20). Two fully human mono-continuetoevolve,requiringsubspecialtywill benefit from evaluation and management from adedicated preventive cardiology service for accurateCVD risk assessment and optimal management inclusive of lifestyle, supplemental, and pharmacological therapy.clonal antibodies that antagonize PCSK9 action wereINFLAMMATORY RISK. ASCVD event rates are unac-approved by the U.S. Food and Drug Administrationceptably high, even among patients intensively(FDA) just 12 years after the discovery of this protein,treated with existing therapies. The concept of resid-and landmark trials have demonstrated incrementalual CV risk implies that outcomes may be improved byimprovement in CV outcomes when these agents aretargeting other CV risk factors and com
Preventive Cardiology as a Subspecialty of Cardiovascular Medicine: JACC Council Perspectives will be accredited by the European Board for Accreditation in Cardiology (EBAC) for 1 hour of External CME credits. Each participant should claim only those hours of credit th