Transcription
2/16/2018The Maternal Fetal TriageIndexCatherine Ruhl, MS, CNMDirector, Women’s Health ProgramsAWHONNDisclosures No commercial support or sponsorship was received forthis presentation Presenter reports no relevant financial or commercialconflicts related to this conference@2015 AWHONN21
2/16/2018Objectives1. Discuss the concept of“triage” as a nursing roleand responsibility2. Describe how astandardized approachto obstetric triage canimprove processes andoutcomes3. Explain the developmentand use of AWHONN’sMaternal Fetal TriageIndex (MFTI)@2015 AWHONN3Quality Triage CareShould women have to wait to betriaged?Do you have a standardized approach towomen who present with hypertension orother non-labor conditions?@2015 AWHONN42
2/16/2018Three women arrive on aholiday eve Woman #1G3P200228 yo39.0 wksCtx q 2-3BOWIWoman#2G2P100122 yo29.2 wks FMNo labor sxWoman#3G1P018 yo38 wksc/o HAno ctx Holding abdomen w/ ctxWho does RN see first?Where do the others wait?@2015 AWHONN5Triage is a process@2015 AWHONN63
2/16/2018Triage is not a place@2015 AWHONN7AWHONN’s Triage Initiative Re-define “OB triage” Reaffirm obstetric triage as a nursing role Improve quality of triage nursing care throughstandardization of acuity classification (theMFTI) Improve education for nurses about triage Test a triage quality measure@2015 AWHONN84
2/16/2018AWHONN’sDefinition of Obstetric TriageObstetric triage is the brief,thorough and systematicmaternal and fetalassessment performed whena pregnant woman presentsfor care, to determine priorityfor full evaluation.@2015 AWHONN9AWHONN’sDefinition of Obstetric Triage Obstetric triage isperformed by nurses. Triage is followed by thecomplete evaluation ofwoman and fetus byQualified Medical Personnel(MD, CNM, NP, or RN whomeets requirements)@2015 AWHONN105
2/16/2018Triage and Escalation(RN)Evaluation(provider orRN/provider)Disposition(Provider) Mobilization: process of movingpeople or resources Escalation: intensifying efforts@2015 AWHONN11Comparing ED and OB triageEmergency Department “Triage” refers to the briefRN assessment todetermine the urgency forevaluationBirth units “Triage” (pre-MFTI) refers toRN’s initial assessment andprovider evaluation Occurs in a triage intakearea May occur on a separateunit or in the LDR Nationally-accepted acuityclassification tooldetermines priority forevaluation Prior to MFTI, no nationalstandard for assigningpriority for evaluation@2015 AWHONN126
2/16/2018Comparing ED and OB triageEmergency Department Triage RN qualifications:standardized course andorientationBirth units Triage RN qualifications?Orientation to triage? Triage RN responsibilities:help out in ED when notriages Triage RN duties: continueto care for pt during evaland obs, may be chargenurse, may have admittedpt assignments@2015 AWHONN13Comparing ED and OB triageEmergency Department Value of triage RN- “Themost important nurse in theED—even more importantthan the charge nurse” (NHnurse) Why so valuable?Birth units Value of triage RN: Not awell-defined role until nowso more challenging toestablish value– First line of defense– First to identify problems– First to mobilize staff andresources– First line of defense– First to identify problems– First to mobilize staff andresources Why so valuable?@2015 AWHONN147
2/16/2018ENA’s triage qualifications ENA supports use of a reliable, valid 5-level triagescale Minimum one year experience as an emergencynurse Complete a comprehensive course and clinicalorientation Ongoing competency validationEmergency Nurses Association. (2017). Triage qualifications and competency.@2015 AWHONN15Where do you triage? How many have anintake area for triage? How many have aseparate area or roomsfor triage andevaluation? How many triage in theLDRs?@2015 AWHONN168
