Transcription
Continuing EducationVolume 33 No. 2 Page 106How to Optimize an ExistingRemovable Partial DentureUsing Narrow-Diameter Implants toIncrease Support and RetentionAuthored by Steven H. Pratt, DDSUpon successful completion of this CE activity 1 CE credit hour will be awardedOpinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention ofspecific product names does not infer endorsement by Dentistry Today. Information contained in CE articles andcourses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged tocontact their state dental boards for continuing education requirements.
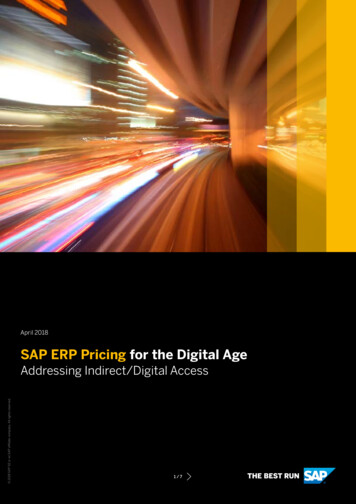
Continuing EducationHow to Optimize an ExistingRemovable Partial DentureUsing Narrow-Diameter Implants toIncrease Support and RetentionEffective Date: 2/1/2014Figure 1. Thepatient’s “do-ityourself” repair,done with a kitpurchased atWalmart.Expiration Date: 2/1/2017ABOUT THE AUTHORDr. Pratt received his DDS from theUniversity of Texas Health ScienceCenter at San Antonio in 1981 andbegan private practice that year in hishometown of Atlanta, Tex. He beganplacing and restoring dental implants in1988. Today, his practice offers all phases of generaldentistry, including comprehensive surgical and restorativephases of implant dentistry. Dr. Pratt holds Fellowships fromthe AGD, the American Academy of Implant Dentistry, andthe International College of Dentists. He has attended6 world symposiums on dental implants in 5 foreigncountries. He has had several of his implant casespublished in national journals and has spoken on thesubject of dental implants to educate both the public and hispeers in the practice of general dentistry. He has also beeninvolved with the Texas Dental Association’s Texas Missionsof Mercy and Smiles on Wheels where he has donated hisservices to those in need. He can be reached via e-mailat stenorpra@att.net.Figure 2. Resorbedlower posterior archwith insufficientbone width to placestandard sizedimplants withoutgrafting.Figure 3. Theexisting lower partialframework fit well.Disclosure: Dr. Pratt has no financial interest in any of thecompanies mentioned in this article, but did receivecompensation from ZEST Anchors for writing this article.dentures (RPDs).2 Recently, when this author polled anaudience of surgeons who place implants and dentists whoroutinely restore implants, only 20% stated that they hadused dental implants to help retain/support RPDs.This utilization of dental implants can easily beincorporated into general and prosthodontic dentalpractices to aid the numerous patients who otherwise mightnot be able to function optimally and comfortably with theirRPDs. Among the reasons patients often choose an RPDover other restorative options are financial or healthINTRODUCTIONAlthough dental implants are now widely used forsupporting fixed prostheses and retaining or supportingcomplete dentures, their use in North America is stillminimal when compared to the proven need.1 A review ofthe literature reveals that dental implants are not nearly aswidely used for supporting or retaining removable partial1
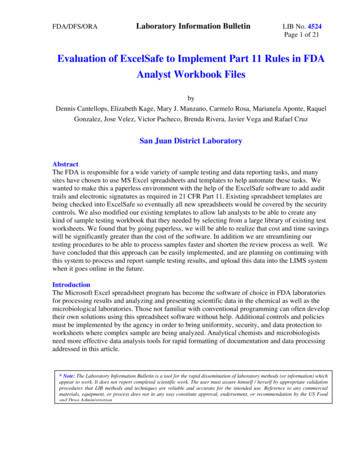
Continuing EducationHow to Optimize an Existing Removable Partial Dentureconcerns, lack of a distal abutment for a fixedpartial denture, or lack of desire to commit tothe time involved with bone grafting andsubsequent implant placement for a fixedprosthesis.Unfortunately, what patients usually donot realize is that an RPD, especially amandibular Kennedy Class I or II prosthesis,can actually cause severe bone lossthroughout time. In conjunction with an upper Figure 4. Panoramic radiograph reveals sufficient height to place 12-mm and 10-mmimplants in first premolar and second molar sites, respectively.complete denture, the Kennedy Class Iprosthesis is known to contribute tocombination syndrome first described byKelly3 in 1972. This bone loss can beprevented or minimalized under a new RPD,or slowed or eliminated under an existingRPD, with the use of dental implants.In many cases, if a patient has beenwearing an RPD for a while, the bone lossmentioned above may be severe enough thatFigure 5. Diagnostic model with drill guidesFigure 6. Vacuum-formed .060 surgicalstandard-sized implants cannot be placed placed, ready for .060 thermoformedstent trimmed and ready for sterilization.without bone grafting, which can be both surgical stent material.expensive and time consuming. If the patienthas insufficient bone for