Transcription
Wu et al. BMC Cancer(2021) ESEARCHOpen AccessThe long-term survival outcomes of gastriccancer patients with total intravenousanesthesia or inhalation anesthesia: asingle-center retrospective cohort studyWei-Wei Wu1†, Wei-Han Zhang2†, Wei-Yi Zhang1, Kai Liu2, Xin-Zu Chen2, Zong-Guang Zhou2, Jin Liu1,Tao Zhu1† and Jian-Kun Hu2*†AbstractBackground: The relationship between the type of anesthesia and the survival outcomes of gastric cancer patientsis uncertain. This study compared the overall outcome of gastric cancer patients after surgery with total intravenousanesthesia (TIVA) or inhalation anesthesia (IHA).Methods: Clinicopathological variables of gastric cancer patients were retrieved from the database of the SurgicalGastric Cancer Patient Registry in West China Hospital, Sichuan University. Patients were grouped according towhether they received TIVA or IHA during the operation. Propensity score (PS) matching was used to balance thebaseline variables, and survival outcomes were compared between these two groups. In addition, studiescomparing survival outcomes between TIVA and IHA used for gastric cancer surgery and published before April20th, 2020, were identified, and their data were pooled.Results: A total of 2827 patients who underwent surgical treatment from Jan 2009 to Dec 2016 were included.There were 323 patients in the TIVA group and 645 patients in the IHA group, with 1:2 PS matching. There was nosignificant difference in overall survival outcomes between the TIVA and IHA groups before matching the cohort(p 0.566) or after matching the cohort (p 0.679) by log-rank tests. In the Cox hazard regression model, there wasno significant difference between the TIVA and IHA groups before (HR: 1.054, 95% CI: 0.881–1.262, p 0.566) orafter (HR: 0.957, 95% CI: 0.779–1.177, p 0.679) PS matching. The meta-analysis of survival outcomes between theTIVA and IHA groups found critical statistical value in the before PS matching cohort (HR 0.74, 95% CI: 0.57–0.96p 0.01) and after PS matching cohort (HR: 0.65, 95% CI: 0.46–0.94, p 0.01).* Correspondence: hujkwch@126.com†Wei-Wei Wu and Wei-Han Zhang contributed equally to this work.†Tao Zhu and Jian-Kun Hu jointly supervised this work.2Department of Gastrointestinal Surgery and Laboratory of Gastric Cancer,State Key Laboratory of Biotherapy, West China Hospital, Sichuan University,and Collaborative Innovation Center for Biotherapy, No. 37 Guo Xue Street,Chengdu, Sichuan Province, ChinaFull list of author information is available at the end of the article The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver ) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
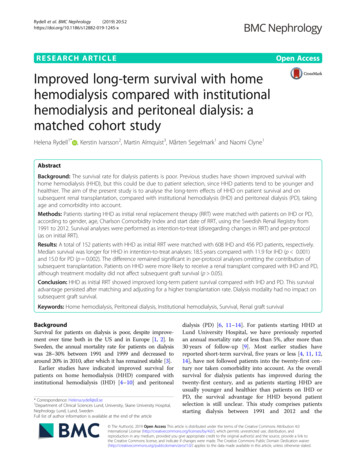
Wu et al. BMC Cancer(2021) 21:1193Page 2 of 12Conclusions: Combined with the results of previous studies, total intravenous anesthesia has been shown to besuperior to inhalation anesthesia in terms of overall survival for gastric cancer patients undergoing surgicaltreatment. The selection of intravenous or inhalation anesthesia for gastric cancer surgery should take into accountthe long-term prognosis of the patient.Keywords: Gastric cancer, Anesthesia, Intravenous, Inhalation, PrognosisIntroductionGastric cancer is one of the most common malignantdiseases of the digestive system, especially in East Asiancountries [1, 2]. Radical surgical treatment with perioperative chemotherapy is the major treatment choiceaccording to the latest treatment guidelines [3, 4]. Several clinicopathological variables, such as macroscopictype, Lauren classification, differentiation degree of thetumor, tumor stage, resection degree, resection patterns,and lymphadenectomy degree, are independent prognostic factors of gastric cancer patients [5, 6].In the perioperative period, both surgical stress andanesthetics may influence cell-mediated immunity andhumoral immunity by influencing the functions of immune competent cells and inflammatory mediator secretion, resulting in immunosuppression. Meanwhile,immunosuppression attributable to anesthetics may accelerate the growth and metastases of cancer cells andresult in poor survival of patients with malignant diseases [7]. In addition, anesthetics were found to suppressthe activity of natural killer cells and promote tumormetastasis in rat models [8]. Anesthetics can also resultin immunological suppression by influencing the function of natural killer cells, as shown in a clinical study ofbreast cancer patients sthesia has been found to have fewer immunosuppressive effects than sevoflurane-based or desfluranebased inhalation anesthesia. Previous studies haveshown that survival outcomes are significantly betterin prostate cancer and colon cancer patients who receive propofol-based