2/16/2018Do you use atriage acuity tool?Photo used with permission from Jenn Doyle.@2015 AWHONN17Does your main ED use atriage acuity index? Why should ahospitalized pregnantwoman receive adifferent standard ofcare than a nonpregnant woman?@2015 AWHONN189
2/16/2018Triage Assessment Elements Chief complaint*Vital signs/ FHRFetal movementCtx/LOF/BleedingPain rating (non-laborcomplaint) Coping with labor Mental statusPregnancy historyPast OB historyPast med/surg history/allergies Social history*Infectious diseaseexposure if relevant@2015 AWHONN19Why standardize triage?1. Improve nurse-providercommunication2. Decrease errors/potentialliability3. Standardize education ontriage4. Standardize triageassessment5. Mobilize resourcesefficiently6. Obtain valuable dataFirst come First served!https://www.youtube.com/watch?v apzgT1zpHzgThese reasons apply to OB units of every size, largeand small 2014 AWHONN10
2/16/2018Triage and Liability Failure to triage and evaluate a womanappropriately– 2nd most common allegation*– 21% of professional liability claims* Case example– Failure of triage nurse to present an accuratepicture of the case to the attending*Review of 100 cases of alleged obstetric liability, 1985-2010.Muraskas et al., 2012 2013 AWHONN21Triage and Liability Failure to transport a woman to a tertiarycenter when indicated– 4th most common allegation*– 11% of professional liability claims* Case examples– Extreme prematurity, complicated twin gestations,triplets or higher orders, known congenitalanomalies*Review of 100 cases of alleged obstetric liability, 1985-2010.Muraskas et al., 2012 2013 AWHONN2211
2/16/2018Areas of Risk in OB Triage Timeliness of– assessment– response from OB Providers and consultants,– transfer of high risk patients to an appropriatefacility equipped to provide the required level ofspecialized care. (Angelini, 2013). Serious reportable events involved fetaldeaths related to timeliness of triage,evaluation and intervention 2013 AWHONN23OB Triage Education Trinity Health System reports in 2015:– 5% of OB RN Directors using an acuity tool OBtriage.– None of the 35 birthing hospitals use astandardized education program to orient RNs tothe role of the OB triage nurse.– Majority of hospitals assign RNs to work in thetriage area after working a designated period oftime in labor and delivery; usually a minimum ofone year.– Lack of objective competency assessment 2013 AWHONN2412
2/16/2018Classifying acuity gives youvaluable data!1. Acuity trends2. Track time from presentation until triage complete, time toevaluation per priority level3. Track patient LOS in triage/eval unit and overall flow basedon acuity4. Track adequacy of nurse staffing in triage r/t acuity5. Measure women’s satisfaction with triage and evaluation6. Track decrease in new reportable events r/t triage andevaluation 2014 AWHONNThe gestation of the MaternalFetal Triage Index (MFTI)1. Expert task forcedrafted an acuity tool2. Content validation(RN, CNM, MD)3. Interrater reliability4. Educational moduletestingOver 100 nurses, physicians and midwivescontributed to developing the MFTI!@2015 AWHONNRuhl, Scheich, Onokpise& Bingham, 20152613
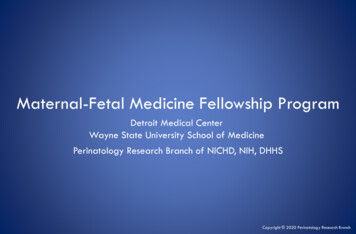
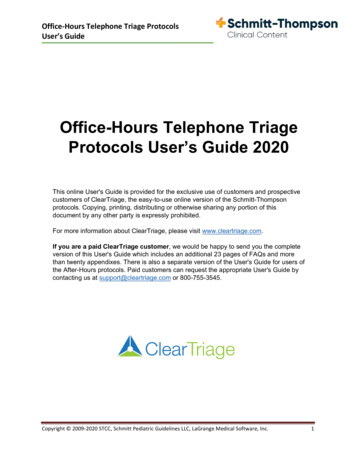
2/16/2018Foundational acuity indexesThe Emergency Severity IndexAgency for HealthcareResearch and Quality, 2012Fla Hospital OB Triage ToolPaisley, Wallace & DuRant, 2011AWHONN’sMaternal Fetal Triage Index Exemplaryclinicalconditionson the right Vital signsaresuggestedvalues-UseFIRST set. Five levels ofacuity Key questionson the left Includes needto transfer tohigher level ofcare@2015 AWHONNRuhl, Scheich,Onokpise &Bingham, 20152814