standard-sizedimplants and cannot afford or doesn’t want topursue bone-grafting procedures, smalldiameter implants (SDIs) may be the implantsof choice. Since FDA approval for “long-termintrabony applications” in 1997, SDIs havegrown in use and public awareness.4For many patients, SDIs offer severalbenefits over standard-sized implants. Theycan often be placed with no or minimal soft- Figure 7. The LOCATOR OverdentureFigure 8. The 2-piece design of the LODItissue reflection. They can be placed in Implant (LODI) (ZEST Anchors) can save as allows the clinician to easily replace themuch as 3 mm of vertical height over an oLOCATOR abutment (ZEST Anchors), ifnarrower ridges than standard-sized implants ball type attachment.attachment wear occurs throughout time.without bone grafting. Small-diameter implantscan often be placed at a fraction of the cost of standard-sizedCASE REPORTimplants, even though 2 SDIs are typically placed in the placeDiagnosis and Treatment Planningof one standard-sized implant.A 70-year-old female presented with a chief complaint of aThe following is a case in which a patient with a typicalbroken maxillary denture. While out of town, she attemptedmandibular Kennedy Class I RPD was unable and unwillingto repair the fractured denture with a denture repair kit thatto wear her partial due to its mobility while eating. SDIswas purchased at Walmart (Figure 1). She gave a history ofwere utilized to correct this problem.having “3 upper dentures made in as many years.” She said2
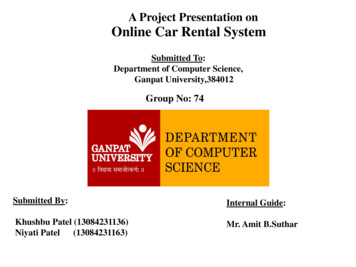
Continuing EducationHow to Optimize an Existing Removable Partial DentureFigure 9. Surgical stent “snapped” intoplace by engaging undercuts on teeth Nos.22 to 27, utilized at this time to markosteotomy sites with 1.2-mm pilot drill.Figure 10. Small flaps reflected to conserveattached gingiva.Figure 11. Paralleling pins in place afterosteotomies prepared. Site No. 31 angledbuccally to avoid lingual undercut.Figure 12. Closure obtained with 4-0Cytoplast PTFE sutures (OsteogenicsBiomedical).Figure 13. Immediate post-op panoramicradiograph.Figure 14. Two weeks post-op, immediatelyafter suture removal.framework fit the existing teeth very well (Figure 3). A panoramicradiograph revealed that there was sufficient bone height in theposterior mandible to place 12-mm implants in the first bicuspidsites and 10-mm implants in the second molar sites (Figure 4).It was explained to the patient that she seemed to be anexcellent candidate for narrow-diameter implants to helpsupport and retain her loose (but otherwise well fitting) lowerpartial. A treatment plan was presented to her that consistedof a new maxillary denture, 4 narrow diameter implants in theposterior mandible, and rebasing her existing partialframework. The patient accepted this treatment plan and wasready to get started as soon as her work schedule allowed.that all 3 had broken in the anterior region and anteriorteeth had broken out of them. Since she did not sleep withher denture in, she attributed this problem to the fact thather lower RPD was loose and always came out when shewas trying to eat. For this reason, she did not wear herlower partial, chewing only with her lower natural teeth(teeth Nos. 22 to 27).Her medical history revealed that she was on a bloodpressure medication, which controlled her blood pressurewithin normal limits. No other significant findings were noted.Clinically, the maxillary arch was fairly well preserved withoutthe significant anterior resorption that is usually seen in cases inwhich lower anterior teeth oppose a maxillary denture.Edentulous areas in the lower arch were resorbed to the extentthat placing standard-sized implants would be impossiblewithout bone grafting. However, there appeared to be sufficientbone to place narrow-diameter implants (Figure 2). Although herlower partial was not retentive enough for her to eat with, theTreatment ProtocolImpressions were made for diagnostic casts and for thefabrication of a surgical stent to aid in the placement of themandibular implants (Figures 5 and 6). Whenever possible,this author prefers to use a restrictive surgical stent to allow3