total intravenous anesthesia thanin those who receive desflurane-based inhalationanesthesia [10, 11]. However, the debate regarding theinfluence of anesthesia types on the long-term survival outcomes of patients with malignant disease hasnot been settled. For example, some studies reportedno relevance of the type of anesthesia for the prognosis of patients with breast cancer [12, 13]. However,paradoxical survival outcomes have been reported between total intravenous anesthesia and inhalationanesthesia in gastric cancer patients [14–16].Therefore, we performed this single-center retrospective cohort study with a large sample size and adjustedfor the clinicopathological prognostic characteristics bythe propensity score (PS) matching method betweentotal intravenous anesthesia (TIVA) and inhalationanesthesia (IHA). The purpose of this study was to assess the relationship between types of anesthesia andlong-term overall survival outcomes after gastric cancersurgery.MethodsData availableWe collected data from the database of the Surgical Gastric Cancer Patient Registry in West China Hospital withthe registration number WCH-SGCPR-2020. The establishment of this database was approved by the Biomedical Ethical Committee of the West China Hospital,Sichuan University, China (No. 2014–215). Patient records and personal information were deidentified beforestatistical analysis.Patients who underwent surgical treatment from Jan1st, 2009 to Dec 31st, 2016 in the WCH-SGCPR database were screened [17, 18]. We included primary gastric cancer patients who underwent surgical resection,with complete intraoperative anesthesia information andpostoperative follow-up information (updated to Jan 1st,2020). Patients with a history of other malignant diseases, preoperative chemotherapy or radiotherapy wereexcluded from the present study. The selection of thepatients is presented in Fig. 1.Anesthesia methodThe choice of anesthesia type was determined by thecharacteristics of the patients and the preference ofthe responsible anesthesiologists, and usually choosethe type they are better at. In the present study, thepatients were divided into the TIVA group and theIHA anesthesia group according to the anesthesiamethods. In both the TIVA and IHA groups,anesthesia was induced with midazolam 0.05–0.15 mg/kg, 0.3 μg/kg sufentanil, and 1–2.5 mg/kg propofol.The maintenance dose of anesthesia was propofol 3mg/(kg*h) or sevoflurane 1 2% and remifentanil 0.1 0.2 μg/(kg*min). For patients with total intravenousanesthesia, anesthesia was maintained with propofoland remifentanil infusion. For patients with inhalationanesthesia, anesthesia was maintained with sevoflurane or desflurane inhalation and remifentanil infusion.Patient-controlled analgesia was recommended for allgastric cancer patients who underwent surgical
Wu et al. BMC Cancer(2021) 21:1193Page 3 of 12Fig. 1 Flow chart of patients’ selectiontreatment in our hospital and they received a totaldose of 3 μg/mL fentanyl or 0.5 μg/mL sufentanil for72–120 hpostoperatively.Nonsteroidalantiinflammatory drugs (NSAIDs), flurbiprofen axetil orparecoxib sodium were used as rescue solutions during the postoperative recovery period and the hospitalstay.Surgical treatment methodAll of the included patients underwent surgical treatment in the Department of Gastrointestinal Surgery,West China Hospital, Sichuan University. A radical operation with curative intent was performed according tothe Japanese Gastric Cancer Treatment Guidelines [3].Total or subtotal gastrectomy was performed accordingto the tumor stage, tumor location and status of the regional lymph nodes. Intraoperative frozen sections wereroutinely performed to secure safe resection margins.There were no limitations on the reconstructionmethods.Clinicopathological characteristicsThe following clinicopathological information was alsoretrieved from the database: age (years), sex (male orfemale), tumor size (cm), Borrmann type (Type I-IV),differentiation degree (well, moderate, poor and undifferentiated), tumor location (adenocarcinoma of theesophagogastric junction (AEG) and non-AEG), operation type (laparoscopic surgery and open surgery),radical degree (R0, R1, and R2), lymphadenectomy degree (D1, D1 , D2, and D2 ), operation time (minutes), blood loss (ml), pathological tumor stage (pT,pN and pTNM), number of positive and examinedlymph nodes, postoperative nonsteroidal antiinflammatory drug (NSAID) use, adjuvant chemotherapy and postoperative recovery course (complicationsand hospital stay). For the clinicopathological variables, the pathological examination was performed bypathologists of the Department of West China Hospital, Sichuan University according to the AJCC 8thstaging manual [19].