2/16/2018Stat (Priority 1)(abbreviated version) Does the woman or fetushave STAT/PRIORITY 1 vitalsigns?or Does the woman or fetusrequire immediatelifesaving intervention?or Is birth imminent? Abnormal Vital Signs––––Maternal HR 40 or 130ApneicSp02 93%SBP 160 or DBP 110 or 60/palpable– No FHR– FHR 110 bpm for 60seconds Lifesaving interventionso Maternalo Fetal*Vital signs are suggestedvalues Imminent birth 2014 AWHONNUrgent (Priority 2)(abbreviated version) Does the woman or fetushave URGENT/PRIORITY 2vital signs? OR Is the woman in severe painunrelated to contractions?OR Is this a high-risk situation?OR Will this woman and/ornewborn require a higherlevel of care?Abnormal Vital Signs* Maternal HR 120 or 50, Temperature 101.0 F,(38.3 C), R 26 or 12, Sp02 95%, SBP 140 or DBP 90,symptomatic or 80/40, repeated FHR 160 bpm for 60seconds; decelerationsSevere Pain: (not ctx) 7 on a0-10 pain scale*Vitals signs are suggested values 2014 AWHONN15
2/16/2018Urgent (Priority 2)(abbreviated version) Is this a high-risk situation? 2014 AWHONNPrompt (Priority 3)(abbreviated version) Does the woman or fetushave PROMPT/PRIORITY 3vital signs? Does the woman requireprompt attention? Abnormal Vital SignsTemperature 100.4 F, 38.0 C1,SBP 140 or DBP 90,asymptomaticPrompt Attention such as: Signs of active labor 34 weeks c/o early labor signs and/or c/oSROM/leaking 34–36 6/7 weeks 34 weeks planned, elective,repeat cesarean with regular Woman is not coping with laborper the Coping with LaborAlgorithm V216
2/16/2018Non-urgent (Priority 4) Does the womanhave a complaintthat is non-urgent? Non-urgent attention suchas: 37 weeks early labor signsand/or c/o SROM/leaking Non-urgent symptoms mayinclude: commondiscomforts of pregnancy,vaginal discharge,constipation, ligament pain,nausea, anxiety.Scheduled/Requesting(Priority 5) Is the womanrequesting a serviceand she has nocomplaint?OR Does the womanhave a scheduledprocedure with nocomplaint? Woman Requesting aService, such as: Prescription refill Outpatient service that wasmissed Scheduled Procedure Any event or procedurescheduled formally orinformally with the unitbefore the patient’s arrival,when the patient has nocomplaint.17
2/16/2018What RNs are saying about the MFTI “I love the MFTI. It really promptsyou to be aware of what priorityyour patients are.” “The MFTI is great and easy touse!” “I used to have difficulty trying todetermine who needed myattention first.” “I really like the vital signs clearlylisted as part of the MFTI. It reallyhelps in our timely treatment ofpatients with hypertensiveemergency.”Photo used with permission fromBrianne Fallon, RN, Shawnee MissionMC, Shawnee Mission, KSWhy is the MFTI unique? Mom AND baby The only nationalobstetric triage acuitytool for the entirety ofpregnancy Multidisciplinary input Rigorous developmentby AWHONN18
2/16/2018Hospital-Based Triage of Obstetric PatientsACOG Committee Opinion #667 July, 2016“Recently developed ,validated algorithms suchas the Association ofWomen’s Health,Obstetric and NeonatalNurses’ Maternal FetalTriage Index could serve astemplates for use inindividual hospital units.”@201637How can the MFTIimprove care? Not missing abnormalpresenting vital signs Early identification ofneed to transfer tohigher level of care Not missing scheduledwomen who havecomplaints Proper attention to– non-ctx pain– women not copingwith labor– decreased fetalmovement– possible pretermcontractions@2015 AWHONN3819