Continuing EducationHow to Optimize an Existing Removable Partial DentureFigure 15. Alginate pick-up impression ofthe lower partial rebase impression.Figure 16. Black processing males andmetal housings placed on LOCATORabutments.for precise placement of parallel implants.The implant of choice for this application was theLOCATOR Overdenture Implant (LODI) (ZEST Anchors). Available in diameters of 2.4 mm and 2.9 mm, the 2.4-mm diameterimplant was ideal for this patient’s thin ridges. The LODI waschosen instead of mini implants with a ball attachment dueto the need for decreased vertical height (Figure 7). Thisauthor has used the LOCATOR Abutment on standardsized implants for years, preferring the varying degrees ofretention that are available versus the retention offered withball type attachments. The LODI was also chosen over a onepiece clone of the LODI due to the fact that the abutment canwear throughout time, especially if patients are not meticulousabout rinsing abrasive toothpaste from both their mouth andthe intaglio surface of their prosthesis. The LODI, being a 2piece implant, allows for changing worn abutments at a laterdate (Figure 8).At the surgical appointment, local anesthesia wasobtained by infiltrating around each site buccally and linguallywith a total of 3 carpules of articaine 4% with 1/100,000epinephrine. The surgical stent was placed, and osteotomysites were marked through the gingiva using the 1.2-mm pilotdrill (Figure 9). The stent was then removed and, in order toretain as much attached gingiva as possible, small flaps weremade and reflected (Figure 10). The stent was then replacedand osteotomies were made using the appropriate drills anddrillstops. The osteotomy for site No. 31 had to be angledslightly buccally to avoid a lingual concavity of the mandible inthat area (Figure 11). LODI Implants were then placed; 2.4mm x 12-mm LODIs in the first bicuspid areas and 2.4-mm xFigure 17. Rebased partial with lingual ventholes allowing escape of excess acrylicwhile picking up LOCATOR males.Figure 18.Intaglio surface oflower partial withthe appropriateLOCATOR malesin place.10-mm LODIs in the second molar regions. Insertion torquefor each implant was recorded. All implants seated with aninsertion torque of slightly greater than 30 Ncm (except No.18, which seated to greater than 70 Ncm). Flaps were closedwith 4-0 Cytoplast PTFE sutures (Osteogenics Biomedical)(Figure 12) and a postoperative panoramic image was made(Figure 13). The patient’s partial was relieved to ensure therewas no contact with the LODI Abutments.At the 2-week post-op appointment, sutures wereremoved (Figure 14) and the final impression for themaxillary complete denture was made. Three days later,occlusion rim adjustments, bite records, and a rebaseimpression for the partial were made (Figure 15).At the delivery appointment, which was 2 weeks later,both the upper and lower prostheses were checked forpressure spots using pressure indicator paste (a 50/50mixture of zinc oxide powder and Crisco). After pressureareas were adjusted, vents were cut through the lingualsurface of the lower partial and the LOCATOR housings4
Continuing EducationHow to Optimize an Existing Removable Partial Denturecontaining the black processing males were captured withself-cure acrylic (Figures 16 and 17). Blue, 2-poundattachments were placed in housings corresponding to allparallel implants and a red, 2-pound extended range malewas placed in housing No. 31 due to the implant having anangulation greater than 10 (Figure 18).At the 24-hour post-delivery appointment, minor ad justments were made to the anterior labial and left posteriorbuccal flanges of the maxillary denture. The right buccalflange of the lower partial also required adjustment. At theone-week postoperative check, the patient reported thatshe was very satisfied with her result. She stated that, forthe first time since having her partial, she was able to eatcomfortably with it. When Brenda was asked if she mindedtaking a portrait image for this article, she stated,“Absolutely not, if it might help someone else as much asyou’ve helped me” (Figure 19).Figure 19.Brenda’s post-opsmile.REFERENCES1. Christensen GJ. Dental implants: Where do we go from here?Clinicians Report. 2013;6:1-2.2. Silva MAB, Consani RLX, Oliveira GJPL, et al. Associationbetween implants and removable partial dentures: review of theliterature. RSBO. 2011;8:88-92.3. Kelly E. Changes caused by a mandibular removable partialdenture opposing a maxillary complete denture. J Prosthet Dent.1972;27:140-150.4. Christensen GJ, Child PL. The truth about small diameterimplants. Dent Today. 