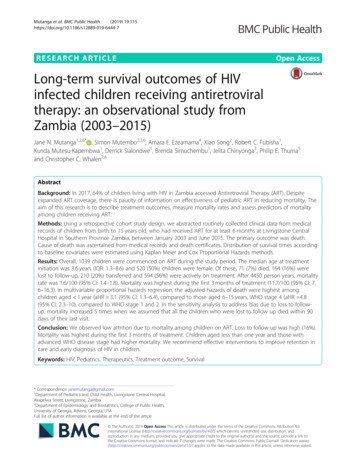
Wu et al. BMC Cancer(2021) 21:1193Page 4 of 12Follow-up informationStatistical analysisPostoperative follow-up was scheduled for each gastriccancer patient who underwent treatment in our department. We recommended at least two outpatient followups in the first 3 years and at least one outpatientfollow-up in subsequent years. At each outpatient visit, aphysical examination, serum tumor markers (CEA,CA19–9, CA125, CA72–4), and enhanced computedtomography (chest and abdominal) were essential tests.Follow-up information was updated to Jan 1st, 2020.The main reasons for patients lost to follow-up were refused to attend the outpatient visits or changes in contact information. Of the 2966 patients eligible foranalysis, 139 patients were lost to postoperative followup, so the follow-up rate was 95.3% (2827/2966), with a48.8 (23.3–77.4) month median follow-up duration.Continuous variables with a non-normal distribution areexpressed as the median and interquartile range (IQR,25–75%); categorical variables are expressed as numbers(%). The Mann–Whitney U test was used to analyzecontinuous variables and ordinal categorical variables,whereas the chi-square test was used for unordered categorical variables. Variables that yielded p 0.1 in univariate survival analysis were considered candidates inthe multivariate Cox-hazard model. A P value 0.05 (2sided) was defined as statistically significant.For patients in the TIVA group, propensity scoreswere computed as the conditional probability using a logistic regression model that included baseline characteristics (age, sex, tumor location, operation type, radicaldegree, lymphadenectomy degree, pT stage, pN stage,pM stage, and adjuvant chemotherapy) to achieve balance in covariates between the TIVA and IHA groups.Propensity score matching pairs were identified withoutreplacement using a 1:2 nearest neighbor matching algorithm with caliper width determined by the recommendation (0.001 of the standard deviation of the logit) [20].The balance of covariates between the TIVA and IHAgroups was assessed by the standardized mean difference(SMD). An SMD 0.1 indicated a good balance in thecovariates between the two groups. All statistical analyses were conducted using R Software (http://www.Rproject.org/), including the “survival”, “survminer”,“ggplot2”, “nonrandom”, “MatchIt”, “meta” and “metafor” packages.Considering that this is a retrospective study, we calculated the statistical power via PASS 11 (Version11.0.7).Meta-analysis between intravenous and inhalationanesthesia methods of gastric cancer surgeryA comprehensive literature search was performed inthe Cochrane Library (January 1, 2005 to November25, 2020), MEDLINE via PubMed (January 1, 1966to November 25, 2020) and EMBASE (January 1,1974 to December 02, 2020) using the terms “gastriccancer”, “gastric carcinoma”, “gastric neoplasm”,“stomach cancer”, “stomach carcinoma”, “stomachneoplasm”, “inhalation, anesthesia”, “insufflation”,“volatile”, “intravenous, anesthesia”, “infusion”, “surgery” and “operation”. Previously published metaanalyses and systematic reviews were also searchedfor relevant articles. Relevant articles were also retrieved by manually checking the reference