2/16/2018What is NOT in the MFTI? Cervical dilation Necessity of a FHR strip Time to providerevaluation based onpriority level Frequency of RNreassessment whileawaiting evaluation Not a diagnosticalgorithm@2015 AWHONN39Clinical Judgment The MFTI guides clinical decision-making Some clinical presentations may not meet theexact criteria described in the MFTI Prioritize to the higher level when there is alack of clarity The MFTI can protect from cognitive bias 2014 AWHONN20
2/16/2018Now it’s your turn! Systematically assess the following casesalways keeping in mind:– Vital signs– Pain rating for non-labor pain– Coping/not coping if in labor– Fetal movement? 2013 AWHONN41Three triaged women on aholiday eve Woman #1G3P200228 yo39.0 wksCtx q 2-3BOWIHolding abd w/ ctxVS, FHR WNLCoping w/ ctxWoman#2G2P100122 yo29.2 wks FMNo labor sxVS, FHR WNL dopplerWoman#3G1P018 yo38 wksc/o HA, 5/10 painBP 126/72, FHR WNLWhat are their MFTI priority levels?Which woman gets the one available bed?@2015 AWHONN4221
2/16/2018Assign the MFTI Priority 18 yo G1P0 37.3 weeks Denies ctx, unsure ifwater broke, pain 0 Initial BP 146/74 Denies preeclampsia sx Repeat BP 10 min later130/72 Other VS and FHR WNL 2013 AWHONN43Assign the MFTI Priority 32 yo G2P001023 weeksVS and FHR WNLStates she doesn’t feelctx or tightening, activeFM, no c/o Sent from office withshort cervix, no ctx forfurther monitoring 2013 AWHONN4422
2/16/2018Assign the MFTI Priorityfor Ms. L 32 yo, G3P2002 35.4 weeks c/o severe, constantupper abdominal pain(9/10), sweating c/o H/A (5/10), deniesvisual changes Says maybe mild ctx BP 144/88, P 122, R 20,T 98.9, FHR 150sThere may be more than onereason for your answer!@2015 AWHONN45Benefits of the MFTIfor Ms. L Attention to abnormalvital sign (BP 144/88,pre-eclampsia sx, P 122) Attention to non-ctxpain (9/10) Timely evaluation Elimination of cognitivebias@2015 AWHONN4623
2/16/2018AWHONN’s Perinatal NursingQuality Measure on Triage“The goal is that 100% ofpregnant patientspresenting to the laborand birth unit with areport of a real orperceived problem or anemergency condition willbe triaged .within 10minutes of arrival.”Learn more at:https://www.awhonn.org/awhonn/content.do?name 02 PracticeResources/02 perinatalqualitymeasures.htm 2014 AWHONNAWHONN’s MFTI Communities Over 120 hospitals participating, 2016 and2017 Peer support and AWHONN mentoring forimplementation of the MFTI Integrated MFTI into EMR or used on paper Educated nursing staff with AWHONN’s online,interactive MFTI module@2015 AWHONN4824
2/16/2018Lessons from AWHONN’s MFTICommunities1. Educate nursing staff on triage/MFTI2. Form a steering committee-multidisciplinary3. Identify shift champions4. Educate providers—grand rounds5. Identify a location for triage, if needed6. Implement the MFTI (paper or EMR)-trial7. Audit to promote correct use of MFTI Conclusions to date: education well-received,implementing MFTI is catalyst for overall triageimprovements@2015 AWHONN49MFTI Community Chart Audits Most discrepancies in priority assignmentplaced woman at lower priority than MFTIindicated– Abnormal vital signs– Preterm ctx or LOF– Decreased fetal movement– Non-labor pain 7 or above@2015 AWHONN5025
2/16/2018Quality Triage Care1. No women waiting , untriaged2. Classify all women’s acuity3. Implement standardized approach to triage,evaluation and escalation@2015 AWHONN51Questions? For clinical questions about the MFTI contactCatherine Ruhl at cruhl@awhonn.org For questions about the MFTI educationalmodule and implementation communities,contact Mitty Songer at msonger@awhonn.org26
OB Triage Education Trinity Health System reports in 2015: – 5% of OB RN Directors using an acuity tool OB triage. –None of the 35 birthing hospitals use a standardized education program to orient RNs to the role of the OB triage nurse. –Majority of hospitals assign RNs to wor