2010;29:116-120.CLOSING COMMENTSPatients with RPDs are often overlooked as candidates fordental implants, unless they are willing to discard their RPDfor a more expensive fixed implant-supported alternative.This case clearly exemplifies how a patient with anunsatisfactory but otherwise well fitting RPD can benefitfrom strategically placed small-diameter implants thatvirtually change a Kennedy Class I RPD into a KennedyClass III RPD. The LOCATOR attachments also offer ex cellent retention of the RPD.Placement of SDIs can be a more economical choice forthe patient who might otherwise need bone grafting to placestandard size implants. In this case, and similar KennedyClass I cases, the patient, with the aid of dental implants,may very well be able to avoid the effects combinationsyndrome and its consequences as one ages.5
Continuing EducationHow to Optimize an Existing Removable Partial DenturePOST EXAMINATION INFORMATIONPOST EXAMINATION QUESTIONSTo receive continuing education credit for participation inthis educational activity you must complete the programpost examination and answer 4 out of 5 questions correctly.1. A review of the literature reveals that dental implantsare now widely used for supporting or retainingremovable partial dentures (RPDs).a. TrueTraditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the postexam (answer 4 out of 5 questions correctly), a letter ofcompletion will be mailed to the address provided.b. False2. Bone loss can be prevented or minimalized under anew RPD, or slowed or eliminated under an existingRPD, with the use of dental implants.a. Trueb. False3. Since FDA approval for “long-term intraboneyapplications” in 1997, small-diameter implants (SDIs)have grown in use and public awareness.a. TrueOnline Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submittingthe form, your Letter Of Completion will be providedimmediately for printing.b. False4. Patients with RPDs are often overlooked ascandidates for dental implants, unless they arewilling to discard their RPD for a more expensivefixed implant-supported alternative.a. Trueb. False5. Placement of SDIs can be a more economical choicefor the patient who might otherwise need bonegrafting to place standard size implants.a. TrueGeneral Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.6b. False
Continuing EducationHow to Optimize an Existing Removable Partial DenturePROGRAM COMPLETION INFORMATIONPERSONAL CERTIFICATION INFORMATION:If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer 4 of the 5questions correctly.Last NameFirst NameProfession / CredentialsSuite or Apartment NumberTRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:CityDentistry TodayZip CodeFax Number With Area CodeFax: 973-882-3622E-mail AddressPAYMENT & CREDIT INFORMATION:ANSWER FORM: VOLUME 33 NO. 2 PAGE 106Examination Fee: 20.00 Credit Hours: 1Please check the correct box for each question below.Note: There is a 10 surcharge to process a check drawn onany bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.1. o a. Trueo b. False3. o a. Trueo b. False2. o a. TrueI have enclosed a check or money order.4. o a. TrueI am using a credit card.5. o a. TrueMy Credit Card information is provided below.o American Express o Visa o MC o DiscoverPlease provide the followingStateDaytime Telephone Number With Area CodeDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004oLicense NumberStreet AddressComplete online at: dentalcetoday.como(PLEASE PRINT CLEARLY OR TYPE)o b. Falseo b. Falseo b. FalsePROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.(please print clearly):Rating Scale: Excellent 5 and Poor 0Course objectives were achieved.Exact Name on Credit CardContent was useful and benefited your clinical practice.Review questions were clear and relevant to the editorial./Credit Card #Illustrations and photographs were clear and relevant.Expiration DateWritten presentation was informative and concise.How much time did you spend reading the activity andcompleting the test?SignatureWhat aspect of this course was most helpful and why?This CE activity was not developed in accordance withAGD PACE or ADA CERP standards.CEUs for this activity will not be accepted by the AGDfor MAGD/FAGD credit.What topics interest you for future Dentistry Today CE courses?7
Removable Partial Denture Using Narrow-Diameter Implants to Increase Support and Retention Effective Date: 2/1/2014 Expiration Date: 2/1/2017 Figure 2. Resorbed lower posterior arch with insufficient bone width to place standard sized implants without grafting. Figure 3. The existing lower partial