lists ofthe retrieved articles. Titles, abstracts, and subsequently full-text articles were screened by two authors (WW Wu and WH Zhang). We only includedstudies comparing survival outcomes between totalintravenous anesthesia and inhalation anesthesiamethods of gastric cancer surgery. Review articles,case reports, articles in languages other than English,and articles with incomplete or duplicated data wereexcluded.Data from the included studies were independentlyextracted by two authors (WH Zhang, WW Wu). Foreach study, we recorded the name of the first author,year of publication, country, study design, and periodof the included patients. The following variables werealso extracted: age (mean SD), sex, tumor stage andsurvival outcomes (hazard ratio, HR; 95% confidenceintervals, 95% CI). The meta-analysis of survival outcomes was performed by the random-effects methodaccording to the Cochrane guidelines. We evaluatedall included studies for quality with the NewcastleOttawa Scale (NOS), and all studies were rated aminimum of 5 points.ResultsPatient characteristics before and after propensity scorematchingA total of 3426 patients underwent treatment in theDepartment of Gastrointestinal Surgery, West ChinaHospital, Sichuan University from January 2009 toDecember 2016. According to the inclusion criteria andexclusion criteria, 2827 patients were included in thefinal analysis, 344 patients with total intravenousanesthesia were in the TIVA group, and 2483 patientswith inhalation anesthesia were in the IHA group. Theclinicopathological and intraoperative characteristics ofthe patients were compared between the TIVA and IHAgroups before and after propensity score matching, andthe results are presented in Table 1. Before PS matching,tumor size, operation type, radical degree, blood loss,pTNM stage, numbers of examined, positive lymphnodes were unbalanced between the TIVA and IHAgroups (p 0.05 and SMD 0.1). After the 1:2 PSmatching procedures, 323 patients in the TIVA group
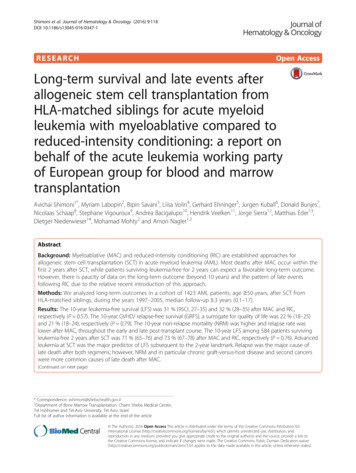
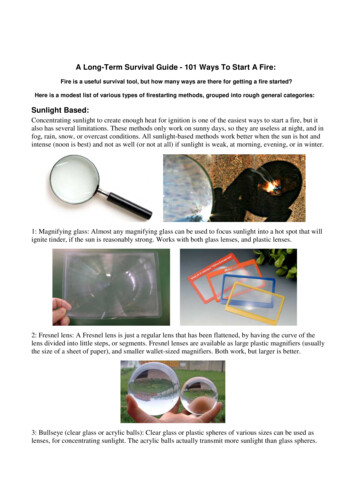
Wu et al. BMC Cancer(2021) 21:1193Page 5 of 12Table 1 Clinicopathological characteristics between TIVA group and IHA group, before and after propensity-score matchCharacteristicsAge, median (IQR)TIVA groupN 323 (%)YearsIHA groupN 2264 (%)60.0 [51.0, 66.0] 59.00 [50.0,66.0]PvalueSMD TIVA groupN 344 (%)PvalueSMD0.6280.035 60.0 [51.0, 66.0] 60.0 [51.0, 67.0] 0.9670.018IHA groupN 688 (%)GenderFemale102 (31.6)671 (29.6)0.5170.042 102 (31.6)205 (31.8)10.004Tumor Size, median (IQR)cm4.0 [3.0, 6.0]5.0 [3.0, 6.0]0.0120.152 4.0 [3.0, 6.0]4.0 [3.0, 6.0]0.4350.065Borrmann TypeType III-IV131 (40.6)916 (40.5)10.002 131 (40.6)238 (36.9)0.3010.075Differentiated DegreeG3-G4260 (80.5)1812 (80.0)0.9050.012 260 (80.5)521 (80.8)0.9860.007Tumor LocationNon-AEG74 (22.9)619 (27.3)0.1060.102 74 (22.9)145 (22.5)0.9450.010Operation TypeLaparoscopic 29 (9.0)318 (14.0)0.0160.159 29 (9.0)73 (11.3)0.3140.078Radical DegreeR1/R24 (1.2)103 (4.5)0.0080.198 4 (1.2)6 (0.9)0.9120.03Lymphadenectomy DegreeD2/D2 291 (90.1)1991 (87.9)0.3030.069 291 (90.1)580 (89.9)10.006Operation Time, median (IQR)min230.0 [205.0,260.0]235.0 [205.0,270.0]0.3680.067 230.0 [205.0,260.0]230.0 [200.0,265.0]0.9280.007Blood Loss, median (IQR)ml100.0 [50.0,105.0]100.0 [80.0,150.0]0.0320.147 100.0 [50.0,105.0]100.0 [80.0,200.0]0.0880.126pT stageT168 (21.1)491 (21.7)0.2420.120 68 (21.1)140 (21.7)0.5150.102T257 (17.6)328 (14.5)57 (17.6)126 (19.5)T373 (22.6)460 (20.3)73 (22.6)120 (18.6)T4125 (38.7)985 (43.5)125 (38.7)259 (40.2)N0126 (39.0)771 (34.1)0.143 126 (39.0)256 (39.7)0.9170.048N160 (18.6)372 (16.4)60 (18.6)108 (16.7)N252 (16.1)417 (18.4)52 (16.1)106 (16.4)N385 (26.3)704 (31.1)I92 (28.5)575 (25.4)0.9620.019II91 (28.2)III140 (43.3)2.0 [0.0, 8.0]pN stagepTNM stage0.12585 (26.3)175 (27.1)0.161 92 (28.5)189 (29.3)529 (23.4)91 (28.2)178 (27.6)1160 (51.2)140 (43.3)278 (43.1)0.026No. of Positive LNs, median (IQR)numbers2.0 [0.0, 7.0]0.8060.034No. of Examined LNs, median(IQR)numbers26.0 [19.5, 35.0] 27.0 [20.0, 37.0] 0.0650.159 26.0 [19.5, 35.0] 26.0 [20.0, 36.0] 0.6700.066Perioperative NSAIDsUse6 (1.9)0.045 6 (1.9)0.04357 (2.5)0.0130.5980.138 2.0 [0.0, 7.0]2.0 [0.0, 7.0]16 (2.5)0.701Adjuvant ChemotherapyYes183 (56.7)1370 (60.5)0.2070.078 183 (56.7)377 (58.4)0.6430.036Postoperative 30-daycomplicationsYes54 (16.7)411 (18.2)0.5820.038 54 (16.7)114 (17.7)0.7790.025Postoperative Hospital Stay,median (IQR)Days10.00 [9.00,12.00]10.00 [9.00,12.00]0.9920.031 10.00 [9.00,12.00]10.00 [9.00,12.00]0.8330.015Abbreviations: TIVA Total intravenous anesthesia, IHA Inhalation anesthesia, SMD Standardized mean difference, IQR Interquartile range, AEG Adenocarcinoma ofesophagogastric junction, LNs Lymph nodesand 645 patients in the IHA group had balanced clinicopathological covariates (p 0.05 and SMD 0.1). Thestandardized differences and distribution of the clinicopathological characteristics before and after propensityscore matching are shown in Fig. 2.Univariate and multivariate survival analysisFirst, we evaluated the survival outcomes between theTIVA and IHA groups, and there was no survival difference by the log-rank test between the TIVA and IHAgroups before PS matching (HR: 1.054, 95% CI: 0.881–1.262, p 0.566) and after PS matching (HR: 0.957, 95%CI: 0.779–1.177, p 0.679) (Figs. 3 and 4).Univariate and multivariate survival analyses of patients in the before and after PS matching cohorts wereanalyzed and are presented in Tables 2 and 3, respectively. In the multivariate survival analysis of before propensity score matching cohorts, age, tumor size,macroscopic type, radical degree, pathological TNMstage, and postoperative adjuvant chemotherapy were independent prognostic risk factors for overall survival.Additionally, in the multivariate survival analysis of
Wu et al. BMC Cancer(2021) 21:1193Page 6 of 12Fig. 2 Illustration of standardized differences in clinicopathological characteristics before and after propensity-score matching cohortspatients after the propensity score matching cohort, age,tumor size, radical degree, pathological TNM stage, andadjuvant chemotherapy were independent prognosticrisk factors for the overall survival outcomes. Most importantly, the anesthesia type (intravenous anesthesia orinhalation anesthesia methods) was not a significant riskfactor for overall survival outcomes in either the before(HR: 1.054, 95% CI: 0.881–1.262, p 0.566) or after propensity score matching cohorts (HR: 0.957, 95% CI:0.779–1.177, p 0.679).Subgroup analysisWe performed subgroup analyses on patients basedon their final pathological stage. Patients in both theTIVA and IHA groups had similar survival ratesacross pTNM stages (Figs. 3 and 4). Before PS match,for whole pTNM stage, the HR was 1.054 (95%CI:0.881–1.262), the propensity score-adjusted HR was0.957 (95%CI: 0.779–1.177). For pTNM-I, the HR was0.980 (95%CI: 0.556–1.728), the propensity scoreadjusted HR was 0.630 (95%CI: 0.442–1.639). ForpTNM-II, the HR was 0.369 (95%CI: 0.577–1.226),the propensity score-adjusted HR was 1.101 (95%CI:0.727–1.667). For pTNM-III, the HR was 0.995(95%CI: 0.798–1.240), the propensity score-adjustedHR was 0.901 (95%CI: 0.697–1.164).Meta-analysis between total intravenous and inhalationanesthesiaThrough the literature search, we found three publishedstudies that compared the survival outcomes betweenthe TIVA and IHA groups (Supplementary Fig. 1).Meanwhile, we added the survival outcomes of our studyto the meta-analysis. The general characteristics of thestudies are presented in Table 4. Both of the studiesused the propensity score matching method to balancethe clinicopathological characteristics between the TIVAand IHA groups. Therefore, a meta-analysis of survivaloutcomes was performed before and after PS matching(Fig. 5A and B). A critical statistical value was found inthe before (HR 0.74, 95% CI: 0.57–0.96, p 0.01) andafter (HR 0.65, 95% CI: 0.46–0.94, p 0.01) PS matchingcohort between the TIVA and IHA groups.DiscussionAccording to previous studies, conflicting conclusionshave been reported on the survival outcomes of totalintravenous anesthesia and inhalation anesthesia usedduring gastric cancer surgery [14–16]. However, in boththe before PS matching and after PS matching cohorts,there was no significant difference between TIVA andIHA in the overall survival outcomes of patients whounderwent gastric cancer surgery. In the further subgroup analysis, no statistical differences were found in
Wu et al. BMC Cancer(2021) 21:1193Page 7 of 12Fig. 3 Survival outcomes between TIVA and IHA groups and subgroup analyses before propensity-score matching cohorts (A. Survival rate for allTNM stages; B. Survival rate for TNM-I stage; C. Survival rate for TNM-II stage; D. Survival rate for TNM-III stage)the survival rates of patients at each stage. Meanwhile,we performed a pooled analysis of survival results frompreviously reported studies and our study to explorewhether anesthesia type can influence the survival outcomes of gastric cancer patients who underwent surgicaltreatment. A critical statistical value was found in thebefore and after PS matching cohort between the TIVAand IHA groups for overall survival outcomes.Although other perioperative treatment modalities,such as radiotherapy, may also affect tumor metastasis,the relationship between anesthetic techniques and theprognosis of cancer patients is one of the core concernsduring the process of making treatment strategy decisions for malignant diseases. Regional anesthesia, suchas epidural anesthesia, has positive implications in theprevention of immunosuppression and in reducing inflammation during the surgical treatment of malignantdiseases.Volatile agents are the most common method of maintaining general anesthesia worldwide. TIVA is primarilyadministered by propofol as an induction and maintenance agent. Propofol has been shown in in vitro
Wu et al. BMC Cancer(2021) 21:1193Page 8 of 12Fig. 4 Survival outcomes between TIVA and IHA groups and subgroup analyses in after propensity-score matching cohorts (A. Survival rate for allTNM stages; B. Survival rate for TNM-I stage; C. Survival rate for TNM-II stage; D. Survival rate for TNM-III stage)Table 2 Univariate and Multivariate survival analysis of patients before propensity-score match (N 2587)CharacteristicsUnivariateMultivariateHR95% CIP valueHR95% CIP valueAge, years 65 vs. 651.3071.157–1.477 0.0011.2171.075–1.3790.002GenderMale vs. Female0.9980.879–1.1330.978Tumor locationAEG vs. Non-AEG0.7230.638–0.819 0.0010.8820.777–1.0020.054Tumor size, cm 5 vs. 52.7142.388–3.084 0.0011.3521.168–1.566 0.001Macroscopic typeType 0–2 vs. Type 3–42.0801.850–2.338 0.0011.1641.026–1.3210.019Differentiate degreeG1–2 vs. G31.5171.291–1.782 0.0011.1050.935–1.3060.240Radical degreeR0 vs. R1/R23.0842.473–3.846 0.0011.9201.534–2.404 0.001Lymphadenectomy degreeD1/D1 vs. D2/D2 1.0350.869–1.2320.701pTNM stageI vs. II2.6012.048–3.304 0.0012.3161.803–2.974 0.001I vs. III6.5195.284–8.042 0.0014.9703.916–6.308 0.001Adjuvant chemotherapyNo vs. Yes0.8840.786–0.9950.0410.7150.634–0.807 0.001Anesthesia methodIVA vs. SAIDsNo vs. Yes1.1830.828–1.6910.355Abbreviations: HR Hazard ratio, CI Confidence interval, AEG Adenocarcinoma of esophagogastric junction, TIVA Total intravenous anesthesia, IHA Inhalationanesthesia, NSAIDs Nonsteroidal Anti-inflammatory Drugs
Wu et al. BMC Cancer(2021) 21:1193Page 9 of 12Table 3 Univariate and Multivariate survival analysis of patients after propensity-score match (N 1032)CharacteristicsUnivariateMultivariateHR95% CIP valueHR95% CIP value 0.0011.4211.159–1.7430.001Age, years 65 vs. 651.4621.198–1.785GenderMale vs. Female0.9550.774–1.1790.669Tumor locationAEG vs. 961Tumor size, cm 5 vs. 52.5132.052–3.077 0.0011.3821.100–1.7360.005Macroscopic TypeType 0–2 vs. Type 3–41.9631.615–2.386 0.0011.1180.903–1.3830.306Differentiate DegreeG1–2 vs. ical DegreeR0 vs. 63.2142.197–4.703 0.001Lymphadenectomy degreeD1/D1 vs. D2/D2 1.2200.883–1.6860.229TNM stageI vs. II3.4402.383–4.965 0.001I vs. III6.6914.775–9.376 0.0015.5693.834–8.089 0.001Adjuvant ChemotherapyNo vs. Yes0.8330.685–1.0130.0680.6930.567–0.847 0.0010.9460.769–1.1630.597Anesthesia methodIVA vs. IHA0.9570.779–1.1770.679NSAIDsNo vs. Yes0.5740.256–1.2850.177Abbreviations: HR Hazard ratio, CI Confidence interval, AEG Adenocarcinoma of esophagogastric junction, TIVA Total intravenous anesthesia, IHA Inhalationanesthesia, NSAIDs Nonsteroidal Anti-inflammatory Drugsexperiments to inhibit the expression of oncogenes andsuppress tumor angiogenesis, resulting in a lower recurrence rate [21–24].The survival impact of anesthetic and anesthesia typeused during the operation has been evaluated in severalmalignant diseases. Total intravenous anesthesia hasbeen found to be associated with significantly better survival outcomes than inhalation anesthesia for esophagealcancer patients [25]. In addition, in a large sample sizestudy of colon cancer patients, total intravenousanesthesia had better survival outcomes than inhalationanesthesia irrespective of the tumor-node-metastasisstage [11]. However, for patients who underwent breastcancer surgery, contradictory results were found in previous studies. A study showed that propofol-based TIVAhad a lower tumor recurrence risk than sevofluranebased IHA for breast cancer patients [26]. However, another existing studies found no significant difference indisease-free survival and overall survival between TIVAand IHA for breast cancer patients [12, 27]. TumorTable 4 General characteristics of study compare survival outcomes between total intravenous and inhalation anesthesiaAuthorCountry TimePeriodTumorStageOperationTypeMatchmethodPSNo. ofmatch PatientsOh et al.,2019KoreaI-IIIAJCC7thLap andOpen1:1 PSmatchBefore 816Gender(male)SurvivaloutcomeHR (95% CI)3791 58.3 12.4IHAIVA IHAIVA vs. IHA60.5 12.7564 2511 0.57 (0.37–0.88)After76959.3 12.7527 5270.92 (0.52–1.63)I-IIIAJCC7thOpenSurgeryBefore 1506 1350 NANA313 3170.61 (0.54–0.68)AfterI-IVNotmentionedTIVA IHAZheng et al.,2018Huang et al.,2019Wu et 162009–2016I-IIIAJCC8thLap andOpen1:1 PSmatch1:1 PSmatch1:2 PSmatch769Age (year)IVA58.7 12.4897897NANA159 1600.65 (0.56–0.75)Before 19021865 1466 15124 1500.47 (0.34–0.63)After16766 1465 15114 1160.56 (0.41–0.78)167Before 3232264 60.0 [51.0,66.0]59.00 [50.0,66.0]221 1593 1.05 (0.88–1.26)After64560.0 [51.0,67.0]221 44032360.0 [51.0,66.0]0.96 (0.78–1.18)Abbreviations: TIVA Total intravenous anesthesia, IHA Inhalation anesthesia, PS Propensity score, HR Hazard ratio, CI Confidence interval, NA Not applicableaThe present study
Wu et al. BMC Cancer(2021) 21:1193Page 10 of 12Fig. 5 Forest plot of survival outcomes among study compares intravenous anesthesia and inhalation anesthesia (A. Before propensity scorematching, B. After propensity score matching)heterogeneity and molecular characteristics are important explanations for the differential treatment outcomesof cancer patients [28, 29]. Whether these factors canhelp explain the different results among the differentcancer types with total intravenous anesthesia or inhalation anesthesia is unclear. Therefore, not only is there aneed for research on the relationship and mechanism ofanesthetic drugs and the immunological response, further study is expecting to analyze the effects ofanesthetic drugs on the expression levels of oncogenesor the regulation of the tumor microenvironment, corresponding functional changes of tumor biological behavior, and the survival outcomes of cancer patients.Specific to gastric cancer, only three studies have reported the influence of TIVA or IHA on the survivaloutcomes of surgical treatment [14–16]. Although thesestudies both used the PS matching method to balanceclinicopathological characteristics, their conclusionswere very different. Different tumor stages or surgicaltreatment strategies might be the reasons for the different survival outcomes between these two studies. For example, in the study of Oh et al., more than half of thepatients
The long-term survival outcomes of gastric cancer patients with total intravenous anesthesia or inhalation anesthesia: a single-center retrospective cohort study Wei-Wei Wu1†, Wei-Han Zhang2†, Wei-Yi Zhang1, Kai Liu2, Xin-Zu Chen2, Zong-Gua